
Abstract
Post-stroke neglect is disabling, yet it is unclear whether existing assessments capture the extent neglect affects activity and participation. The objective of the study is to explore stroke survivor and caregiver perspectives on how neglect affects activity and participation and to compare their experiences to neglect assessments items. We conducted an explanatory sequential mixed-methods study by conducting semi-structured interviews with stroke survivors (n = 7) and caregivers (n = 7) analyzed using thematic analysis. Stroke survivors completed the Catherine Bergego Scale (CBS) and Behavioral Inattention Test (BIT). Descriptive analyses characterized participant’s neglect. The standardized CBS and BIT tests indicated that stroke survivors demonstrated mild-to-moderate (CBS) or no-to-mild (BIT) neglect. In contrast, the qualitative data revealed serious safety concerns and significant ongoing difficulties participating in school, work, and family activities because of neglect. Current assessments may not measure the impact of neglect on activity or participation in life for stroke survivors.
Plain Language Summary
Individuals with neglect after stroke experience disability. This study interviewed individuals with neglect and their caregivers to understand whether clinical assessments capture the impact that neglect has on their daily life. Results show that existing assessments may not fully measure the challenges that individuals experience.
Unilateral neglect (neglect) is a common neurological disorder that is defined as a failure to perceive, orient, or attend to stimuli on the side opposite the lesion (Heilman et al., 1987). Neglect can manifest in a number of ways. Individuals may experience egocentric neglect (viewer-centered) where they neglect one side of near space (peripersonal neglect), one side of far space (extrapersonal neglect), or one side of their own body (personal neglect). Individuals can also have allocentric neglect and neglect one side of objects (Esposito et al., 2021). Neglect is prevalent following stroke and affects approximately 30% of stroke survivors (Esposito et al., 2021). Although it is more common to have left-sided neglect as a result of a right hemisphere lesion, individuals with left hemisphere lesions also experience right-sided neglect (Appelros et al., 2004). While natural recovery can occur and some individuals see a resolution of symptoms, neglect persists for approximately one third to one half of individuals into the chronic stage of stroke recovery (i.e., ≥6 months post–stroke; Appelros et al., 2004). Neglect has a negative impact on a stroke survivor’s ability to perform activities of daily living (ADLs). Individuals with neglect have greater disability, require longer hospitalizations, and have poorer life satisfaction compared with stroke survivors without neglect (Chen et al., 2015; Nijboer et al., 2013; Vossel et al., 2013). A recent systematic review and meta-analysis by Revet et al. (2021) also found that individuals with neglect have worse functional outcomes (standardized mean difference of −0.93 [95% confidence interval (CI) = [−1.27, −0.59]) at follow-up compared with those without neglect. Individuals with neglect also frequently have anosognosia (i.e., lack of awareness) that further contributes to disability (Vossel et al., 2013).
Given the prevalence of neglect and the negative outcomes associated with neglect, it is imperative that stroke survivors are adequately assessed for neglect and that clinicians determine how neglect affects a patient’s ability to perform activities and participate in life roles. Clinicians require this information for treatment planning and accurate measurement of a patient’s progress. However, existing neglect assessments are largely impairment-based and examine performance on simple paper–pencil-based tasks and in a quiet clinical setting with few distractions rather than the complex environment of the home and community (Grattan & Woodbury, 2017). Although commonly used, these paper–pencil assessments do not provide clinicians with information regarding how neglect affects daily life.
In contrast to paper–pencil impairment-based assessments, behavioral neglect assessments (i.e., functional-based) largely examine neglect in the context of ADLs and these have consistently demonstrated higher sensitivity in detecting neglect (Azouvi et al., 2006; Grattan & Woodbury, 2017). The Catherine Bergego Scale (CBS) is one of the most frequently used behavioral neglect assessments (Azouvi et al., 2006). An assessor observes an individual complete 10 different task items such as eating, dressing, and navigation to determine whether the individual has neglect and, if so, determine its severity. The Behavioral Inattention Test (BIT) is another commonly used neglect assessment and includes both conventional items (i.e., paper–pencil items) and behavioral items (Wilson et al., 1987). The behavioral items include tasks such as copying an address, reading a clock, and sorting coins.
While behavioral neglect assessments such as the CBS and BIT have some items that address instrumental activities of daily living (IADL) domains, items tend to focus more on ADLs or encompass a small aspect of an IADL (e.g., sorting coins as part of money management); hence, they may not capture the extent to which neglect affects performance of IADLs or participation in real-world settings. For example, an individual with neglect may be able to get dressed and eat independently. However, they may not be able to go grocery shopping, care for their child, or return to work because of their neglect. Current neglect assessments may fail to detect the full extent of the impact of neglect on individuals’ lives because they may not include items assessing these types of tasks. In fact, a study conducted by Klinke et al. (2016) examined the experiences of patients with neglect after discharge from inpatient rehabilitation to home (i.e., subacute stage-weeks to months post-stroke) and found that many of the challenges stroke survivors with neglect (SS) faced were not captured by the neglect assessments that were administered.
Commonly used behavioral neglect assessments focus on ADLs, but lack a breadth of items related to IADLs, home, and community activities. Hence, it remains unknown whether these assessments are comprehensively measuring and characterizing the true impact of chronic (>6 months post-stroke) neglect on an individual’s life. We sought to understand the degree to which neglect affects the daily life of stroke survivors and caregivers and to determine whether assessment items correspond. The purpose of this study was to (a) understand from both stroke survivor and caregiver perspective how neglect affects activity (“the execution of a task or action by an individual”) and participation (“involvement in life situation”) as defined by the International Classification of Functioning, Disability and Health (ICF; World Health Organization [WHO], 2001, p. 10); (b) compare these findings with the items on commonly used behavioral neglect assessments; and (c) compare the degree of impairment (based on performance on behavioral neglect assessments) with themes that the stroke survivor and/or caregiver report with regard to disability and participation restrictions.
Method
Design
We used an explanatory sequential mixed methods study design (Creswell & Plano-Clark, 2017). Explanatory sequential mixed methods begin with quantitative data collection and analysis and then incorporate qualitative data collection approaches to better understand quantitative findings (Creswell & Plano-Clark, 2017). Integrating findings from multiple datasets using a mixed methods design allows for enhanced understanding of complex questions within real-world environments (Bazeley, 2018). Within an explanatory sequential mixed methods design, qualitative and quantitative data are analyzed independently and then integrated for expanded interpretation, allowing for a more robust understanding of the concept studied. This study was conducted at an academic medical center and was approved by the local institutional review board. All work followed the ethical standards of the revised Declaration of Helsinki.
Participants
Purposive sampling was used to recruit participants. SS were recruited from a cross-sectional stroke neglect rehabilitation study. Participants were eligible if they met the following criteria: (a) unilateral hemispheric stroke >6 months ago, (b) had neglect based on score <18 on the Virtual Reality Lateralized Attention Test (VRLAT) that was administered by a licensed occupational therapist, (c) ≥18 years of age, and (d) English language speaking. Participants were excluded if they had severe aphasia limiting their ability to participate in an interview. Caregivers of stroke survivors with neglect (CG) were recruited and were eligible if they met the following criteria: (a) were ≥18, (b) spoke English language, and (c) identified as the CG of the participating SS.
Instruments
We collected demographic data (e.g., age, gender, race) from all participants and stroke information (e.g., stroke lesion side and type, time since stroke) from the SS. We collected demographic and caregiving data (e.g., relationship of the CG to the SS) from CG. SS were administered a stroke severity assessment (National Institutes of Health Stroke Scale [NIHSS]), neglect assessments (BIT, CBS), and then participated in the interviews. CGs were then scheduled to participate in their interviews separately (Azouvi et al., 2006; Goldstein & Samsa, 1997; Wilson et al., 1987).
Quantitative
Stroke Severity
The NIHSS is an assessment commonly used to assess stroke symptoms and characterize stroke severity (Goldstein & Samsa, 1997). The NIHSS includes 15 items, and each item has specific scoring criteria. Item ratings are summed to derive a total score that can range from 0 to 42. Higher scores indicate greater stroke symptoms and severity (Goldstein & Samsa, 1997).
Neglect
The VRLAT was administered to screen for eligibility and determine whether participants had neglect (score <18/20; Buxbaum et al., 2012). The VRLAT is a valid and reliable measure of neglect and has greater sensitivity at detecting neglect when compared with paper–pencil assessments (Buxbaum et al., 2012).
We administered the CBS as part of the assessment battery. The CBS items are scored on a 4-point scale (0 = no neglect to 3 = severe neglect). Items on the CBS are summed to derive a total score that can range from 0 to 30. Item scores and total scores ≥1 indicate neglect. Higher scores indicate greater neglect severity. The psychometric properties of the CBS are well established (Azouvi, 2017).
We also administered all of the behavioral items of the BIT (Wilson et al., 1987). The BIT items have their own scoring criteria but use a 10-point scale (scores range from 0 to 9). Item ratings are summed to derive a total score (0–81) and lower scores indicate greater neglect. A total score less than 67 indicates the presence of neglect. Individual items do not have cutoff scores established to indicate the presence of neglect. The BIT has well-established psychometric properties (Wilson et al., 1987).
Quantitative data were analyzed using IBM SPSS Statistics for Windows, Version 27 (IBMCorp, 2020). Descriptive analyses were conducted to characterize the sample and participants’ performance on the neglect assessments. We used the CBS and BIT item scores to determine whether SS demonstrated impairment on each of the assessment items. As the BIT does not have specific item cutoff scores, we conservatively used a score of 8, which indicates that the participant demonstrated some degree of impairment performing the item (Wilson et al., 1987). We calculated the number and percentage of SS who demonstrated impairment on each assessment item and the number and percentage of participants (SS and CG) who described challenges completing these types of daily tasks when interviewed.
Qualitative
A semi-structured interview guide was developed by a team of investigators led by an expert qualitative and mixed methodologist to ensure the same guiding questions were used during interviews and to expand understanding of quantitative data collected. It was generated based on the overall study objectives, specific aims, research questions, and content area captured within the instruments. SS questions focused on the impact of neglect on daily life. Following are the sample SS questions: (a) How does neglect affect your life? and (b) what would you like to do that you can’t do because of your neglect? CG questions had a similar focus but included questions regarding the role the CG plays in supporting the SS. Sample questions included the following: (a) How does neglect affect your life or your loved one’s life? and (2) can you describe some challenges due to neglect that he or she might face throughout a typical day if you were not there to help? Investigators asked follow-up questions to facilitate clarification and further explanation. To reduce the influence of potential researcher bias, each participant was asked prior to the conclusion of the interview whether there was anything else they felt was important to share that the study team did not ask about.
We collected interview data between June 2019 and February 2020. The individual, face-to-face, semi-structured interviews lasted approximately 30 to 45 min. We audio-recorded interviews and kept field notes to document observations. Audio-recordings from interviews were transcribed verbatim using a professional transcription service. A priori codes based on the interview guide and study aims were added to a codebook and emergent codes were added as needed. Initial coding was conducted by three investigators (E.G., M.N., E.H.) using a Level 1 approach (manifest) (Saldaña, 2015). Codes were then reviewed and confirmed by the same investigators. Each interview underwent Level 2 (latent) coding by all three investigators. Level 1 or manifest codes are essentially paraphrased, whereas Level 2 or latent codes highlight participant voices or the meaning behind what is said. Consensus on coding was reached during regular face-to-face team meetings. Investigators agreed on operational definitions and terms for emergent codes, and overarching themes and findings were further evaluated based on items within both the CBS and BIT instruments. An audit trail was also maintained throughout the qualitative analytical methods to enhance trustworthiness. Data saturation was reached with the qualitative data collected and analyzed, a key metric for ensuring reliability of findings.
Results
Quantitative
Fourteen participants (seven SS, seven CG) provided informed consent. The seven SS participated in the neglect assessments and all the SS and CG participated in the individual interviews. Demographic and descriptive data can be found in Tables 1 and 2. SS participants were primarily White females who had a mild-to-moderate (based on NIHSS scores) right hemispheric ischemic stroke. CG were primarily White males and were the spouse of the SS.
Participant Characteristics.
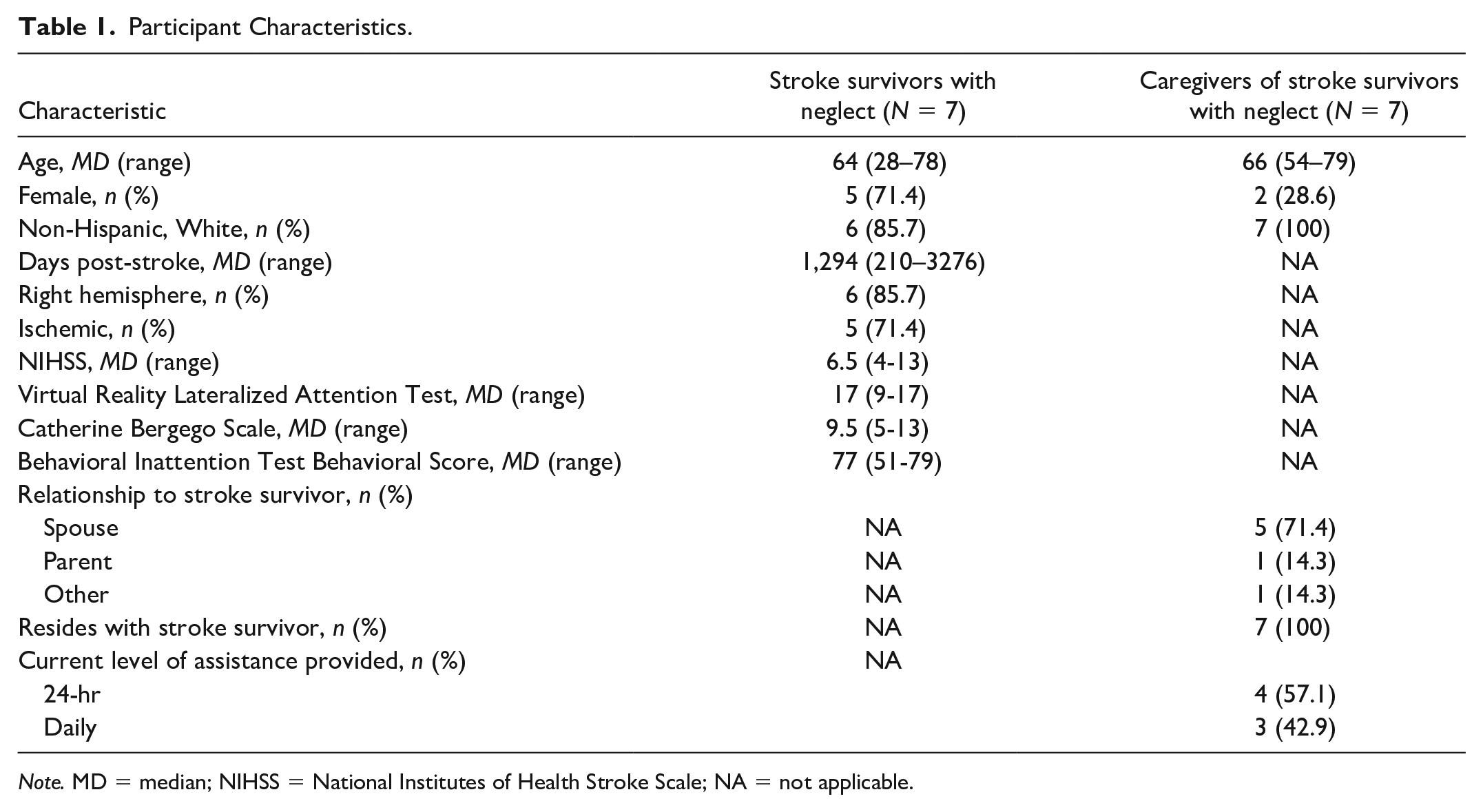
Note. MD = median; NIHSS = National Institutes of Health Stroke Scale; NA = not applicable.
Assessment Item Scores for Stroke Survivors With Neglect (N = 7).
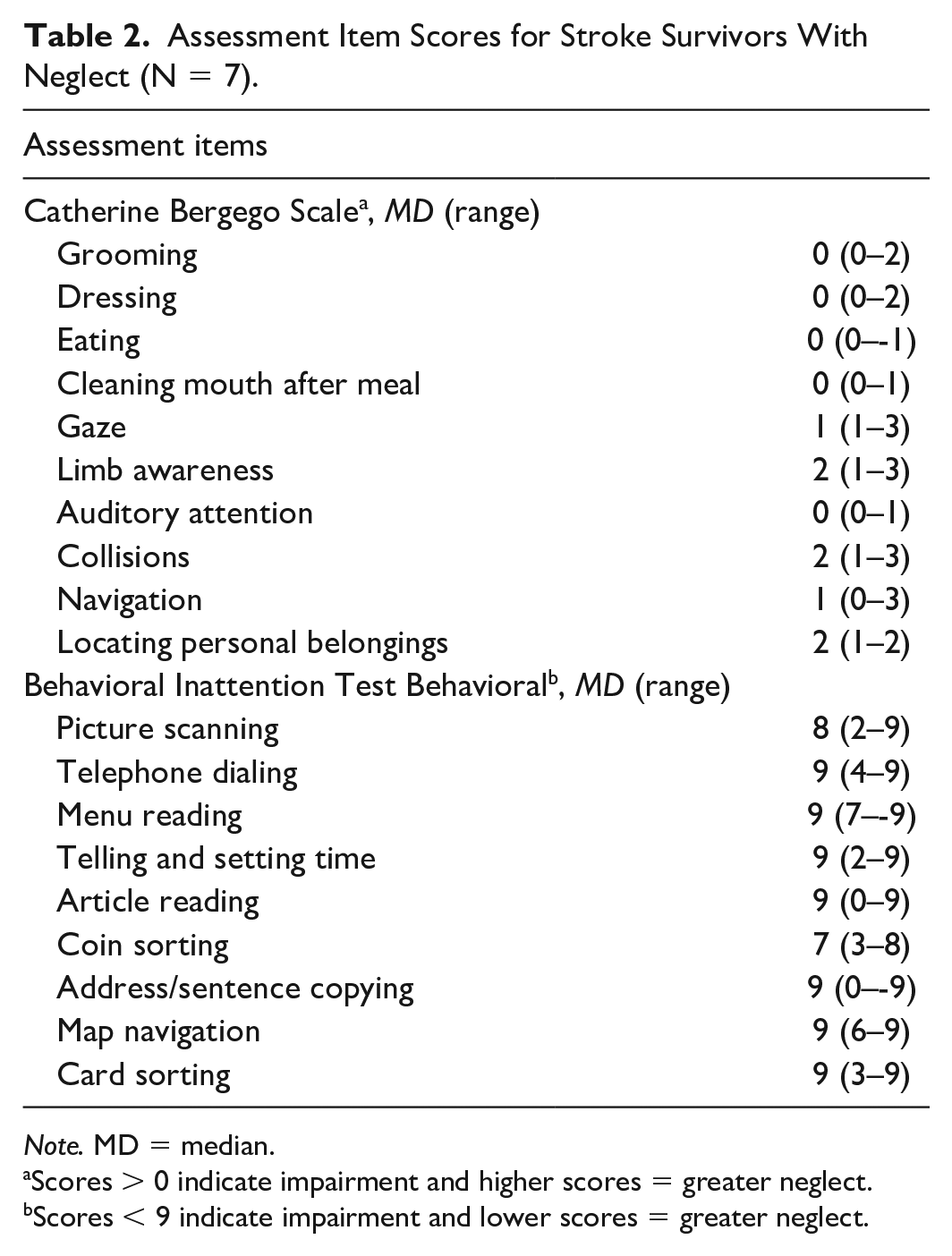
Note. MD = median.
Scores > 0 indicate impairment and higher scores = greater neglect. bScores < 9 indicate impairment and lower scores = greater neglect.
All SS demonstrated some degree of neglect (mild-moderate) based on the CBS total scores (Table 1). At the item level, the median scores for the CBS ranged from 0 to 2 indicating no to mild neglect (Table 2). SS largely did not demonstrate neglect based on the BIT, as total scores primarily exceeded the established cutoff score (Table 1). Most participants did not demonstrate impaired performance on the items on the BIT as the median score for seven of nine items on the BIT was 9, indicating a perfect score on the item (Table 2). Thus, the BIT was not sensitive at detecting neglect in many participants.
Participants’ performance on the various items of the CBS and BIT varied considerably (Table 3). However, all participants demonstrated impairment on the three CBS items (gaze, limb awareness, and personal belongings) and one BIT item (coin sorting).
Comparison of Participant-Reported Disability to Performance on Neglect Assessments.
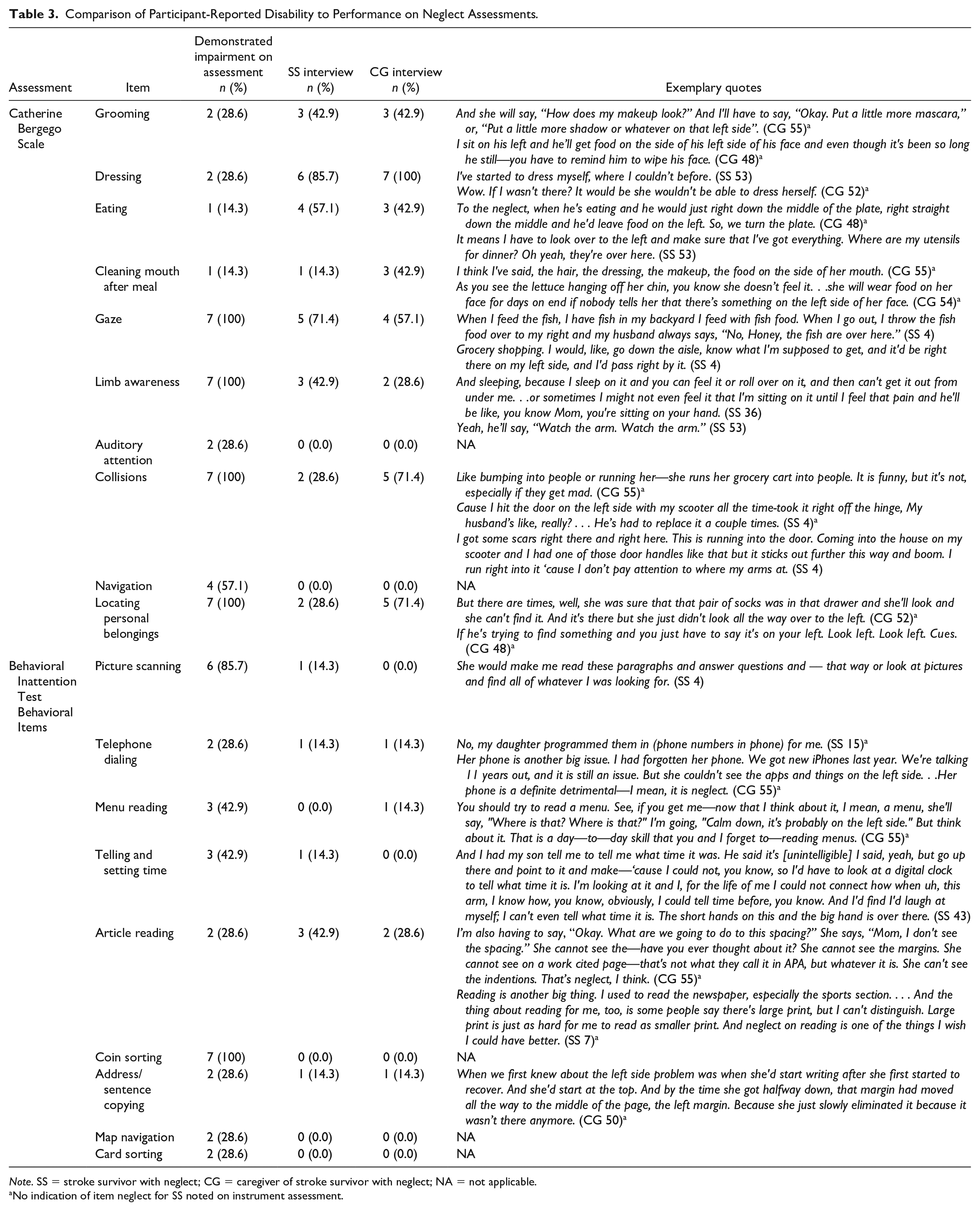
Note. SS = stroke survivor with neglect; CG = caregiver of stroke survivor with neglect; NA = not applicable.
No indication of item neglect for SS noted on instrument assessment.
Qualitative
Neglect was a major theme evident in the interview data from both stroke survivors and their caregivers. Within this predominant theme, subthemes related to safety, impact on quality of life, and challenges were consistently noted across participant interviews. A major finding from the qualitative interviews included safety-related concerns secondary to neglect that are not captured by current assessments. Caregivers expressed safety concerns for the stroke survivor and for those around them, had concerns in their ability to safely navigate through the house or in public, and concerns with bathing (i.e., falls), and cooking. Stroke survivors shared several examples of injuries sustained because of their neglect. Driving was noted as a major safety concern among both caregivers and stroke survivors: If he’s in a cart at Walmart or something, you’ve got to watch how he’s driving because he’ll run kids over. (CG 48) I ran into the backend of a policeman—– who stopped in the middle of the road. But I didn't realize he was stopped. I didn't even see the blue lights. (SS 4) I pray when she goes out of the driveway, look to your left, look to your left. . . . Her parking is really bad too. I forgot about that. She's had several fender benders because of her left-side neglect. (CG 55) Well, I often wonder, you know, she can't walk and they've never taught her how to crawl and I often wonder if a fire was to happen how would she get out? I just have no idea how she'd get out ‘cause she just end up sitting or laying wherever she's at and burning. (CG 49) And I don't realize I'm there till, like, sometimes I'm going between two trees with the golf cart and the next thing you know, that tree is right in front of me. See. And most times I can stop the cart before I hit the tree. (SS 7) There have been times where (Spouse) and I will be driving. He'll say oh, did you see those kids over there? I'd say no. I just don't see them at all because I typically don't turn that way to look. (SS 9)
In addition, safety-related concerns also included their ability to be active participants in family engagement activities. For example, one participant shared concerns over playing with grandchildren because of safety issues or potentially hurting a crawling baby on the floor or being unable to carefully hold the child: I just want to pick her up and my son has to like hold her up and I can hold her up with one arm and stuff. But ever since she was a little baby I couldn’t, you know, I couldn’t. And, and I didn't dare and then I worry about if she’s playing on the floor and stuff, you know. And I want to play with her I don’t wanna get, you know, step on her or something like that. (SS 43)
Throughout the qualitative interviews, participants provided numerous examples of neglect, many of which were not evident during the administration of the quantitative assessments. For example, neglect in dressing was identified for two stroke survivors (43 & 53) on the CBS; however, within the interviews, an additional four stroke survivors (4,9,15, & 36) and five caregivers (48, 49, 50, 51, & 52) reported impairments in dressing that affected daily life and independence although these participants scored highly on these items during testing. Exemplary quotes for dressing and reported items are included in Table 3.
Beyond the traditional deficits assessed, participants discussed how neglect had a strong negative impact on their ability to engage in school, work, or family activities. These affected stroke survivors’ academic pursuits and employability, resulting in economic stressors and logistical care considerations for caregivers, and ultimately posed concerns for the entire family unit: No, um, math so if we’re doing, um, a lot of stuff we’re doing from left to right. I’m not, I’m missing some of the problems on the left. (SS 36) The big picture-because it just is you think okay. There goes his job, you know . . . what’s going to happen? (CG 48) I was only 54. I was still working and so then you have to get somebody to stay with him. (CG 48) When (SS’s name) first recovered from the stroke and she was going back to doing her teaching and some of her other things that she does, I tried to tell everybody—everybody said oh, look, she’s doing great. She’s going to be fine. No, no, no, no. Please don't do that to yourself, because you’re going to be wrong. She’s not going to be fine. This has changed. She has changed. You need to understand. And they refused. (CG 50)
In addition to direct impact on educational and work-related concerns, participants shared implications of neglect on household activities and family responsibilities beyond the scope of current assessment instruments: Not sometimes washing dishes, but I think it might just be the way our sink is set up. I kind of cheat with that too, because I just put the dishes all in the right side now. (SS 36) Like I get mail in and sit with my—and have somebody do some work for me and they send me a bill and I want to make sure that bill is right. See, and I turn all my paperwork over to that when I pay a bill to my youngest daughter. . . . I used to write all the checks and everything like that before I had the stroke, but she takes care of that now. (SS 7)
Qualitative findings identified challenges related to neglect that were sometimes captured by the neglect assessments but also expanded understanding on the degree neglect had on daily life for both the stroke survivor and their primary caregiver. In the interviews, participants more frequently discussed challenges related to items on the CBS than items on the BIT (Table 3). SS most commonly discussed challenges related to dressing and gaze and rarely discussed challenges related to reading a menu, sorting coins/cards, navigating a map, or auditory attention. CG most commonly discussed challenges related to dressing and locating personal belongings and rarely discussed any challenges related to items on the BIT. Higher numbers of participants reported deficits during the interviews in the areas of grooming, dressing, eating, and cleaning mouth after meals than identified on the CBS. Notably, while some overlap exists between instruments and participant self-report, there was considerable variation.
Discussion
SS and CG identified a wide range of examples of how neglect affects daily life and it is clear that neglect, at least within our sample, contributes to participation restrictions (e.g., work, school, family relationships, leisure activities, religious activities) far beyond ADLs (e.g., self-care, mobility). There were many participation restrictions that were not represented by the commonly used behavioral neglect assessments. Clinicians should recognize the potential impact of neglect and consider these findings when working with SS and CG. Clinicians should ask clients and caregivers about the impact of neglect on participation and IADLs to ensure that they are adequately addressing neglect when providing intervention.
A major theme that emerged was that there were safety concerns for not only the SS but also for family members and members of the community. Our findings coincide with a study by Klinke et al. (2016) that found significant personal safety issues due to cognitive impairments (e.g., memory, anosognosia) were reported by SS upon discharge from inpatient rehabilitation to home. However, our results uniquely highlight that there are not simply personal safety costs that need to be considered. While it is possible that these challenges emerged after SS no longer received rehabilitation services, there is a need for rehabilitation professionals to assess and address these safety issues in the chronic stage of stroke recovery. In our study, safety concerns related to driving were particularly prevalent and many SS had traffic accidents because of their neglect. Interestingly, many of these same individuals reported that the SS continued to drive and legally had their driver’s licenses, despite driving-related performance deficits. Some of these same SS even participated in driving rehabilitation assessments and passed testing per their report. Previous studies have shown that cognitive and visual perceptual impairments, including neglect, can predict fitness to drive status (Akinwuntan et al., 2006; Shimonaga et al., 2020) and clinical practice guidelines indicate that individuals post-stroke should undergo a thorough driving evaluation to assess for these impairments (Winstein et al., 2016). However, driving evaluation protocols (i.e., clinical assessments, on-road testing) and state regulations in the United States regarding driving after stroke vary considerably. Some countries in the World automatically restrict driving for a period of time after stroke until further evaluation and recommendations can be made, yet adherence to these restrictions remains an issue (Vander Veen & Rudman, 2022). While there are a number of barriers (e.g., public policy, funding, lack of education) to having all stroke survivors undergo driving evaluations, driving rehabilitation programs that are evaluating stroke survivors may need to include more extensive testing for neglect to ensure that it is safe for them to resume driving (Vander Veen & Laliberte Rudman, 2022).
Although many of the themes (related to activity limitations) identified were represented by the behavioral neglect assessment items, it is still important to recognize the overall difficulty of these items may not reflect the difficulty of the daily activities described by participants in the interviews. For example, participants described the challenges associated with grocery shopping and ambulating without colliding into other people or displays. While there is an item on the CBS that examines collisions, this item is observed in a much less dynamic (i.e., less difficult) environment than a busy grocery store setting.
Our findings coincide with previous studies that demonstrate how performance on neglect assessments can be inconsistent and suggest that the item difficulty for these assessments may not be sufficiently challenging (Azouvi et al., 2006; Grattan & Woodbury, 2017). SS had difficulty performing items on the CBS but had much less difficulty completing items on the BIT. In fact, the majority of the SS would not have been characterized as having neglect (based on cutoff scores) if the BIT alone was used to characterize the sample. It can be inferred that the BIT items were either too easy for the SS or that these items do not reflect the challenges they experience because of their neglect. Our qualitative results support this notion as the responses did not consistently represent the items on the BIT. We had many more themes and quotes that aligned with the items represented on the CBS than the BIT. Interestingly, we had examples where participants reported difficulty performing an activity due to their neglect in their day-to-day life but performed well on the assessment item itself.
While it is clear that neglect negatively affects activity and participation, existing clinical assessments may not be measuring neglect-related disability sufficiently. A recent scoping review of neglect measures also found that while an abundance of neglect assessments exists, the overwhelming majority are impairment-based measures that do not address participation, nor do they measure various subtypes of neglect (Williams et al., 2021). Thus, it is important that assessments that are developed address participation, IADLs, and include items that measure various neglect subtypes. Given the potential challenges associated with standardizing a comprehensive IADL assessment, it may be useful that a checklist of IADLs be developed to identify how neglect affects IADL performance. It is also important that researchers are mindful of the barriers (e.g., time constraints, lack of training) that clinicians face in implementing assessments in practice (Vancleef et al., 2022).
A limitation of this study was the small and homogeneous sample. While data saturation was achieved, a larger-scale study with inclusion of more diverse populations is warranted. Among our participants, SS largely demonstrated mild neglect on the behavioral measures. Thus, SS who have more severe neglect or CG for someone with more severe neglect may have different experiences that are not represented. It is also possible that participation in the CBS and BIT prior to the interviews primed the SS to discuss related experiences and that this influenced the results. Although the qualitative interviews focused on neglect, it is important to recognize that most SS also have additional co-existing impairments (e.g., motor, cognitive, sensory). Thus, participant responses often reflected the impact of multiple impairments and did not exclusively focus on neglect. It also may have been difficult for SS and CG to distinguish whether it was neglect or another impairment that was contributing to activity limitations. SS may have also had anosognosia, which may have limited their perspective and insight into how neglect affects their daily life (Vossel et al., 2013). For example, an SS with anosognosia may not recognize that they are having difficulty managing their finances because of their neglect. Although we included CG perspectives to address this potential shortcoming, this is a potential limitation. Finally, it must be acknowledged that we do not necessarily have an exhaustive report of how neglect affects SS and CG. Future studies may examine the item difficulty of behavioral neglect assessments to ensure that clinicians can adequately measure neglect and capture the extent to which neglect is affecting SS. In addition, exploration among a larger sample comparing levels of impairment may expand understanding of the impact neglect has on IADLs and participation and the usefulness of these instruments in assessing the impact of neglect across severity levels. These findings provide an initial first step to inform future studies aimed at developing more comprehensive neglect assessments for stroke survivors.
Conclusion
This study highlights the impact neglect has on IADLs and participation after stroke and demonstrates that existing clinical assessments may not be measuring neglect-related disability adequately. Thus, clinicians may not fully realize how neglect is affecting a client with stroke and as a result fail to address neglect-related disability sufficiently in treatment. Similarly, a clinician may not have the means to measure and document response to intervention adequately. Although preliminary, these findings emphasize the need for standardized assessments that comprehensively assess the impact of neglect on the occupational performance of stroke survivors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the U.S. Department of Veterans Affairs under grant number 1 IK2 RX002420-01A2; NIH/NCATS grant number UL1TR001450; and an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number P20GM109040.
Research Ethics Section and Patient Consent
All participants provided informed consent and adhered to the Medical University of South Carolina Institutional Review Board, Protocol #00044531.