
Abstract
The Occupational Self-Assessment version 2.2 (OSA) is a self-assessment of the client’s occupational competence and values. To describe the process of cross-cultural adaptation of OSA into Brazilian Portuguese (OSA-Brazil) and examine its reliability and validity for use with the Brazilian population. Assessment translation was guided by two international guidelines for cross-cultural adaptation of standardized instruments. Face validity was tested with 24 participants. Internal consistency, test–retest reliability, and convergent validity were tested with a convenience sample of 40 participants. The cross-cultural adaptation process concluded with a consensus among the expert panel review (r > 80%) and evidence of strong face validity. The OSA-Brazil demonstrated appropriate test–retest reliability (r > 0.70) and convergent validity with the 36-Item Short-Form Health Survey (SF-36) (p < .05). The OSA-Brazil has good face validity, test–retest reliability, and convergent validity. The assessment can be used by the Brazilian occupational therapists to assess client’s occupational competence.
Introduction
The Model of Human Occupation (MOHO) is a widely established theoretical model in the occupational therapy profession. From its inception, assessments that address multiple components were developed and tested to increase the practicality of clinical contexts with limited evaluation time. According to Kielhofner (2008), in clinical contexts with limited evaluation time, it is best to select an assessment that addresses multiple MOHO concepts to ensure a holistic view of the client’s lived experience. The basic MOHO concepts are volition (motivation for occupation), habituation (habits, and internalized roles), performance capacity (process, motor, and social interaction skills), and environment (Taylor & Kielhofner, 2017). Existing assessments that examine multiple MOHO constructs include the Model of Human Occupational Screening Tool, the Occupational Circumstances Assessment-Interview and Rating Scale, the Occupational Performance Interview History Interview-II, and the Occupational Self Assessment (Turpin & Iwama, 2011). Holistic evaluation offered by these assessments can support clinicians’ understanding of the impact of volition, habituation, performance capacity, and the environment on the client’s occupational participation (Forsyth & Kielhofner, 2013).
This study aimed to conduct a cross-cultural adaptation of the Occupational Self Assessment (OSA) Version 2.2 into Brazilian Portuguese to support the ongoing efforts to develop theoretically grounded and psychometrically sound assessment measures that can be used by Brazilian practitioners and researchers (Chaves et al., 2010; Cruz, 2018; Cruz et al., 2019; Paulisso et al., 2020). From a methodological perspective, this study is grounded on Classical Test Theory (CTT) to examine the validity of the scores of OSA-Brazilian Portuguese and its reliability (Allen & Yen, 2002).
The OSA Version 2.2 was selected based on the evidence of its feasibility (assessment length and constructs measured), psychometric properties, and clinical utility in occupational therapy (Kielhofner et al., 2009, 2010).
The OSA Version 2.2. complements previously translated assessments and offers insight into the client’s self-reported occupational competency and value, which are not otherwise captured by other assessments. The OSA Version 2.2 is a self-report measure of clients’ perceived occupational competence and value designed to support client-centered practice, evaluation, and outcome tracking (Baron et al., 2006). The OSA has two questionnaires: OSA “My Self” and OSA “My Environment,” administered according to a three-step administration process. In Step 1, the client rates their occupational competence (from “a lot of problems” to “extremely well”). In Step 2, the client assesses the degree of importance of each occupation (from “not so important” to “most important”). In Step 3, the clients analyze their responses and select occupational performance and participation areas to be addressed in the occupational therapy plan.
The OSA Version 2.2 offers practitioners and researchers a valid and reliable measure of the client’s perceived influences of motivation, habituation, communication and interaction skills, process skills, motor skills, and environmental impact on occupational participation (Kielhofner et al., 2010). In addition, a methodological series of three studies using Rasch analysis concluded that OSA could be used by clients with several disabilities and in different practice settings to inform occupational competence and values affecting occupational performance and participation (Kielhofner et al., 2009).
The OSA Version 2.2 has been widely used by clinicians worldwide and translated into 16 languages, but not Brazilian Portuguese. Furthermore, to the authors knowledge, there is no published research examining the clinical utility of the OSA from a South American perspective. The present study aimed to describe the cross-cultural adaptation of the OSA Version 2.2 into Brazilian Portuguese (OSA-Brazil). In addition, the study examined the psychometric properties of the assessment based on face validity, internal consistency, test–retest reliability, and convergent validity with a Brazilian sample of patients with neurological conditions.
Methods
The cross-cultural adaptation of OSA version 2.2 into Brazilian Portuguese and the psychometric properties followed three distinct phases:
Phase I: Translation and cross-cultural adaptation
Phase II: Testing of face validity and utility
Phase III: Evaluation of reliability and validity
These three Phases are detailed below. Prior to initiating the OSA’s translation, the first author contacted the MOHO Clearinghouse at University of Illinois at Chicago to obtain permission to conduct the cross-cultural adaptation of OSA Version 2.2 and evaluate its psychometric properties. After signing a contract, permission was granted to start the translation.
Specifically, the researchers aimed to translate and evaluate the psychometric properties of the “My Self” questionnaire of OSA Version 2.2. This decision was based on previous findings that the “My Environment” scale of OSA had a significant number of items that demonstrated inadequate psychometric properties (Kielhofner et al., 2009).
Phase I: Translation and Cross-Cultural Adaptation
The cross-cultural adaptation was guided by two international guidelines for cross-cultural adaptation studies: (a) guidelines for the process of cross-cultural adaptation of self-report published by Beaton et al. (2000) and (b) guidelines published by the ISPOR Task Force for Translation and Cultural Adaptation (Wild et al., 2005). The process for cross-cultural adaptation proposed by Beaton et al. (2000) was selected as the primary guideline for this study, as it has been recognized as one of the most frequently cited procedures for cross-cultural adaptation in Brazil and international studies (Beaton et al., 2000; Ossada et al., 2020; Paulisso et al., 2020).
The OSA Version 2.2 assessment and administration procedures were initially translated by two independent translators fluent in English and Brazilian Portuguese. Consistent with recommendations by Beaton et al. (2000), one of the translators did not have any prior knowledge of the subject (in this case, specific to MOHO) or the research objectives to avoid theoretical bias. The other translation was performed by an occupational therapist knowledgeable in MOHO concepts. Synthesis of the two independent translations was made by the first and fifth authors, who met to reconcile any differences and propose the final translation. The final translated version of OSA-Brazil was back-translated into English by two independent translators. The first and fourth authors reconciled the back translation. To evaluate whether the back-translated version of the OSA-Brazil was compatible (i.e., had the same item meaning) to the original version of the assessment, the back-translated OSA-Brazil were checked by an American occupational therapist with theoretical and clinical knowledge of MOHO and the OSA Version 2.2 assessment.
The final copy of the OSA Brazil underwent an expert committee review comprised of 10 participants from different professional backgrounds (occupational therapy, physiotherapy, and English language education). Each committee member was asked whether OSA-Brazil was comparable to the original OSA Version 2.2. The committee members rated their agreement based on semantic, cultural, conceptual, and idiomatic compatibility and provided written justification for their decision.
The semantic equivalence determines the equivalence of words in terms of meaning and grammar. As such, this process determines whether the translated terms have the same meaning as initially intended. The idiomatic equivalence analysis sought to determine that any idiomatic expressions in the original assessment were translated to maintain the same meaning as the original assessment. The cultural equivalence determines that the expressions used in the original assessment were consistent with the cultural context of the translated assessment. Finally, the conceptual equivalence determines whether the original assessment’s concepts are maintained in the translated assessment. Specifically, conceptual equivalence refers to the validity of the concept explored, and the events experienced by people of the target culture. This consideration is essential since the items can be equivalent in semantic but not conceptual meaning (Guillemin et al., 1993).
The data gathered during the expert committee review was analyzed using the Agreement Index (AI) (Cohen, 1960).

The authors and the expert committee reviewed any item with an AI < 80% and revised until AI > 80% was achieved. Then, the items were analyzed according to the AI in semantic equivalence, idiomatic equivalence, cultural equivalence, and conceptual equivalence.
Phase II: Face Validity and Utility
Pilot testing was conducted with a convenience sample of 24 participants (12 undergraduate students in occupational therapy and 12 patients receiving occupational therapy services). The inclusion criteria for occupational therapy students were as follows: >18 years old and completing their final year of occupational therapy undergraduate studies (Wild et al., 2005). The inclusion criteria for participants with neurological conditions under occupational therapy services were as follows: >18 years old, score ≥18 on the Mini-Mental State Examination (MMSE) and have a neurological diagnosis. Given that the OSA is a self-report measure, the MMSE was used to ensure that the participants had adequate cognitive skills to understand and respond to the assessment. In addition, to accommodate differences in literacy levels, the 18-point cut-off score was selected since it was previously shown to be appropriate for clients with limited literacy levels in Brazil (Lourenço & Veras, 2006).
It is recommended that translation research examines assessments from two different strata of potential users: (a) the lowest stratum of the assessment’s potential users who have minimal knowledge of the assessment tool and (b) the highest stratum of potential users who have extensive knowledge of the assessment tool (Ossada et al., 2020; Paulisso et al., 2020). The expert committee represented the highest stratum. The lowest stratum was represented by undergraduate students in occupational therapy and clients with neurological conditions.
In addition to representing a population of clients without cognitive deficits, occupational therapy students were selected based on their future roles as occupational therapists. The students recruited were in their final year of occupational therapy education and enrolled in a clinical practice placement in neurological rehabilitation. Professionals in the field must understand the assessment and its aims (Wild et al., 2005). Therefore, it was hypothesized that if students in occupational therapy can understand the translated OSA items, the assessment would also be accessible to occupational therapy practitioners.
Participants with neurological conditions were recruited to represent a crucial population in Brazilian occupational therapy services. In Brazil, neurological conditions (e.g., stroke) are recognized as the leading cause of hospitalization and disability (Dantas et al., 2019). We also wanted to investigate the accessibility of the translated assessment for individuals with a range of neurologically based difficulties (i.e., motor, processual, and interaction and communicational skills). Finally, it was hypothesized that this sample would ensure that the data was a representation of the client’s characteristics commonly seen in the Brazilian context of practice.
At the start of the study, both participant groups were presented with the OSA assessment form, and prior assessment instructions were provided before completing the form. Participants with fine motor impairments had the first author’s assistance completing their assessment form. Following assessment completion, the participants were directed to complete an additional survey developed by the first and fifth authors to evaluate the participants’ perception of (a) their understanding of each item, (b) assessment length, (c) assessment difficulty, and (d) their capacity to complete the assessment without assistance from the researchers. Each item was rated on a four-rating scale (Figure 1). The participants were given an option to add comments for any areas for improvement to ensure that the assessment appropriately targeted clients’ needs within the Brazilian cultural context. Statistical analysis was performed using SPSS software version 22 (Nie et al., 2013).
Phase III: Evaluation of Reliability and Validity
The reliability and validity of the OSA-Brazil were examined with a convenience sample of occupational therapy clients receiving rehabilitation services in Brazil. The participants were recruited from an outpatient rehabilitation clinic that was associated with a public university. Participants were eligible to participate in the study if they were receiving occupational therapy or physiotherapy services. Additional inclusion criteria were: >18 years old, score ≥ 18 on the MMSE and have a neurological diagnosis. To accommodate differences in literacy levels, the 18-point cut-off score was selected since it was previously shown to be appropriate for clients with limited literacy levels in Brazil (Lourenço & Veras, 2006). The procedures for the assessment administration were the same as the ones in Phase II.
The reliability of the OSA-Brazil was examined according to test–retest reliability and internal consistency. Test–retest reliability was used to evaluate how the same results could be achieved across two administrations on two separate time points, 10–14 days between the first and second administration. The intraclass correlation coefficient (ICC) of > 0.70 was considered the minimum acceptable, once different publications ranging from alpha values between 0.70 and 0.95, where high values are >90 (Tavakol & Dennick, 2011). Cronbach’s alpha coefficients were used for examining internal consistency, with a coefficient > 0.70 classified as acceptable (Tavakol & Dennick, 2011).
The validity of the OSA-Brazil was examined to gauge whether the translated assessment was measuring the construct initially intended. Construct validity examines the extent to which a measure corresponds to its theoretical constructs of the phenomenon to be measured (Cozby, 2009). Construct validity was examined by evaluating the OSA-Brazil’s convergent validity with the 36-Item Short-Form Health Survey (SF-36). The SF-36 is a gold standard measure of health-related quality of life. The measure evaluates the quality of life across eight domains: vitality, physical functioning, bodily pain, general health perceptions, physical role functioning, emotional role functioning, social role functioning, and mental health (Ciconelli et al., 1999). Based on previous research findings from a study that performed a cross-cultural adaptation of the OSA Version 2.2 for Malaysia, it was hypothesized that participants’ self-reported occupational performance would be positively correlated with their self-reported health-related quality of life (Murad et al., 2011). It was also hypothesized that there would be a strong correlation between the OSA-Brazil and SF-36. According to Forsyth and Kielhofner (2013), correlational research can support the investigation of relationships between constructs proposed in MOHO theory. We hypothesized that carrying out this analysis would address the need to examine the construct validity of the OSA-SF while also providing insight into how the OSA-SF can be used with other assessments in Brazil.
Spearman’s rho correlation coefficient was used to test the OSA-Brazil construct validity with the SF-36. The strength of correlation was evaluated according to criteria proposed by Munro (2011): p < .05: ≥ 0.75 = strong; 0.50–0.74 = moderate; and ≤0.49 = weak. Statistical analysis was performed using SPSS software version 22 (Nie et al., 2013).
Ethical Considerations
The Ethics Application was submitted and approved by the Institutional Review Board at the University where the research was conducted. The study commenced only after ethical approval, including the pilot testing. All participants, including expert committee members, occupational therapy students, and patients, were informed of the study’s risks and benefits. Their participation was voluntary, and their identity was anonymized. To avoid harm, participants with neurological conditions who responded to the questionnaires were offered the option to complete the questionnaires in two meetings. The researcher also proposed breaks to prevent fatigue in case of discomfort and stress. We statement that all participants have provided written informed consent.
Results
Phase I: Translation and Cross-Cultural Adaptation
The characteristics of the expert committee are presented in Table 1. The majority of committee members had 5–10 years of professional experience and worked in physical rehabilitation.
Expert Committee Background.
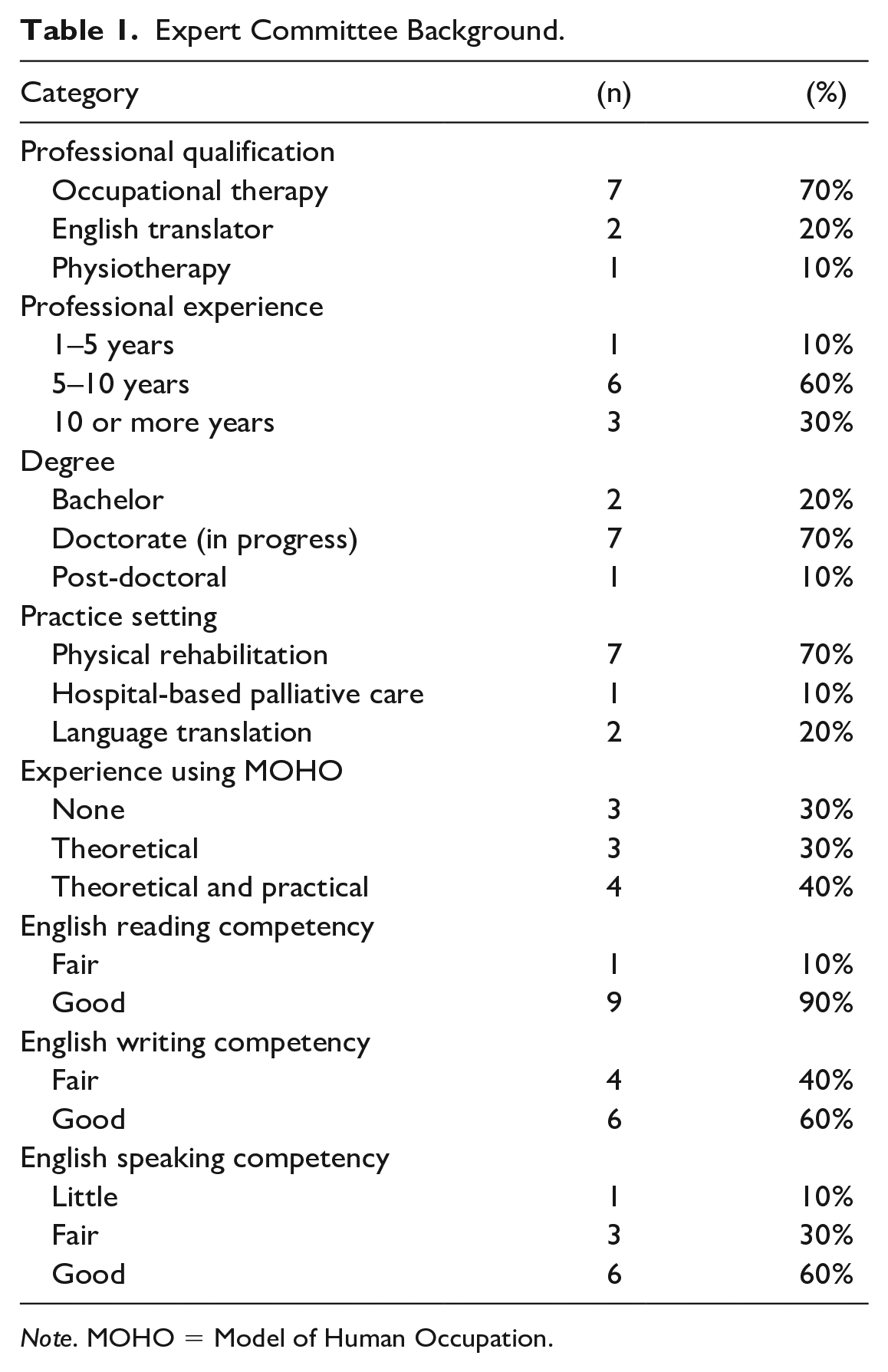
Note. MOHO = Model of Human Occupation.
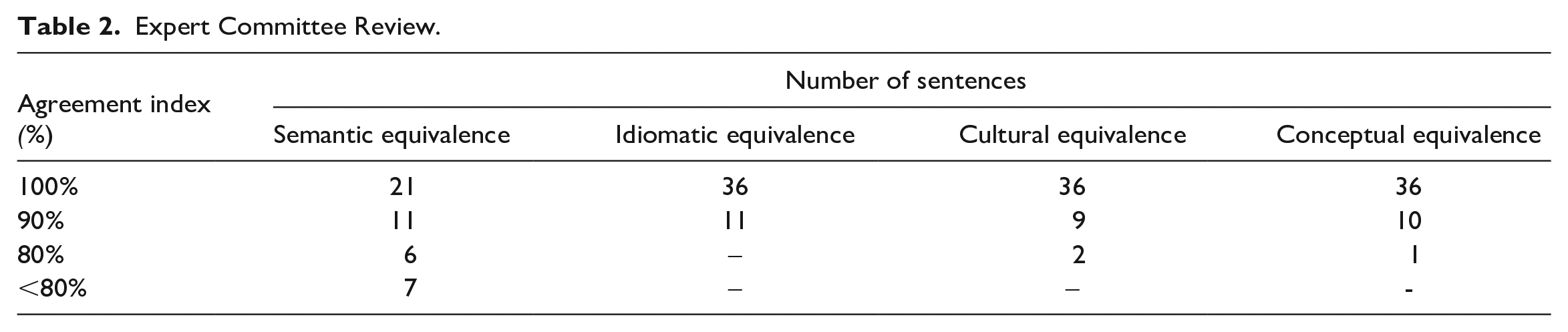
Table 2 summarizes the AI obtained from the expert committee. Seven items on the OSA questionnaire did not meet the 80% cutoff for AI regarding semantic equivalence. The revision of the items indicated the need to re-structure the sentences to correspond to the Brazilian Portuguese language in the order of words. For example, the original item: “I have some difficulty doing this,” was initially translated as “Tenho alguma dificuldade em fazer isto” (Have some difficulty doing this). After review by the expert committee was decided to add the pronoun to increase the level of comprehension of this item for “Eu tenho alguma dificuldade ao fazer isto.”
Expert Committee Review.
Phase II: Pilot Testing and Evaluation of Face Validity
The pilot testing was conducted with a total of 24 participants divided into two groups: (1) undergraduate students in the final year of an occupational therapy course and (2) people with neurological conditions.
Twelve people with a neurological condition were enrolled in the pilot testing of the OSA-Brazil. The average participant age was 53 ± 12 years. The majority of participants were women (n = 7) and reported that they were retired (n = 10). Four participants reported previous experience with physical and occupational therapy. Participant diagnoses included stroke (n = 10), multiple sclerosis (n = 1), and spinal cord injury (n = 1). The average total score on the MMSE was 24 ± 4, with only two participants receiving a maximum possible score of 30. Participants with neurological conditions had an average score of 46 ± 12 on the competence subscale and 63 ± 10 on the value subscale on the OSA questionnaire. The most commonly identified goal items included: “Physically doing what I need to do” (n = 8), “Getting where I need to go” (n=4), “Doing activities I like” (n=4), and “Concentrating on my tasks” (n = 3).
Twelve students were enrolled in the pilot testing of the OSA-Brazil. The average participant age was 22 ± 1 years. The majority of participants were women (n = 11). Only one participant reported a medical diagnosis of Carpal Tunnel Syndrome. All participants obtained a maximum score of 30 on the MMSE. Participants had an average score of 55 ± 5 on the competence subscale and 57 ± 8 on the value subscale on the OSA questionnaire. The most commonly identified goal items included “Getting done what I need to do ” (n = 6), “Concentrating on my tasks” (n = 5), “Taking care of myself” (n = 5), and “ Having a satisfying routine ” (n = 5).
For the group of participants with neurological conditions, the assessment was reported as having an appropriate length (n = 11). Five participants reported that the content was easy to understand. While the majority reported that they could respond to the assessment without assistance from a therapist (n = 8), five participants reported having doubts while completing the assessment, and six reported difficulties differentiating between the competence and value categories.
Student participants’ results suggested that the assessment was an appropriate length (n = 10), and the content was easy to understand (n = 9). However, the majority also reported having doubts while completing the assessment (n = 9) and reported difficulty differentiating between the competence and value categories (n = 6). Only four participants reported feeling competent enough to complete the assessment without support from a therapist.
In addition, 100% of respondents in both groups reported difficulties understanding the difference between the two rating scales, “mais importante” (really important), and “o mais importante” (most important). Based on this finding, it was recommended to replace “o mais importante” (most important) with “importantissimo.” Finally, 50% (n = 6) of the participants in both groups reported difficulties differentiating between Step 1 (rating of occupational competence) and Step 2 (rating of importance of each occupation). To assist with readability, changes were made in the assessment’s layout to present its content so that the respondents could easily locate the items corresponding to the two steps. One column between the two steps was added to visually guide the respondent without modifying the assessment layout when compared with the original version.
Phase III: Analysis of Reliability and Validity
Fourty participants with neurological diagnoses (not including the 12 from Phase II) were enrolled in the final testing of the OSA-Brazil. The average participant age was 51.8 ± 15 years. The majority of participants were women (n = 27). Participant diagnoses included: stroke (n = 26), traumatic brain injury (n = 4), spinal cord injury (n = 2), cerebral palsy (n = 2), hemiparesis without clear diagnosis (n = 2), Guillain-Barré Syndrome (n = 2), and neurotoxoplasmosis (n = 2). The average total score on the MMSE was 26 ± 3. All participants were currently enrolled in occupational therapy and physiotherapy services.
Table 3 presents that the OSA-Brazil presented good internal consistency and test–retest reliabilities and a high level of Cronbach’s alpha coefficients:
ICC and Cronbach’s Alpha Coefficients for OSA-Brazil.
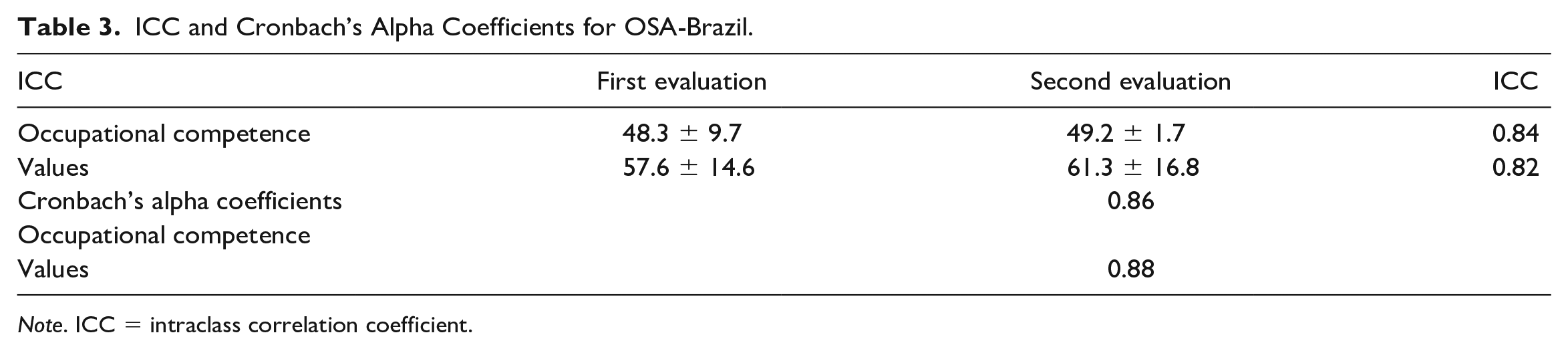
Note. ICC = intraclass correlation coefficient.
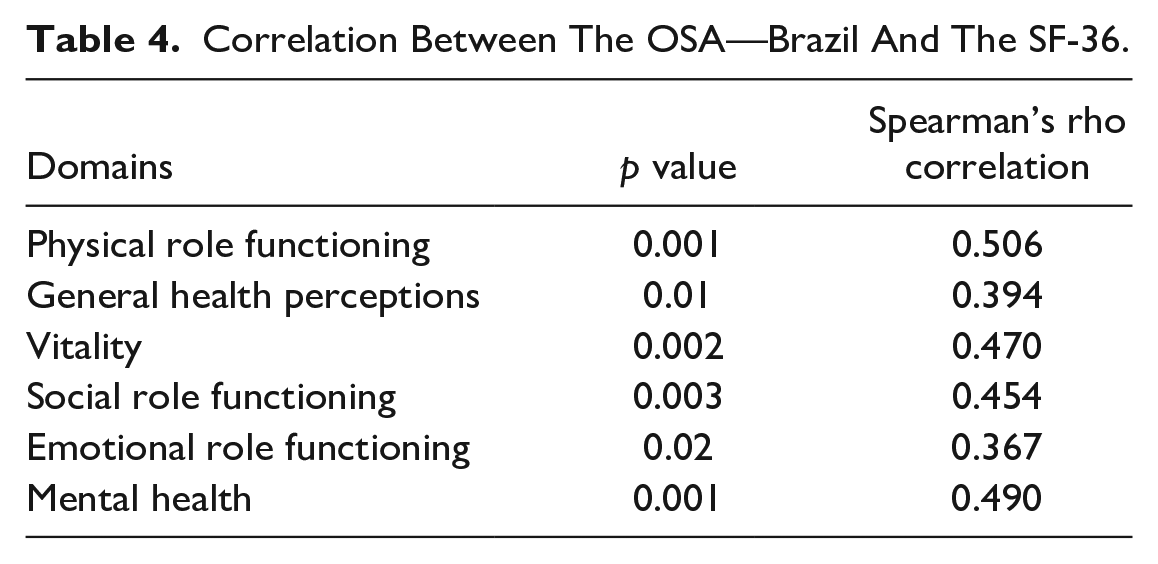
Table 4 shows a significant correlation between the OSA-Brazil questionnaire’s competence section and six domains on the SF-36.
Correlation Between The OSA—Brazil And The SF-36.
Discussion
This original research offers initial evidence to support the reliability and validity of OSA-Brazil. The cross-cultural adaptation process followed the procedures guided by two guidelines, and multiple steps were taken to ensure that the assessment was both psychometrically sound and clinically relevant for practitioners and clients (Beaton et al., 2000; Wild et al., 2005).
The OSA was selected for this study based on (a) being grounded in a well-established occupation-focused theory and (b) having occupational performance as the central feature of this assessment. The MOHO conceptualizes occupational participation as influenced by the dynamic components: volition, habituation, performance capacity, and the environment. This model has been recognized as one of the few to explicitly address volition in detail as a critical contributor to occupational performance (Taylor & Kielhofner, 2017). As a result, the OSA-Brazil can gather relevant information about the client’s perception of their occupations, offering a novel way of assessing their needs, reinforcing occupation-focused practice and client-centered practice, as premises described by the World Federation of Occupational Therapists (WFOT, 2010).
Existing assessment measures available in Brazilian Portuguese continue to be limited in their scope to assess occupational performance and do not consistently recognize intrinsic and extrinsic influences on occupational performance (Chaves et al., 2010). The MOHO is comprehensive and recognizes intrinsic (i.e., personal factors) and extrinsic (i.e., environment factors) contributors to occupational performance (Cruz, 2018). As a self-report measure of occupational performance, the OSA-Brazil offers Brazilian occupational therapists an opportunity to better understand the client’s experience while considering their perceived competence and values. Furthermore, by capturing both intrinsic and extrinsic factors, the OSA-Brazil can guide client-centered clinical reasoning and goal setting.
Translation and Cross-Cultural Adaptation
Two commonly identified barriers to cross-cultural adaptation of assessments include (a) the translation of words which has no equivalent translation between the languages and (b) the evaluation of an item that is not common to the target culture (Epstein et al., 2015). However, neither of these challenges were identified in this study’s translation, back translation, or expert committee review stages. These findings can be explained by the fact that the OSA was initially developed and tested in partnership with therapists from different countries, which likely helped minimize the above-mentioned cultural interference (Baron et al., 2006). Our findings are further supported by the fact that MOHO and its assessments have been studied in several countries, and its theories consider the client’s narratives and concepts, such as occupational forms, that “are culturally defined for each client” (Forsyth & Kielhofner, 2013, p. 66).
Pilot Testing and Evaluation of Face Validity
In addition to rigorous translation and back-translation processes, pilot testing was essential for final modifications in the content and the layout of the final OSA-Brazil. The assessment was well received by participants in both pilot groups (individuals with neurological diagnoses and undergraduate occupational therapy students), and both participant groups were able to use the OSA-Brazil to identify areas for change. The primary item identified as a goal area by individuals with neurological diagnoses was: “Physically do what I need to do.” This finding suggests that physical impairments may directly impact people’s performance capacity with neurological conditions, suggesting that OSA-Brazil can capture how individuals perceive their occupational performance considering a neurological condition. The primary item identified as a goal area by occupational therapy students was: “Getting done what I need to do.” This result suggests that the assessment is also sensitive to people’s occupational demands without specific diagnoses or health conditions and may be responsive to any acute stressors that compromise the individual’s capacity to perform their occupations. In this case, the findings may be the occupational stressors associated with the student role and the occupational demands and expectations to complete academic activities to fulfill this role (Asgari & Kramer, 2008).
It must also be noted that participants in both pilot groups reported that they would respond to the full assessment without therapist cues or support. A small percentage of participants reported that some items were confusing. Based on these findings, it must be recognized that ongoing assessment development could facilitate client independence in completing this self-report measure. However, these results are not seen as a barrier to OSA-Brazil’s clinical utility in research or clinical practice. Support and supervision from an occupational therapy practitioner have been recognized as essential features of the assessment administration process (Baron et al., 2006).
Phase III: Analysis of Reliability and Validity
Our results offer the initial evidence supporting internal consistency and test–retest reliability of the OSA-Brazil with a neurological population of clients. Furthermore, the OSA-Brazil construct validity was supported by evidence of convergent validity with six domains on the SF-36 (Ware, 2000). This finding is consistent with previous research, which found significant correlations between the OSA-Brazil and the SF-36 (Murad et al., 2011). The OSA was developed to assess occupational competence and values’ self-perception across 21 items on the OSA questionnaire.
Domains of physical health measured by the SF-36 were directly related to occupational competence measured by OSA-Brazil. This domain assesses skills necessary to perform vigorous (e.g., lifting heavy objects, running, or climbing stairs) or moderate (e.g., carrying groceries, showering, or getting dressed) activities, which are consistent with items specific to physical and motor skills on the OSA-Brazil (e.g., physically doing what I need to do, or getting where I need to go). Furthermore, while this assessment was not intended to assess mental or emotional health, significant correlations were found with the SF-36 “Emotional Role Functioning” and “Mental Health” domains. This finding suggests a relationship between the occupational competence of people with neurological conditions and their psychological well-being.
According to MOHO, performance capacity refers to the “ability to do things provided by the status of underlying objective physical and mental components and corresponding subjective experience” (Tham et al., 2017, p. 75). Performance capacity depends on the muscular, neurological, cardiopulmonary, and other body systems used when acting in the world. Even indirectly, other OSA-Brazil items were also related to the physical aspects of the person. The habituation items (e.g., “Getting done what I need to do” and “Having a satisfying routine”) or the volition items (e.g., “Accomplishing what I set out to do” and “Effectively using my abilities”) may be influenced due to a person’s physical limitations, which justifies the correlation with the SF-36 domains. The correlation between OSA-Brazil and SF-36 supports our understanding that the physical and mental domains of the SF-36 are likely related to the client’s self-reported occupational competence and may contribute to how individuals experience their occupational performance (Kielhofner, 2008). Moreover, a critical discussion is that the complexity of human occupation requires understanding the dynamic interaction of MOHO components rather than its components separately.
Conclusions
This study offers evidence in support of satisfactory cross-cultural adaptation of the OSA Version 2.2, the OSA-Brazil. Based on an expert review, the OSA-Brazil was found to have appropriate semantic, idiomatic, cultural, and conceptual equivalence. Pilot testing on the OSA-Brazil offered evidence for the assessment’s face validity and clinical utility. Internal consistency, test–retest reliability, and convergent validity of the OSA-Brazil with the SF-36 were then supported through testing with a larger sample of individuals with neurological conditions.
This study’s primary limitation is that, to the authors’ knowledge, there are no assessments available in Brazil to measure the same constructs as the OSA (occupational competence and values). This significantly limited the type of methodological approaches used and, subsequently, the findings of this study. Another limitation is specific to the study sample. Individuals with neurological conditions may have been limited in their capacity to accurately appraise the accessibility of the translated assessment. However, we felt that this sample was crucial for ensuring a representative sample of occupational therapy clients in Brazil.
We believe that OSA-Brazil will support evidence-based and theoretically grounded assessment practices and ensure psychometrically sound and client-centered approaches. Future research with large samples should evaluate how the OSA-Brazil items are correlated with other variables such as role identity, occupational participation, performance, and skills are needed. Studies of Rash analysis are recommended to verify if the Brazilian version can measure changes over time.
Supplemental Material
sj-jpg-1-otj-10.1177_15394492231188614 – Supplemental material for Cross-Cultural Adaptation, Reliability, and Convergent Validity of Occupational Self-Assessment for Brazilian Portuguese
Supplemental material, sj-jpg-1-otj-10.1177_15394492231188614 for Cross-Cultural Adaptation, Reliability, and Convergent Validity of Occupational Self-Assessment for Brazilian Portuguese by Paulo V. B. Mendes, Debora C. M. Carrijo, Jacqueline D. Costa, Evguenia S. Popova, Kathi B. Baron and Daniel M. C. Cruz in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
The authors would like to thank the Coordination for the Improvement of Higher Education Personnel (CAPES) (Brazil) for the research grant, as well as all the research participants.
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Fundação Coordenação Aperfeiçoamento de Pessoal de Nível Superior (CAPES) on project: Rede de Cooperação Universitária para o Ensino, Pesquisa, Desenvolvimento e Inovação em Tecnologia Assistiva, through a doctoral scholarship (grant no. 88882.160590/2017-01).
Research Ethics and Patient Consent
The permission to conduct the cross-cultural adaptation of OSA V2.2 was obtained from University of Illinois at Chicago. The research was submitted and approved by the Research Ethics Committee of the Federal University of São Carlos, São Carlos, Brazil, respecting the prerogatives of Resolution 466/12 of the National Commission of Ethics in Research (CONEP), which deals with ethics in human research, under the advice of number 2.636.017.
Were appropriate informed consent procedures were used and all subjects were informed of the study’s risks and benefits, that their participation was voluntary, and that their identity would not be disclosed. Appropriate handling of confidentiality and data security were confirm for authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.