
Abstract
Telehealth delivery of Lifestyle Redesign®, an occupational therapy intervention framework addressing health and quality of life among people with chronic conditions, is understudied. The objective of this study was to evaluate the effectiveness, satisfaction, and engagement of telehealth Lifestyle Redesign for young adults with diabetes. Using process data from two randomized controlled trials, we compared in-person and telehealth intervention effects. Among telehealth clients, effectiveness was assessed using pre-post changes in occupational performance, occupational satisfaction, and health management; a survey captured telehealth satisfaction. Attendance and engagement in in-person versus telehealth therapy were compared. Preliminary results indicate telehealth clients had significant increases in occupational performance, occupational satisfaction, and health management (all p < .02), and high levels of telehealth satisfaction. Intervention engagement (p = .59) and attendance (p = .42) were similar across treatment modalities. Telehealth delivery of Lifestyle Redesign occupational therapy is feasible and potentially efficacious, and continued advocacy is needed to ensure access to occupational therapy through telehealth.
Keywords
Introduction
Type 1 diabetes (T1D) is one of the most common chronic illnesses of childhood, estimated to impact around 244,000 individuals in the United States under the age of 20 (Centers for Disease Control and Prevention, 2022). Research on the management of T1D has focused largely on the needs and experiences of children and their families, with less attention paid to the challenges of young adulthood. This developmental phase is characterized by greater autonomy in disease management; educational, employment, and living situation transitions; and a transition from pediatric to adult health care systems. These transitions foster a challenging time for diabetes care and management (Monaghan et al., 2016; Sauder et al., 2021), illustrated by less frequent health care visits, higher HbA1c, and the highest risk for hypoglycemia and diabetic ketoacidosis (Foster et al., 2019; Sauder et al., 2021). More concretely, only around 17% of young adults aged 18 to 25 and 30% of young adults aged 26 to 30 with T1D meet the current recommendation of an HbA1c of ≤7.0% (Monaghan et al., 2016). These challenges are compounded by stressful life events that further diminish self-management and raise HbA1c (Joiner et al., 2018; Vigen et al., 2018). Young adults with T1D experience greater fatigue and dysfunction in physical, emotional, and work functioning than their peers without diabetes (Bronner et al., 2020), which contributes to a greater incidence of mental health conditions including depression and anxiety (Monaghan et al., 2016).
Interest in occupational therapy (OT) for T1D service provision has grown due to the profession’s emphasis on performance patterns (American Occupational Therapy Association, 2020) and the impact of everyday activities on health and well-being. In OT practice, the individual, task, and environment are analyzed to identify performance barriers and facilitators (Cahill et al., 2016). This approach is relevant to T1D given the importance of daily self-monitoring, dietary management, and medication adjustment. Several studies have demonstrated that OT is feasible and effective for improving quality of life and blood glucose levels among individuals with diabetes (Bahadır Ağce & Ekici, 2020; Pyatak et al., 2018; Pyatak et al., 2019; Smallfield et al., 2021). By supporting the performance of occupations that impact T1D management, the unique perspective of OT to promote occupational engagement, through the transactional nature of activities (Dickie et al., 2006), can serve as a valuable addition to diabetes care teams.
Due to the COVID-19 pandemic, OT saw an increase in telehealth service provision. OT practice adapts well to the format given that telehealth use can facilitate skill development and the creation of healthy habits and routines in their natural context. Telehealth also improves access to services and prevents delays in receiving care (Telehealth in Occupational Therapy, 2018). Telehealth OT has been implemented successfully in a variety of settings including home health, dementia care, primary care, mental health, and chronic condition management (Albritton et al., 2021; Laver et al., 2020; Reay et al., 2021; Tenforde et al., 2020; Zahoransky & Lape, 2020).
Given the success of other telehealth T1D interventions (Bakhach et al., 2019; Bassi et al., 2022; Jewell et al., 2022; Tchero et al., 2018), and preliminary evidence supporting the role of OT in diabetes care (Bahadır Ağce & Ekici, 2020; Pyatak et al., 2018; Pyatak et al., 2019; Smallfield et al., 2021), telehealth OT has the potential to be a powerful intervention for young adults with T1D. One approach for providing occupational therapy services is Lifestyle Redesign 1 (Pyatak et al., 2022) wherein chronic condition management is addressed by supporting sustainable habit and routine creation while promoting clients’ autonomy. This approach has been effective in improving health and quality of life among people with diabetes when delivered in-person (Pyatak et al., 2018; Pyatak et al., 2019), and there is preliminary data demonstrating Lifestyle Redesign ’s effectiveness through telehealth (Schepens Niemiec et al., 2021).
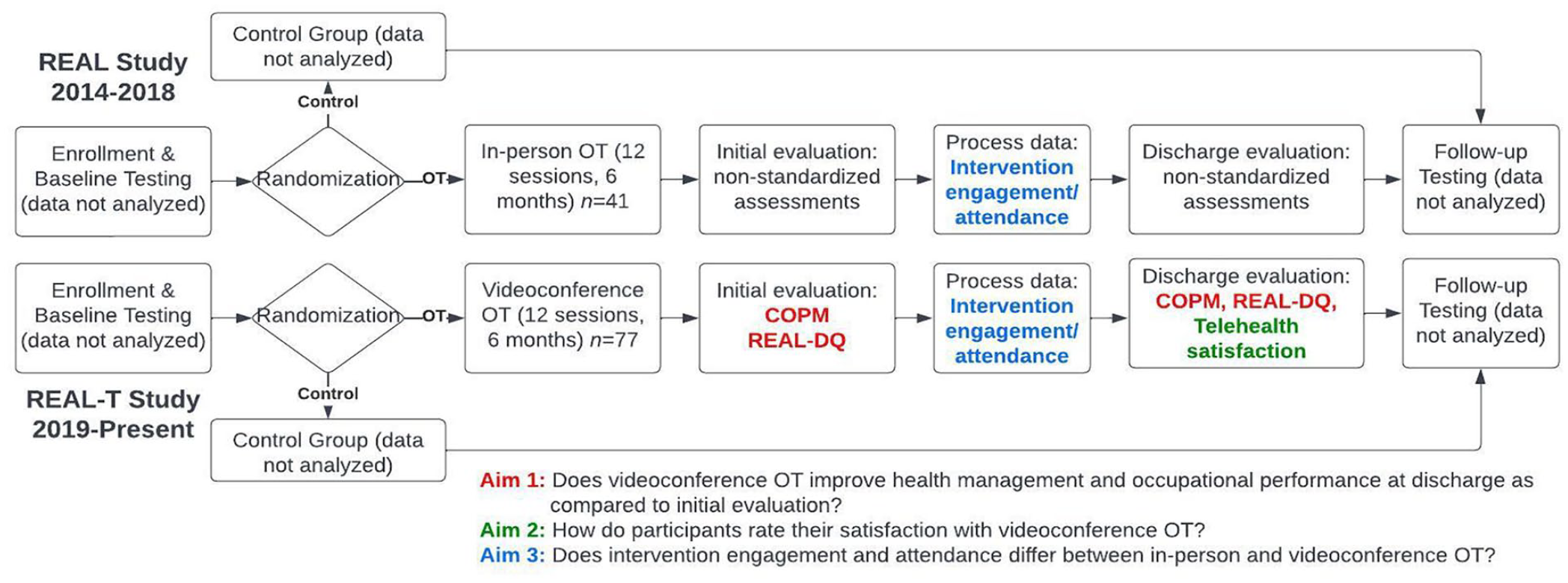
The emerging intersections of diabetes management, OT, Lifestyle Redesign, and telehealth led to the development of the Resilient, Empowered, Active Living – Telehealth (REAL-T) Study. The REAL-T study’s primary aim is to evaluate the efficacy of the REAL intervention, (Pyatak et al., 2018) as administered through telehealth, in improving blood glucose levels (HbA1c) and psychosocial well-being among young adults with diabetes. The REAL-T study is a telehealth adaptation of the previously conducted, REAL study, which found that Lifestyle Redesign OT was efficacious in improving blood glucose levels and psychosocial well-being (Pyatak et al., 2018). Using preliminary data from REAL-T and data from the completed REAL study, this article reports on three primary aims:
First, to examine the effectiveness of telehealth-delivered Lifestyle Redesign OT in addressing occupational performance and satisfaction among young adults with T1D
Second, to assess client satisfaction for telehealth-delivered Lifestyle Redesign OT
Third, to compare engagement and attendance of telehealth versus in-person OT as provided in the REAL-T and REAL studies.
Method
Study Design
This study presents a primary analysis of pre-post, descriptive data from the REAL-T study, an ongoing clinical trial (NCT04023487) evaluating the REAL intervention as delivered through telehealth. In addition, a secondary analysis of the previously conducted REAL study was run to compare in-person versus telehealth care delivery. Both the REAL and REAL-T studies were two-arm, parallel-group, randomized controlled trials in which participants were assigned in a 1:1 ratio to either OT intervention or usual care (see Figure 1). Both studies were approved by the USC Institutional Review Board (#HSC-18-00633), and all participants provided informed consent before engaging in study activities. As the REAL-T trial is currently ongoing, this analysis examined outcomes from participants who had completed the 6-month OT intervention as of 08/01/2022. Details regarding the methodology and outcomes of the REAL study, including its CONSORT diagram, have been published elsewhere (Pyatak et al., 2017; Pyatak et al., 2018); below we briefly review relevant aspects of both the REAL and REAL-T studies.
A Comparison Between the REAL Study and the REAL-T Study Intervention Designs
Participants
Eligibility criteria for participants in both studies included the following: were aged 18 to 30 years old, fluent in English or Spanish, and had been diagnosed with diabetes for at least 12 months. REAL study participants resided in the greater Los Angeles area, whereas participation in REAL-T was initially restricted to greater Los Angeles and later expanded to include residents of any state where the study’s occupational therapists were licensed (CA, CO, OR, TX, and WA). Participants in REAL had HbA1c levels ≥8.0% and had low socioeconomic status, whereas REAL-T participants had HbA1c levels ≥7.5% and no socioeconomic inclusion criteria. Participants in both studies were excluded if they were currently pregnant or planned to become so in the next 12 months, or had a cognitive impairment or severe disability limiting life expectancy.
Procedures
Participants in both studies were recruited from local clinics and social media advertising. After providing informed consent, participants completed a baseline assessment battery including an HbA1c test and demographic and psychosocial surveys. After participants completed baseline measures, participants were randomized through the computerized Research Electronic Data Capture (REDCap) database management system (Harris et al., 2009) and informed of their treatment assignment (OT or usual care). In both studies, interventions were administered by licensed occupational therapists trained in Lifestyle Redesign and motivational interviewing. Participants completed approximately 10 to 16 sessions lasting approximately 1 hour each over 6 months. In REAL-T, treatment sessions were conducted individually over HIPAA-Compliant Zoom allowing for greater individualization and flexibility in scheduling. The study intervention manuals (Pyatak, Carandang, & Davis, 2015) included modules addressing Healthy Habits and Routines, Managing Diabetes, Emotions and Well-Being, People and Places, and Accessing Care. Module topics were developed based on reviewed evidence-based practice, the Lifestyle Redesign Manual (Clark et al., 2015), and previous research with the target population (Carandang & Pyatak, 2018; Pyatak, 2011; Pyatak et al., 2014). It includes suggested activities, handouts, and resources to support individualized goals.
Measures
Canadian Occupational Performance Measure
The Canadian Occupational Performance Measure (COPM; Law et al., 2014) is an assessment tool that measures perceived occupational performance and satisfaction over time. The COPM has previously been used sparingly to measure functional progress among individuals with T1D, but more frequently among those with type 2 diabetes (Cahill et al., 2016; Marinho et al., 2016; Reis et al., 2019). In this study, it was administered at OT evaluation and discharge. The COPM guides clients to self-identify areas of occupational deficit, creating a person-centered and occupation-based measure. Scores range from 1 to 10, with higher scores indicating better-perceived performance and satisfaction. Changes in pre-post scores are used to track progress and intervention effectiveness.
REAL Diabetes Questionnaire (REAL-DQ)
The REAL-DQ is a health management assessment designed for internal use within the REAL and REAL-T studies and was administered at OT evaluation and discharge. The tool was created to identify clients’ knowledge and beliefs related to diabetes, to aid in intervention planning and tracking progress. Questions are clustered within the REAL and REAL-T intervention domains: healthy habits and routines, managing diabetes, emotions and well-being, interactions with others and the environment (“People and Places”), and accessing care. Participants ranked six items per category using a five-point Likert-type scale where 1 indicates “Disagree Strongly” and 5 indicates “Agree Strongly.” Scores ranged between 6 and 30 with higher scores reflecting improved adaptation to living with diabetes. Changes in scores from pre- to post-intervention suggest intervention effects on diabetes management. The REAL-DQ is accessible as Supplemental Table 1.
Telehealth Satisfaction Survey
When discharged from OT, participants were provided a questionnaire that captured personal characteristics, quality, and comfort during OT sessions, an impression of the OT over telehealth, comparisons between in-person and telehealth provision, and intention to utilize telehealth in the future. The survey included five-item Likert-type scales ranging between “Strongly Disagree” and “Strongly Agree” as well as “Yes” and “No” questions. The Telehealth Satisfaction Survey is accessible as Supplemental Table 2.
Intervention Engagement and Attendance
Intervention engagement and attendance were evaluated by reviewing OT documentation from the REAL and REAL-T studies. The number and duration of sessions were extracted from treatment notes taken during both studies. Participant engagement was tracked through OT discharge notes and categorized as complete (i.e., participated in as many OT sessions as were offered), withdrew or lost to follow-up (i.e., received some OT sessions before requesting discontinuation or ceasing responding to scheduling attempts), or did not participate (i.e., were unreachable or declined to engage in any OT sessions).
Data Analysis Plan
COPM and REAL-DQ
Data were extracted from REDCap, input into SAS, and mixed models were run. Repeated measures data result in non-independence in the data set; each person’s score is correlated with their other score. In other words, there is a correlation between each participant’s COPM evaluation and discharge scores and REAL-DQ evaluation and discharge scores. Mixed models manage this through the estimation of random effects for model intercepts and the slopes of any predictor variables. That is, they account for these person-level effects. In these models, the only predictor is time (Discharge vs. Evaluation). Across all outcomes, the random effects for the slopes were indistinguishable from zero, so the random slopes were excluded from the model. Random intercepts were retained, although most were non-significant.
Telehealth Satisfaction Survey
Frequency distributions were generated from the Telehealth Satisfaction Survey to provide an overview of participants’ satisfaction with telehealth.
Intervention Engagement and Attendance
A Fisher Exact Test was used to evaluate differences in the proportion of participants who completed, withdrew, were lost to follow-up, or never initiated treatment in each study. Independent sample t tests were used to compare the number and duration of treatment sessions across the two studies.
Results
Overall, 118 participants were included in the analyses: 77 from REAL-T and 41 from REAL. Because data collection is ongoing in REAL-T, some variables contained incomplete data and thus included fewer participants in the analysis. These incomplete data sets were included to maintain transparency in the research, limit bias, and maintain the principles of intent-to-treat.
Overall demographic characteristics were as follows: REAL-T participants were 23.8 (±3.7) years old; 57.1% female, 37.7% male, and 5.2% non-binary or other gender identities. Their self-identified racial/ethnic backgrounds were 41.6% White, 40.3% Hispanic/Latinx, 2.5% other, and 15.6% more than one racial/ethnic group. The majority resided in California (81.9%), with 10.4% from Texas and 7.7% from other states (Colorado, Oregon, and Washington). The 41 REAL participants were 23.3 (±3.6) years old, 53.7% female, and 46.3% male. 2 Their self-identified racial/ethnic backgrounds were 82.9% Hispanic/Latinx, 7.3% White, 4.9% Black, and 4.9% other or more than one racial/ethnic identity; all resided in California at the time of study participation.
Effectiveness
COPM and REAL-DQ results are presented in Table 1. Overall, participants significantly increased in both occupational performance (p < .0001) and occupational satisfaction (p < .0001). Notably, of the 70 participants who completed the COPM at evaluation, only 40 had COPM data at discharge, indicating a 42.9% loss to follow-up. Baseline scores differed between those who had follow-up COPM data and those who did not (participation: 3.69 vs. 4.02, p = .03; satisfaction: 3.37 vs. 3.67; p = .11), with participants who scored higher at baseline being less likely to complete follow-up measures. For the REAL-DQ, similar trends were noted, with statistically significant improvement noted in all subscales (range: p = .017 to p < .0001), and a large proportion of participants with missing data at discharge. When comparing participants who had follow-up data to those who did not, baseline REAL-DQ scores on three subscales demonstrated marginally significant differences (Healthy Habits, p = .06; Managing Diabetes, p = .04; Emotions and Well-being, p = .06) with participants who scored higher at baseline being less likely to complete follow-up measures. In contrast, the People and Places and Accessing Care subscales did not have significant differences (p = .95 and p = .54, respectively).
Telehealth Study Participant Changes in COPM and REAL-DQ Scores From Evaluation to Discharge to Measure Telehealth Effectiveness.
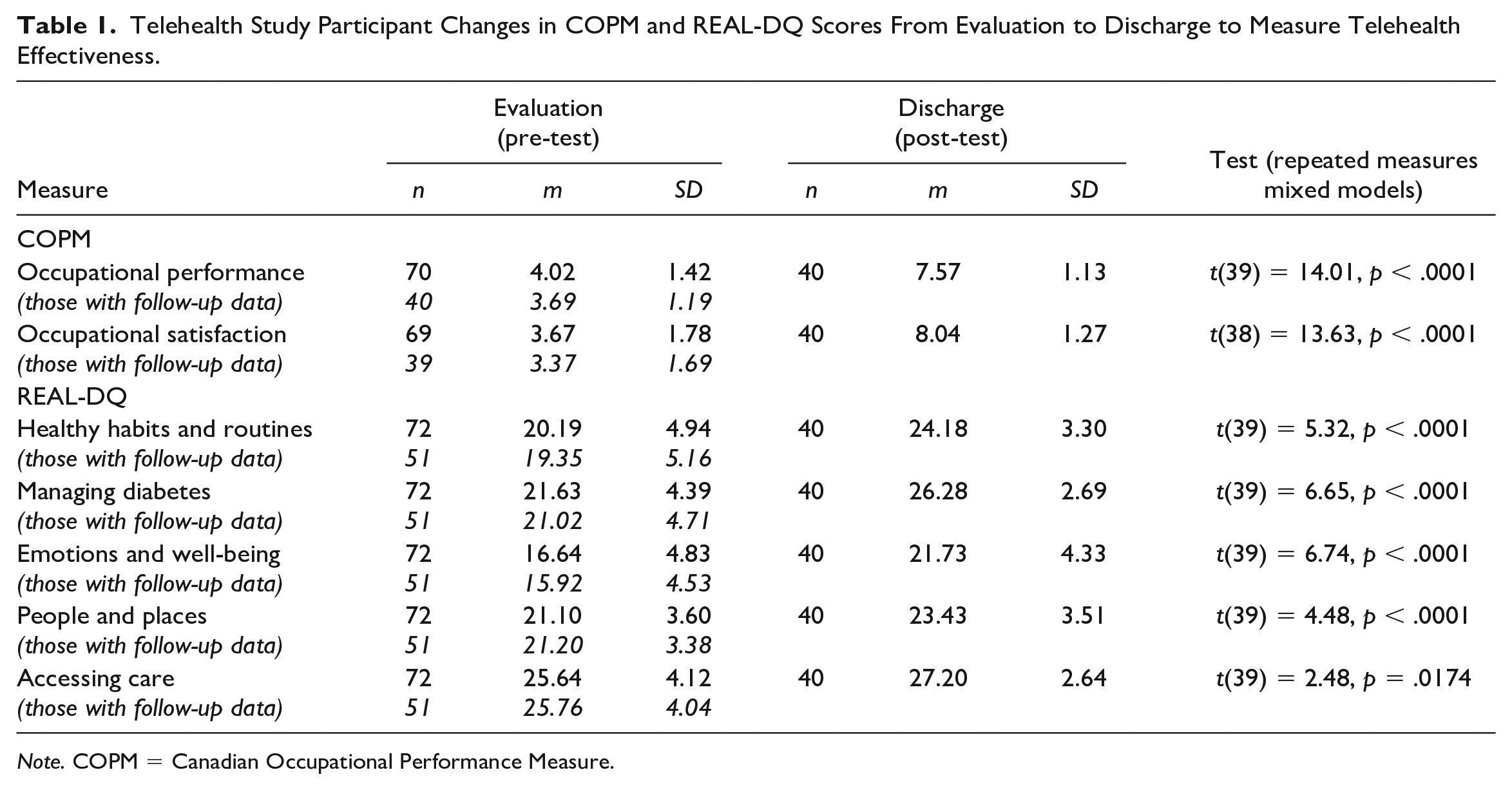
Note. COPM = Canadian Occupational Performance Measure.
Satisfaction
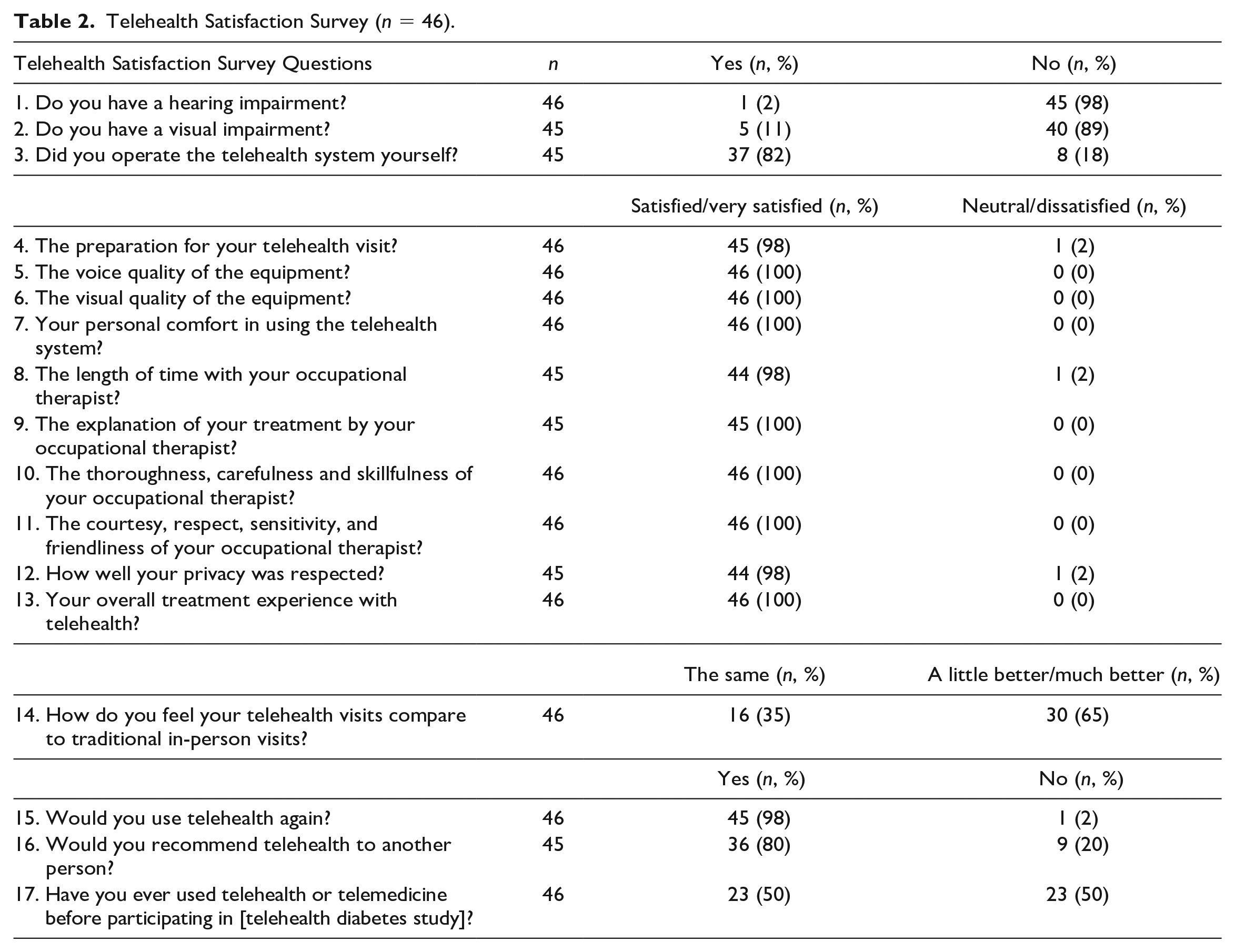
Satisfaction with telehealth is presented in Table 2. Overall, the majority of participants were very satisfied with the technical components of telehealth (visual, audio, user interface) with satisfaction ranging from 98% to 100%. Regarding treatment, 91% of respondents were very satisfied overall with their experience using telehealth, 98% of respondents would use telehealth again, and 80% would recommend it to others. When asked to evaluate their satisfaction with telehealth versus in-person care, 35% indicated that the experience was the same while 65% of respondents felt that telehealth was a little better (28%) to much better (37%) than traditional service provision.
Telehealth Satisfaction Survey (n = 46).
Engagement
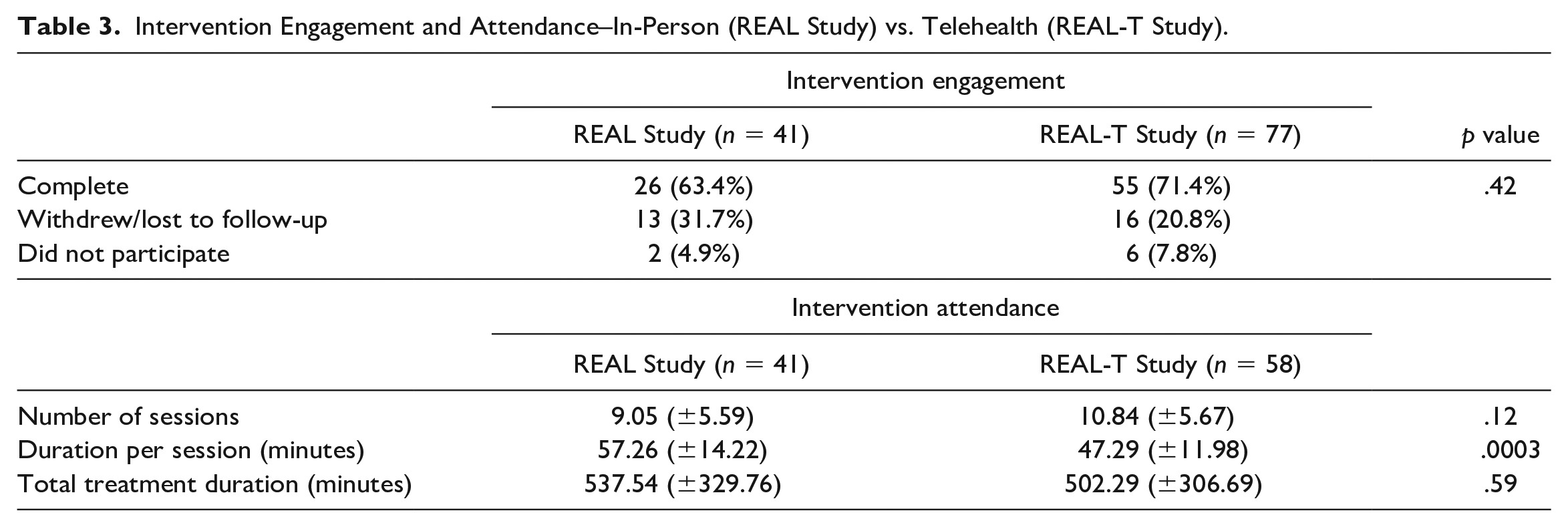
A comparison of intervention engagement and attendance in-person (REAL) and through telehealth (REAL-T) is presented in Table 3. There was no difference in the proportion of participants who completed the intervention, withdrew or were lost to follow-up, or received no occupational therapy (p = .42). Similarly, there was no difference in the overall amount of therapy received (p = .59). However, therapy time was distributed differently: telehealth clients engaged in more sessions (10.84 vs. 9.05; p = .12) which were significantly shorter in duration than in-person sessions (47.29 vs. 57.26 min; p = .0003).
Intervention Engagement and Attendance–In-Person (REAL Study) vs. Telehealth (REAL-T Study).
Discussion
This article aimed to explore effectiveness, satisfaction, and engagement in telehealth-delivered, Lifestyle Redesign OT for young adults with T1D. The study demonstrated that telehealth OT is satisfactory and improves health management, occupational performance, and occupational satisfaction. These findings support previous Lifestyle Redesign studies for individuals with diabetes (Pyatak et al., 2018; Pyatak et al., 2019) that showed lifestyle modifications can improve diabetes management while demonstrating that these benefits can be fostered through telehealth care delivery. These results, demonstrated through the REAL-DQ, also build upon literature on young adults living with T1D that aims to address physical, emotional, and work functioning through improved diabetes management skills (Bronner et al., 2020). As the COPM addresses participant-identified occupational concerns related to diabetes and the REAL-DQ addresses diabetes management skills, together these measurements target the areas that are most important to participants and diabetes management.
Effectiveness
This study showed improvements in occupational performance and satisfaction supporting previous research demonstrating that a COPM-directed intervention improves diabetes outcomes (Marinho et al., 2016). Results also align with telehealth research demonstrating improved diabetes management skills (Bisno et al., 2021). These positive results contained interesting patterns of missing data. Those with lower scores on the COPM and REAL-DQ at baseline were more likely to have follow-up scores at discharge, perhaps because they recognized a greater need for OT services to support their health management and occupational performance, in contrast to participants with higher COPM and REAL-DQ scores. An alternate interpretation is that those who were lost to follow-up rated themselves more highly due to having less insight into their occupational performance and health management challenges. Thus, they may be more likely to opt-out of OT services, given a more limited awareness of the potential to benefit.
Satisfaction
Satisfaction with telehealth as a care delivery modality was markedly high in REAL-T. One explanation for this outcome is that during the COVID-19 public health emergency, telehealth became the primary modality for health care providers, although this seems unlikely. This may be true for technical measures of telehealth such as visual, audio, and systems utilized as there was increased use of technology in this regard during the COVID-19 public health emergency (Samson et al., 2021). However, participants were encouraged in the telehealth satisfaction survey to reflect on all of their previous in-person health care experiences, their telehealth treatment experience, and future health care utilizations. This captures a more longitudinal perspective that may be less impacted by the immediate context of the pandemic. While common barriers to telehealth, including a lack of reliable internet access and privacy concerns, have been identified in other literature (Garcia et al., 2021), participants did not note these concerns when provided the opportunity to identify personal challenges with telehealth.
Engagement
Participants in both REAL and REAL-T demonstrated equivalent time spent in therapy. Notably, the absence of follow-up data at discharge, as discussed previously, was not a result of treatment modality, as the rate of loss to follow-up did not differ between the in-person and telehealth interventions. In addition, there was no difference in the total duration of treatment in both interventions. Previous literature has shown conflicting findings regarding whether patients are more likely to attend telehealth as compared with in-person visits (Chakawa et al., 2021; Childs et al., 2021). It is unclear whether, and to what extent, attendance in REAL-T is related to the study’s context. Notably, the majority of intervention sessions for the REAL-T study took place during the COVID-19 public health emergency, as participants enrolled between October 2019 and November 2022. Thus, these circumstances should be taken into consideration when assessing participant engagement and outcomes. For example, participants’ willingness to engage in shorter, more frequent sessions as compared with in-person therapy could be motivated by a desire to address social isolation or psychosocial stressors caused or exacerbated by the pandemic.
Limitations
As the REAL-T study is still ongoing, only a partial sample of those who had completed the 6-month intervention portion of the study was included in this analysis. Although pre-intervention measures were compared between those who had follow-up data and those that did not, the claims made in this article should be interpreted with caution given that final analyses are still pending. Because the study is ongoing, there were also instances where incomplete data entry contributed to missing data, further decreasing statistical power and generalizability. Finally, REAL-T outcomes examined in this article were only analyzed on a pre-post basis because the reported measures were not administered to the usual care control group. Thus, findings should be interpreted with caution as we cannot rule out alternative explanations for participants’ improvement, such as regression to the mean. Future analyses will examine additional outcomes such as HbA1c and psychosocial well-being, in a more methodologically rigorous fashion, including a comparison to a randomized control group.
Conclusion
Although preliminary, this study suggests telehealth OT for diabetes is effective, satisfactory, and has an equivalent engagement to in-person OT. Telehealth OT appears to promote improvements in occupational performance and satisfaction as well as diabetes management skills, in a satisfactory, convenient, and accessible format. Specifically, increases in occupational performance and satisfaction, diabetes management skills, and attendance were shown. These findings may be useful to practitioners, payers, and policymakers who are hesitant to provide or authorize such treatments. Telehealth appears to promote significant improvements in occupational performance and satisfaction as well as diabetes management knowledge and skills, in a highly satisfactory, convenient, and accessible format. This study demonstrates the potential benefits of telehealth OT, given its impact on occupational engagement and diabetes management. Telehealth increases this impact, as it is significantly less constrained by time and geographic barriers to care compared with in-person services (Jewell et al., 2022). When considering how best to provide care to individuals with low prevalence conditions, such as type 1 diabetes, who may not live near an occupational therapist with training in this practice area, telehealth is an essential tool to promote access to care.
Supplemental Material
sj-docx-1-otj-10.1177_15394492231172933 – Supplemental material for Telehealth Lifestyle Redesign Occupational Therapy for Diabetes: Preliminary Effectiveness, Satisfaction, and Engagement
Supplemental material, sj-docx-1-otj-10.1177_15394492231172933 for Telehealth Lifestyle Redesign Occupational Therapy for Diabetes: Preliminary Effectiveness, Satisfaction, and Engagement by Seth Mitchell, John Sideris, Jeanine Blanchard, Gabrielle Granados, Jesús Díaz and Elizabeth Pyatak in OTJR: Occupational Therapy Journal of Research
Footnotes
Acknowledgements
The study authors would like to thank the investigative team and research participants, and NG Nnoli for assistance in preparing the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institutes of Health/National Institute of Diabetes, Digestive and Kidney Disorders (NIH/NIDDK) (grant no. R01DK116719-01A1).
Research Ethics
All research described in this manuscript was conducted in accordance with ethical principles for the conduct of research as outlined in the Declaration of Helsinki. Study procedures were approved by the University of Southern California’s Institutional Review Boards and all participants provided informed consent. IRB Protocol number: HS-18-00633
Trial Information
Clinical Trial reg no. NCT04023487, clinicaltrials.gov
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.