
Abstract
Background:
Little is known about participation during adverse times.
Objectives:
This study described participation of children with autism aged 6 to 13 during COVID-19 pandemic and examined the extent to which child factors, mother’s own participation, and environmental barriers/supports explain child participation in home and community.
Method:
A total of 130 mothers completed the Participation and Environment Measure for Children and Youth, the Health Promoting Activities Scale, functional issues checklist, and sociodemographic questionnaire.
Results:
Children’s participation frequency and involvement were significantly higher at home than in the community. In both settings, mothers desired change in 71% of activities. Multiple regression models indicated that child’s age and mother’s participation frequency significantly explained child’s home involvement (R2 = 21%), where mother’s participation (frequency) had a unique contribution (ΔR2 = 10.4%) at home but not in the community.
Conclusion:
Findings imply the importance of maternal participation to child’s participation at home and suggest redirecting attention for enhancing family participation as a whole.
Introduction
Participation, defined as involvement in life situations (World Health Organization, 2001), is beneficial for child’s development, well-being, and thriving (King et al., 2003; Weiss & Burnham Riosa, 2015) and is an important outcome in pediatric rehabilitation, including occupational therapy. However, the participation patterns of children with autism, 1 in terms of frequency and diversity of activities done, remain limited, particularly in unstructured, social, and recreational occupations (Hilton et al., 2008; Hochhauser & Engel-Yeger, 2010; Potvin et al., 2013); this tends to further decline as children move into adolescence (Simpson et al., 2019).
Both personal (e.g., functional issues) and environmental factors (e.g., barriers and supports) affect the participation of children with autism, as identified in scoping reviews (Askari et al., 2015; Krieger et al., 2018). Common environmental barriers and/or supports include attitudes, social supports, availability of resources and services, policies, and so on. Family factors, including income (Shattuck et al., 2011) and parental perceptions/beliefs and interests in participation and recreation (Coussens et al., 2020; King et al., 2003), have been well documented to positively affect child participation. However, little is known about the impact of parent’s actual participation, particularly in leisure-oriented and health-promoting nonparenting activities, on the participation patterns of school-aged children with autism across different settings. To our knowledge, two studies (pre-COVID) examined mother’s actual participation among young children: one in Canadian children (mean age = 3.5 years) with various disabilities at home only (n = 236; Williams et al., 2019), and the other among Israeli children (mean age = 4.98 years) with autism (n = 30; Bar et al., 2016). Mothers of children with disabilities are often considered the main caregivers (Bourke-Taylor et al., 2010), and their active lifestyle may influence their child’s participation (Ayvazoglu et al., 2015) as children may begin to adopt participation habits from their mother. Thus, a strong need to better understand the relationship between maternal and child participation in the presence of personal and environmental factors, especially among children in a broader and older age group, exists. Focusing on older school-aged children, aged 6 to 12 (middle childhood), is crucial as this is an important developmental stage of task achievements (e.g., learning physical skills to achieve competence and independence; Havighurst, 1948). It allows examination of participation before entering adolescence, and before the shift in participation (a decline) occurring at age 12 (Jarus et al., 2010).
The pandemic, an exceptional global situation, required families to remain home and follow social distancing rules placed on gatherings, schools, dine-in restaurants, and other venues (Razak et al., 2022), which induced abrupt and greater changes in daily participation (Aishworiya & Kang, 2021). This imposed another layer of complexity on child’s well-being, particularly among those with neurodevelopmental disabilities. Examples include exacerbated mental health symptoms (Masi et al., 2021) and greater barriers in accessing health care services (Eapen et al., 2021). Little is known about the participation patterns of school-aged children with autism during such adverse times. This study, therefore, aimed to (a) describe participation patterns and environmental barriers/supports in home and community during COVID-19, and (b) estimate the extent to which child’s functional issues, income, environmental barriers/supports, and mother’s actual participation can explain frequency and involvement of the child’s participation in home and community activities as well as the number of those activities parents would like to see change, that is, desire for change.
Method
This cross-sectional study, conducted during COVID-19 from December 2020 to May 2021 (nearly 80% of surveys were completed in winter), was approved by several ethics boards. Mother-participants, all residing in Canada and the United States, were recruited from autism-related organizations, special schools (public and private), associations, and research networks. Formal consent was obtained using an online platform, that is, LimeSurvey, by all participants.
Participants
One hundred thirty mothers participated in the study. Mothers were included if they (a) had a child aged 6 to 12 with an autism diagnosis (across the entire spectrum) reported by parents; (b) understood English or French to complete the questionnaires independently; and (c) had access to an electronic device and internet. Mother-participants were excluded if (a) they had a major self-reported health condition as this can affect their own participation and (b) their child had an additional complex neurodevelopmental diagnosis such as cerebral palsy or Down syndrome. Co-occurrence of such conditions was excluded as they may affect participation (Mammad et al., 2019). Children who encountered other conditions such as attention deficit hyperactivity disorder (ADHD) and intellectual disability (ID) were included as these are more common in this population (Påhlman et al., 2020).
Measurements
The Participation and Environment Measure for Children and Youth
To measure participation patterns (i.e., frequency, involvement, and desire for change) and environmental barriers/supports at home and in the community, the English or French-Canadian version of the Participation and Environment Measure for Children and Youth (PEM-CY) was used (Coster et al., 2014). Parents rated their child’s participation using three scales: frequency using an 8-point scale, from never (0) to daily (7); involvement in activities using a 5-point scale, from minimally involved (1) to very involved (5); and whether parents wanted to see a change in their child participation using “Yes” or “No” along with five additional options to clarify the types of change desired. For each setting, mean scores were calculated per each scale; frequency score ranges from 0 to 7 and involvement score ranges from 1 to 5. Number of activities parents desire change was counted and presented in percentages, where higher percentages suggest less satisfaction with the child’s participation (Coster et al., 2014). Environmental factors were measured using 12 items for home and 16 items for community. Examples include physical accessibility, social support, attitudes of others, and the demands of the activity (physical, cognitive, and social). The environmental support and barrier scores for each setting were calculated by counting the environmental items rated as “Usually helps” or “Usually yes” and “Usually makes harder” or “Usually no,” respectively. The number of environment features perceived as barriers or supports to participation per setting were presented in percentages. The PEM-CY has good reliability and validity with internal consistency ranging from 0.59 to 0.91, test–retest reliability ranging from 0.70 to 0.95, and has been successfully used among parents of children with autism (Egilson et al., 2018; Simpson et al., 2019). A French-Canadian version of the PEM-CY is also available.
Health Promoting Activities Scale
Mother’s actual participation frequency in health-promoting activities was measured by the Health Promoting Activities Scale (HPAS; Bourke-Taylor et al., 2013). This brief and psychometrically sound instrument measures the participation frequency in self-selected leisure activities that promote health (e.g., “social activities with people who are important and supportive toward you”). The HPAS includes eight items (or activities) rated on a 7-point response scale from never (1) to once or more every day (7). A sum score is generated ranging from 8 to 56 where a higher score indicates more frequent participation. The HPAS has good internal consistency (0.78) and excellent intraclass correlation (0.9), and its construct validity has been demonstrated (Bourke-Taylor, Law, et al., 2012; Bourke-Taylor et al., 2013). It was also effectively used among mothers of school-aged children with developmental disabilities (Bourke-Taylor, Pallant, et al., 2012).
Checklist of Functional Issues
The complexity of the child’s state was measured by a parent-report checklist of 12 functional issues. It included 12 functional issues (e.g., difficulty paying attention or concentrating; communicating with others; and socializing with other children). Each item/functional issue was rated on a 3-point scale: no problem, little problem, and big problem. The number of functions rated as little problem or big problem were counted, ranging from 0 to 12. This checklist, covering multiple domains of functional issues, is easy to complete and feasible. It has consistently shown the ability to explain participation variance in previous studies (Anaby et al., 2014). Parents also reported on their child’s health condition (e.g., developmental delay, intellectual disability, and attention deficit disorders), selecting up to three health conditions using a list of 13 health conditions.
Demographic Questionnaire
Information on child’s age and sex, household income, region, and type of community was collected using a demographic questionnaire.
Statistical Analysis
Descriptive statistics and paired t tests were used to characterize and compare the patterns of participation of children with autism and environmental barriers/supports in the home and the community settings. Pearson correlation coefficient (between explanatory variables <0.45) and the variance inflation factor (VIF) values (closer to 1) indicated no concern for multicollinearity. Multiple linear regressions were conducted and R2 change was calculated. Explanatory variables were entered in “blocks,” allowing us to test the unique contribution of each factor to the explained variance of each of the three participation outcomes: frequency, involvement, and desire for change. Specifically, in Block 1, income was entered; Block 2 included child factors (i.e., functional issues and age); and Block 3 comprised environment barriers and supports. Mother’s participation frequency was added in the last block, testing the unique contribution of this variable over and above other factors already known to be important. SPSS 27 and R studio were used, and level of significance was set to 0.05 for all statistical tests. A sample of 130 mother-participants provided enough power to model up to six explanatory variables at a conservative effect size (F2 = 0.15) with a power of 0.80 when α = .05 (Green, 1991).
Results
The demographic characteristics of children and mothers are presented in Table 1. The average number of child’s functional issues reported was 7.48 of 12 (SD = 1.84). The median family annual income level fell into a range of CA $30,000 to CA $40,000/year. On average, based on HPAS, mother’s level of participation frequency in health-promoting activities was 35.67 of 56 (SD = 9.22), indicating more than “2-3 times a month” but less than “once a week.” Mother’s participation frequency in each activity is shown in Supplemental Figure 1. Specifically, mothers most frequently participated in quiet and physically inactive leisure activities done alone, with a mean frequency score of 5 (i.e., “once a week”) on a 7-point scale.
Sample Characteristics.
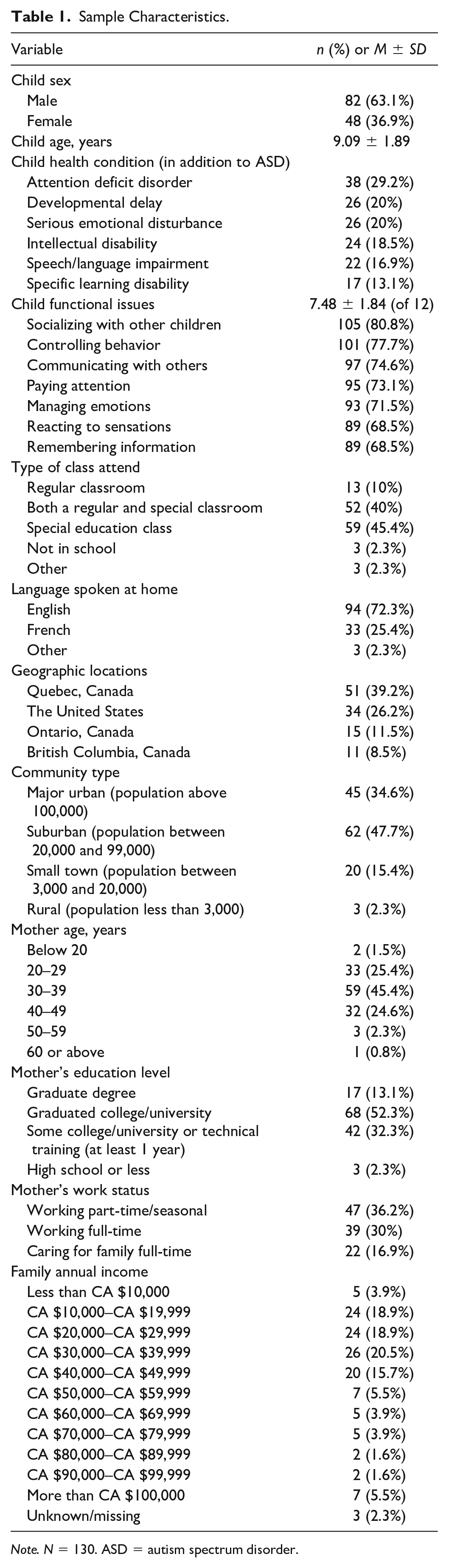
Note. N = 130. ASD = autism spectrum disorder.
Participation Patterns
As described in Table 2, children participated more frequently (t = 15.34, p < .001) and were more involved (t = 2.14, p = .03) in the home setting compared with the community. On average, mothers desired to see change in 71% of the listed activities, similarly in both settings (t = −0.14, p = .89). The specific item scores for each setting were presented in Table 3. With respect to frequency of home activities, all children participated in all the 10 activities at least “few times a month.” Watching TV/videos and personal care were done most often. Regarding involvement, computer/video games and watching TV had the highest mean score. Most mothers wished to see change in personal care (81.5%), followed by doing homework (78.5%) and school preparation (76.2%).
Scores of Participation Scales for Home and Community.
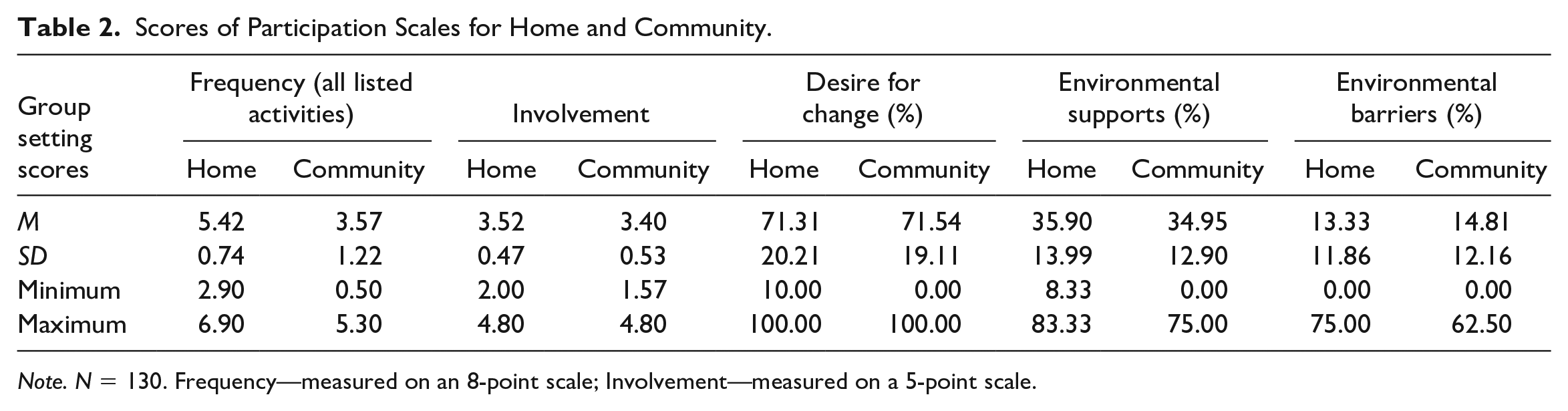
Note. N = 130. Frequency—measured on an 8-point scale; Involvement—measured on a 5-point scale.
Mean Participation Scores of Each Activity for Home and Community.
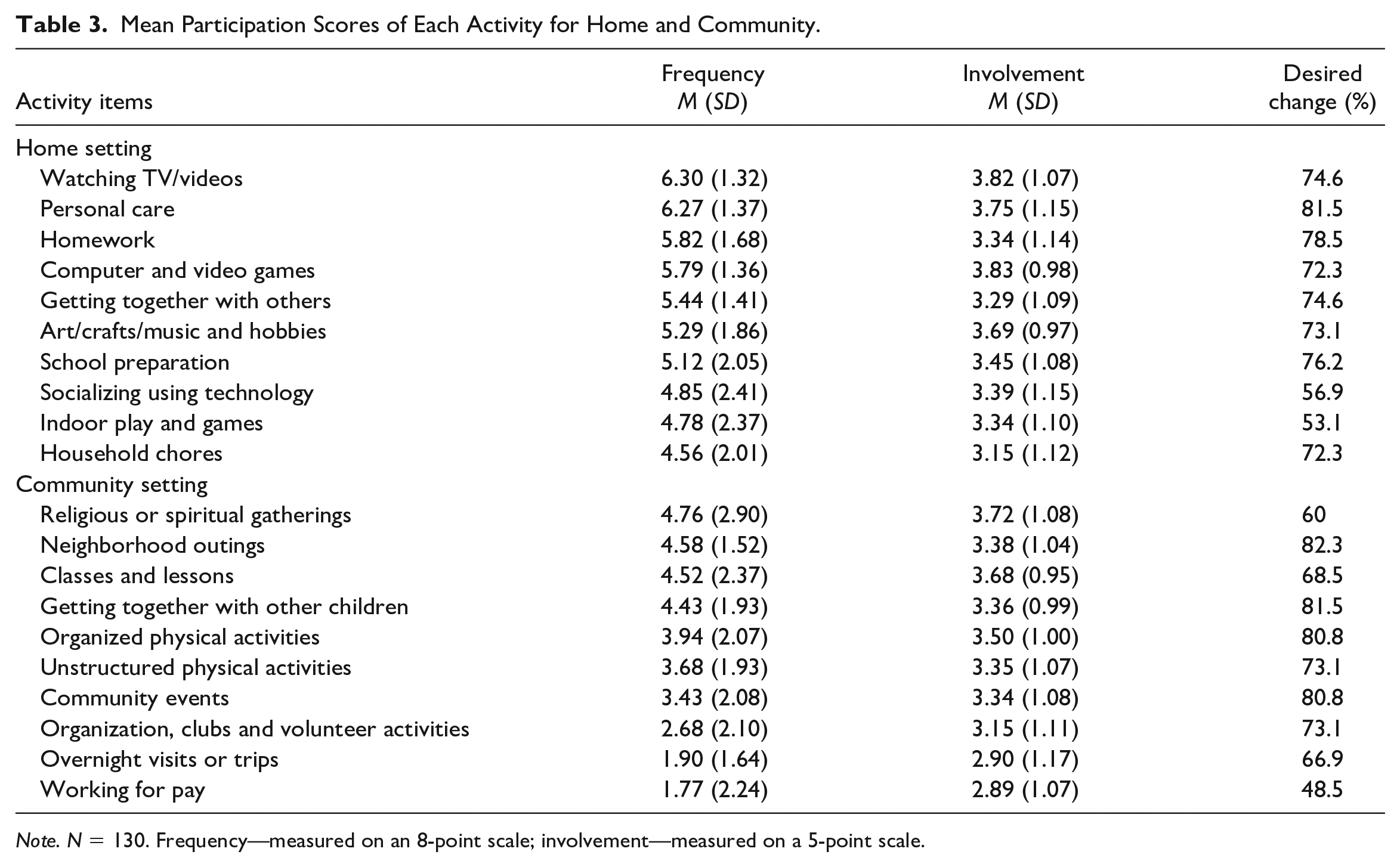
Note. N = 130. Frequency—measured on an 8-point scale; involvement—measured on a 5-point scale.
In the community, frequency levels were lower, with only four of 10 activities being rated as occurring more than “few times a month.” Most common activities included religious or spiritual gatherings and neighborhood outings, whereas least common activities included overnight visits or trips and participating in organizations/groups/clubs. With respect to involvement, “religious or spiritual gathering” and “classes and lessons (not school-sponsored)” had the highest score indicating more than “somewhat involved.” More than 80% of mothers wished to see change in four of 10 listed activities, including neighborhood outings, getting together with other children, community events, and organized physical activities.
Environmental Barriers and Supports
Mothers tended to consider environment items as supports to participation, rather than barriers, in each setting (both p < .001). Descriptively, at home, as shown in Figure 1, having enough resources, including time and money, was the most common support while attitudes/actions of outside caregivers and availability of supplies and information were the most common barriers. In the community, having access to personal transportation was the most common support, whereas availability of equipment or supplies was reported as the most common barrier. No significant differences, based on paired t tests, were found in percentage of supports (p = .532) or barriers (p = .193) between the two settings.
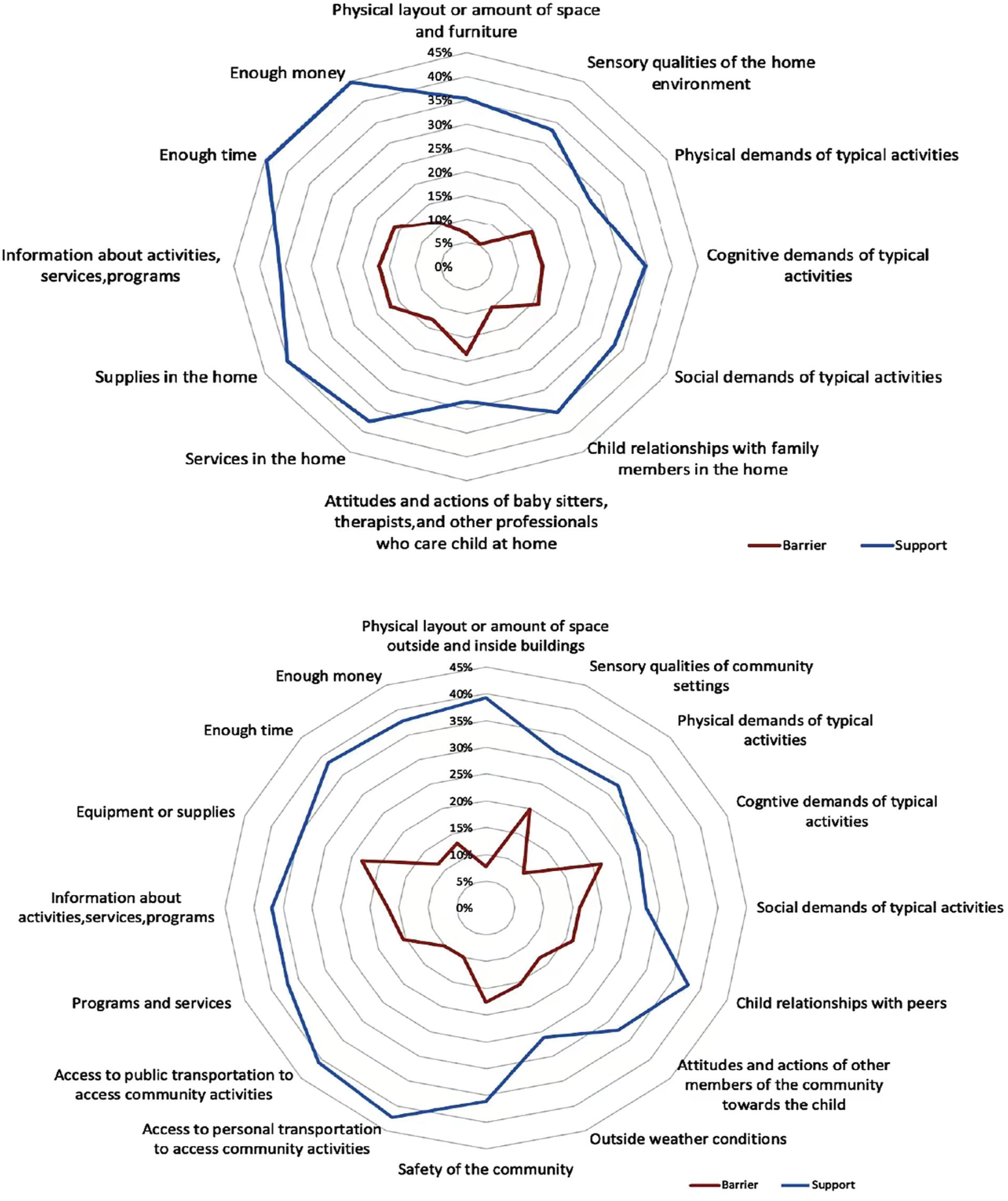
Mean Level of Environment Supports and Barriers in Each of Items in Home and Community.
Models of Participation Outcomes in the Home Setting
At home (Table 4), the outcomes of involvement and desire for change had the highest variance explained (20.9% and 17.4%, respectively) in the final step, and frequency had the lowest level of variance explained (7.6%). Mother’s participation frequency was significantly (and positively) associated with both child participation frequency (β = 0.24) and involvement (β = 0.34), accounting for 5.4% and 10.4% of the unique variances, respectively. The unique contribution of mother’s participation frequency was pronounced in the model explaining involvement levels, and together with child’s age accounted for 21% of the variance. That is, older children of mothers who participated in health-promoting activities tended to be more involved in home-based activities than younger children. Regarding the model explaining desire for change at home, child’s age (β = −0.29), environmental barriers (β = 0.32), and functional issues (β = −0.2) had a significant association with desire for change, accounting for 17.4% of the variance. Younger children, higher number of environmental barriers, and fewer functional issues were associated with greater number of activities in which mothers wished to see change.
Multiple Regression Analyses for Participation Outcomes for Home and Community.
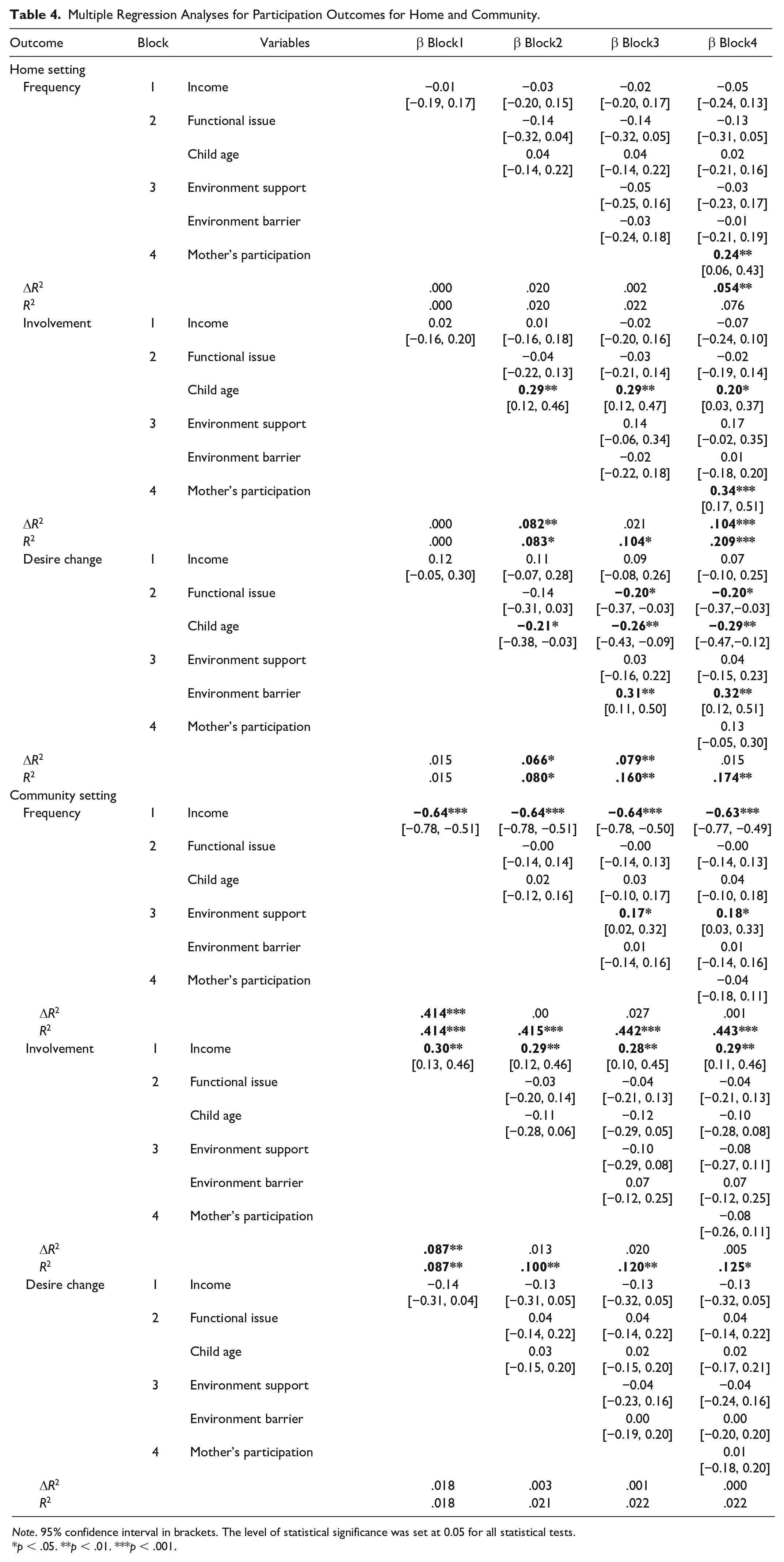
Note. 95% confidence interval in brackets. The level of statistical significance was set at 0.05 for all statistical tests.
p < .05. **p < .01. ***p < .001.
Models of Participation Outcomes in the Community Setting
In the community, participation frequency had the greatest explained variance (44.3%). Family income had a negative association with frequency levels (β = −0.63) and a positive one with involvement (β = 0.29), accounting for 41.4% and 8.7% of their variance, respectively (Table 4). That is, children of families with higher income participated less often in community activities yet were more involved. Income had a more pronounced association in the frequency model and served as the only significant contributor in explaining involvement. Environment supports had a negligible contribution of 2.7% (β = 0.18) on child participation frequency. None of the explanatory factors were associated with desire to change. Mother’s participation frequency was not significantly associated with any of the participation outcomes in the community.
Discussion
Participation Patterns During COVID-19
During COVID-19, school-aged children with autism participated more frequently and were more involved in activities at home than in the community. This concurs with prepandemic research, stating that children with autism prefer home-based activities over community ones (Khalifa et al., 2020). At home, children participated most frequently in watching TV/videos and personal care management. This is consistent with a recent study (Kaya Kara et al., 2021) examining participation of children with ADHD at home during the pandemic, and with prepandemic evidence among children with autism (Simpson et al., 2018). Aligned with previous studies (Egilson et al., 2018; Mattinson et al., 2018), children in our study were more involved in computer/video games and watching TV compared with other home activities.
Nevertheless, the pandemic may have intensified these patterns as families had to stay at home, and additional obstacles to engagement in outdoor community activities existed (Narzisi, 2020). To illustrate, in the community, children most frequently participated in religious or spiritual activities, which is somewhat inconsistent with pre-COVID research, where unstructured physical activities were most frequent (Mattinson et al., 2018; Simpson et al., 2018). A possible explanation includes tighter public health restrictions for outdoor community activities than for religious or spiritual activities that are often employed during crisis and may lead to better mental health outcomes during COVID-19 (Lucchetti et al., 2020).
Mothers wanted to see change in 71% of the total activities in both home and community, implying they were somewhat dissatisfied with their child’s participation, or it was far from being “optimal” or “ideal.” This number is relatively high considering previous studies with same measurement scale (Kaya Kara et al., 2021; Marino et al., 2018) and could be related to disruption in family routine especially as schools changed to remote learning (Hai et al., 2021). In the community, more than 80% of mothers wanted changes in social activities, highlighting a strong need to offer their children more opportunities to be part of community life. The pandemic might have limited opportunities for socializing; hence, creating new informal or unstructured social opportunities for participation in pairs (respecting public health regulations) can be a useful strategy to enhance social participation during COVID-19 (Anaby et al., 2021).
The Effects of Mother’s Participation Frequency Across Models
Findings indicated that mother’s participation frequency had a pronounced association with children’s involvement and had a relatively lower effect on frequency of participation at home. It is plausible that mothers who engage in leisure-based health-promoting activities are aware of the importance of the subjective experience derived from chosen activities. As such, they may encourage their children to also engage in activities they are interested in, which can increase children’s involvement. Findings lend further support to the differences between these two participation dimensions: frequency and involvement, discussed extensively in the literature (Imms et al., 2016). They also highlight the importance of “being in the moment” and fully immersed in an activity especially for those with autism (Askari et al., 2015). Furthermore, when opportunities for community activities are limited (due to COVID-19), extra attention may be given to the quality of the activities (or involvement), making the most of what is possible/available.
As maternal participation is amenable to change, it could be improved through intervention and, therefore, requires further attention in clinical occupational therapy practice. Similarly, a recent study (Bjornstad et al., 2021) highlights the need for interventions that promote healthy behaviors of parent caregivers. The positive association between mother’s own participation and their child’s participation concurs with emerging evidence among preschoolers (Bar et al., 2016; Williams et al., 2019), extending it to school-aged children with autism.
The lack of significant association between mother’s and children’s participation in community-based activities in our study warrants reflection. Barriers to community participation has always been more complex and hard to control in “normal times” (Bedell et al., 2013), and in pandemic times it becomes more complicated. This assumption merits further investigation, combining individual interviews with parents to reflect on their child’s PEM-CY results. Overall, maternal participation appears to be a contributing factor for promoting children’s participation and could be further incorporated in participation-focused studies.
The Contribution of Personal and Environmental Factors Across Models
Income was a significant contributing factor for explaining child participation in the community setting only. Children from higher income families participated less frequently in community activities, but the quality of their participation (involvement) was higher. The negative association between income and participation frequency is not well aligned with previous research (Anaby et al., 2014; Krieger et al., 2018); however, these studies focused on families with relatively high household incomes (CA $80,000–CA $100,000), whereas in our sample almost 60% had an annual family income below CA $39,999. Concurrently, it could simply be that community activities usually done by children of high-income families were unavailable during the pandemic, affecting frequency levels. The positive relation between income and involvement may be explained by potential mediating factors such as parents’ strategies to facilitating child participation. For instance, mothers with more financial resources may have more time and resources to apply strategies to facilitate child social participation (Bedell et al., 2005). Further mixed-methods studies are needed to clarify this, especially during adverse times. Overall, the different magnitude and direction of the effect of income between frequency and involvement further supports that they are two fairly distinct dimensions of participation (Imms et al., 2016). Our study found that child’s age and the number of functional issues explained one participation outcome at home (i.e., desire for change) but had no significant contribution for explaining any participation outcomes of community-based activities. It is plausible that, during the pandemic, functional issues become less profound (especially in the community) as public health regulations mandate participation patterns, rather than child’s personal factors. In addition, findings indicate that environmental factors had limited impacts in both settings. Environment barriers and supports during the pandemic may have played a smaller role than usually seen in previous studies (Anaby et al., 2013; Krieger et al., 2018) given public restrictions. Nevertheless, lack of availability of resources, access to information, and unsupportive attitudes were barriers commonly reported by our mother-participants. Modifying the environment to support participation even in times of crisis is still viable. Anaby et al. (2021) showed that removing environmental barriers using the PREP approach (Pathways and Resources for Engagement and Participation) during COVID-19 improved participation of youth with physical disabilities in leisure activities. This required creative solution–based strategies from the occupational therapists, the parents, and other stakeholders involved. Indeed, providing environment-focused interventions to improve participation by, for instance, connecting families to local advocacy groups and community organizations, educating individuals working with these families, and sharing relevant (and accessible) information with families (about available activities, programs, and resources) can be essential particularly in adverse times.
COVID-19 policies across countries may have influenced our findings during data collection. A post hoc analysis (using t test) comparing the American (26%) and Canadian (74%) subsamples revealed significant differences in participation patterns. Specifically, the U.S.-based children participated more frequently (mean difference = 1.44, p < .01) and in greater diversity (mean difference = 2.6, p < .01) in the community, whereas Canadian children had a higher frequency (mean difference = 0.34, p < .05) and involvement level (mean difference = 0.44, p < .01) at home. Stricter policies on public events, gatherings, and workplace closures in Canada compared with the United States (Razak et al., 2022), may explain this.
This study has some limitations. It employed a cross-sectional, convenience sampling method that did not account for the shifting pandemic-related restrictions practiced within each district and, hence, findings should be interpreted with caution. While the study was conducted mainly in the winter, a seasonal effect may have occurred; however, only 15% of mothers reported that weather conditions served as a barrier (see Figure 1). Autism diagnosis was reported by parents; however, parent-reporting of diagnoses was found a reliable method and a useful epidemiological tool (Daniels et al., 2012). Severity of autism was not assessed. We, however, looked at the overall complexity of child’s functional abilities by gathering information on the number of functional issues. More rigorous assessments pertaining specifically to children with autism, such as the Autism Classification System of Functioning: Social communication (ACSF:SC; Di Rezze et al., 2016), are recommended for future studies. Finally, participation patterns of fathers or other main caregivers were not considered to ensure feasibility and alleviate measurement burden; further larger studies are needed to understand the effect of participation frequency and involvement of both parents/caregivers on child’s participation while considering other caregiving responsibilities.
Conclusion
This study is one of the first to examine participation patterns of school-aged children with autism during COVID-19. Findings highlight the positive impact of mother’s own participation (in leisure-oriented health-promoting occupations) on child participation, especially in the home setting. If further research demonstrates a causal link, such knowledge can redirect clinical attention in occupation therapy (among other health care professionals) toward the development of interventions aimed at improving parental participation with the purpose of facilitating engagement for the entire family unit.
Supplemental Material
sj-docx-1-otj-10.1177_15394492231164939 – Supplemental material for Participation of Children With Autism During COVID-19: The Role of Maternal Participation
Supplemental material, sj-docx-1-otj-10.1177_15394492231164939 for Participation of Children With Autism During COVID-19: The Role of Maternal Participation by Ziru Wang, Anat Golos, Jonathan A. Weiss and Dana Anaby in OTJR: Occupation, Participation and Health
Footnotes
Acknowledgements
We would like to thank Taryn Perelmiter from Summit School, Mushirah Hossenbaccus, and Andreanne Guindon from Lethbridge-Layton-Mackay Rehabilitation Centre, who assisted in recruitment. Thanks are also extended to Pranamika Khayargoli who assisted in editing the manuscript and proofread it.
Author Contributions
Z.W. collected and co-analyzed the data, designed the figures, co-interpreted the results, and drafted the manuscript. D.A. conceived the study design, validated the data analysis, and critically revised the manuscript. J.A.W. consulted the team on analysis and statistics and reviewed the manuscript critically. A.G. reviewed the manuscript critically.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author (D.A.). The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Ethics Approval Statement
Ethical approval has been obtained from both McGill University Research Ethics Board (A06B2614A) and CIUSSS Centre Ouest de l'île de Montréal (the Integrated Health and Social Services University Network for West-Central Montreal) (2021-2663).
Patient Consent Statement
Formal consent was first introduced and then signed electronically using the online platform LimeSurvey, by each eligible participant before starting the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.