
Abstract
Poststroke anxiety and depressive symptoms (P-SADS) affect one in three people and are associated with decreased participation in activities of daily living. This study sought to characterize occupational therapy (OT) P-SADS care practices and identify factors influencing P-SADS care provision in one U.S. inpatient rehabilitation (IRF) facility. An explanatory sequential mixed-methods study design was used by gathering data from electronic health records (from January 1, 2019 to December 31, 2019) as well as semi-structured interviews with OT practitioners in the IRF. No objective P-SADS screens were documented nor were any P-SADS-focused goals written. Minimal evidence-based P-SADS interventions were identified. Practitioners reported multi-level barriers to OT P-SADS care including limited time, pressure to prioritize physical recovery, and inadequate resources to guide practice. OT practitioner P-SADS care was inconsistent with established evidence-based practice. This research identifies gaps in comprehensive stroke recovery and informs implementation efforts to support evidence-based P-SADS care in IRFs.
Introduction
Mental health changes after stroke are common and can present as poststroke anxiety and depressive symptoms (P-SADS; Virani et al., 2020). The one in three stroke survivors who experience P-SADS have significantly worse functional independence, neuromotor recovery, and quality of life compared with survivors without P-SADS (Mitchell et al., 2017; Towfighi et al., 2017; Virani et al., 2020). Stroke survivors with P-SADS are also over three times more likely to die after stroke (Robinson & Jorge, 2016). Stroke survivors commonly discharge from the acute hospital to an inpatient rehabilitation facility (IRF) for continued multidisciplinary intensive rehabilitation (American Heart Association/American Stroke Association [AHA/ASA], 2016; Centers for Medicare & Medicaid Services [CMS], 2021a; Hong et al., 2018). Inpatient rehabilitation is often the most time- and cost-intensive therapy setting, as all patients in IRFs are required to receive 3 hr of therapy per day, 5 days per week, from physical therapy, speech therapy, and/or occupational therapy (OT) (CMS, 2021a).
OT practitioners facilitate functional recovery through occupational performance and participation in activities of daily living (ADL; “Occupational Therapy Practice Framework,” 2020). OT practitioners have expertise in identifying and reducing barriers to independence and meaningful participation in ADLs, and OT practitioners are uniquely qualified to address mental and physical effects of stroke (“Occupational Therapy Practice Framework,” 2020). In addition, practitioners have expertise in building habits, routines, and positive health behaviors that support mental health and functional participation (Burson et al., 2017). To address the negative influence of adverse mental health symptoms on functioning, OT practitioners may use a combination of compensatory and restorative approaches to support meaningful and safe participation in client-valued activities (“Occupational Therapy Practice Framework,” 2020).
While all members of the IRF multidisciplinary team seek to support patient mental health, significant challenges exist in the treatment of P-SADS during post-acute recovery. Anti-depressant and anti-anxiety medications often require 6 to 8 weeks to take effect, which may potentially hinder the effectiveness of rehabilitative therapy delivered in post-acute recovery (Virani et al., 2020). In addition, talk-based studies, largely conducted among rehabilitation psychology, demonstrate minimal effects on functional recovery (Towfighi et al., 2017). Stroke survivors have also reported dissatisfaction over current standards of mental health care, including a perceived lack of patient-centered mental health care and de-prioritization of mental health (Simpson et al., 2018).
Research indicates that a combination of screening for P-SADS and collaborative care interventions in the management of mental health can improve mental illness symptoms and quality of life (Towfighi et al., 2017). OT practitioners play an important role in addressing mental health and supporting collaborative care, however, there are currently no studies examining OT evaluation and treatment practices for P-SADS in U.S.-based care facilities, including the IRF setting. U.K.-based research found varying adherence (40-83%) for P-SADS screening protocols among OT practitioners (Kneebone et al., 2012, 2013; Morris et al., 2012). Without examination of OT evaluation practices, it remains unknown if or how P-SADS are being evaluated in physical IRF settings and the associated functional implications for OT practitioners.
A review by Hildebrand (2015) is currently the only evidence review available examining OT interventions for addressing P-SADS. The review identified behavior modification and behavior change counseling, including motivational interviewing and problem-solving therapy to be effective interventions for addressing P-SADS (Hildebrand, 2015). These review recommendations are also supported by P-SADS treatment guidelines from the AHA/ASA (2016). While the article by Hildebrand (2015) is the only review to guide P-SADS practice, individual studies provide insight to how OT practitioners apply the efficacious treatment strategies identified in the Hildebrand (2015) review. OT practitioners apply motivational interviewing through the identification of barriers to participation and support patients in self-setting goals (Cheng et al., 2015; Oyake et al., 2020). OT clinicians also use problem-solving therapy to provide structure and support in approaching and trialing problem-solving and coping strategies (Visser et al., 2016).
While some research exists regarding recommended strategies for OT P-SADS care, there is minimal documentation of how OT practitioners address P-SADS in IRFs. Given that evidence-based care is not consistently integrated into practice, it is critical that practice patterns are identified and described (Juckett et al., 2020). This work also answers the call for further research into OT practices for psychosocial participation among stroke survivors (Skidmore & Shih, 2022). Therefore, this study sought to: (a) characterize how OT practitioners address P-SADS and; and (b) elucidate factors that influence OT P-SADS care provision at a U.S. academic medical center IRF.
Method
Study Design
An explanatory sequential mixed-methods design was used to integrate electronic health record (EHR) data with semi-structured interviews among OT practitioners at a U.S. academic medical center IRF. This research design allows for EHR analysis to inform the creation of the semi-structured interview guide, as well as to characterize and explain OT practice for addressing P-SADS in the physical IRF setting (Fetters et al., 2013). Figure 1 is a schematic of the study design.
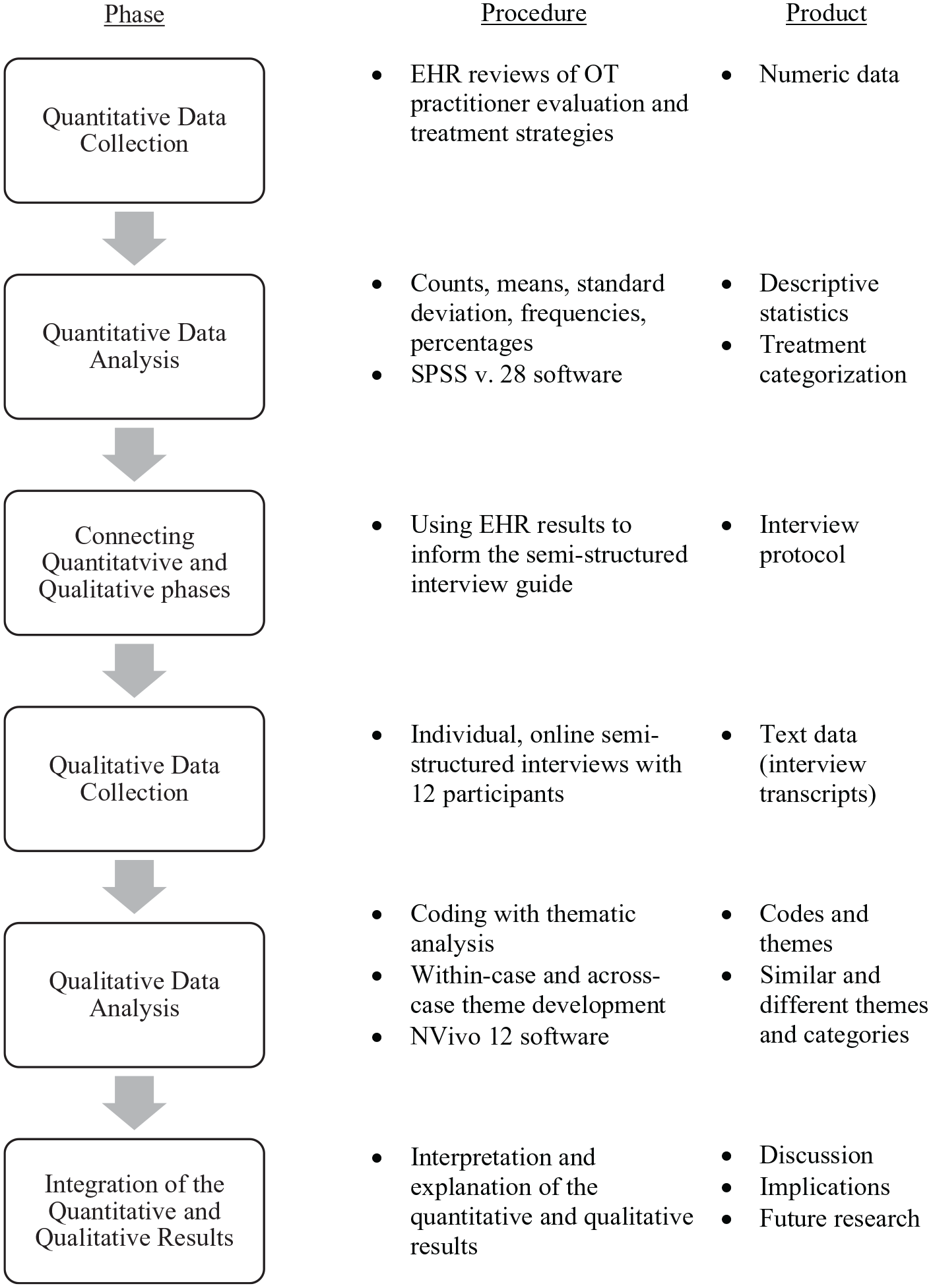
Schematic Illustrating the Study Design.
Participants
Multidisciplinary EHR documentation was reviewed among stroke survivors admitted to the IRF between January 1, 2019 and December 31, 2019. The sample of stroke survivors included patients who were: (a) age ≥35 years; (b) stroke as the sole admission diagnosis; (c) documented P-SADS during the IRF stay; and (d) no active psychosis documented during the IRF stay. Patients aged ≥35 years were chosen as being representative of the larger population of stroke survivors, to reflect that this age group shares 99% of the stroke disease burden (Yang et al., 2017). Patients, who exhibited P-SADS during the IRF stay, were established through interdisciplinary team notes throughout the patient’s stay, including notes from: rehabilitation psychology, physical medicine and rehabilitation medicine, social work, case management, spiritual care services, speech therapy, physical therapy, nursing, and recreational therapy. The 1-year documentation review period was chosen to assess care that was reflective of typical practice prior to the COVID-19 pandemic and to account for seasonal fluctuations in stroke admission, according to Agency for Healthcare Research and Quality guidance (Agency for Healthcare Research and Quality, 2018).
For the semi-structured interviews with OT practitioners, potential participants were recruited via email listservs and through partnership with the OT clinical team lead at the IRF. All state licensed OT practitioners employed at the IRF, who treated stroke survivors at least one time per week, were considered eligible for participation in the interviews.
Procedures
EHR data were extracted manually from OT practitioner evaluation, daily treatment, progress, and discharge documentation. Two trained, independent reviewers completed health record analyses through: (a) counts of the number of P-SADS screens performed by an OT practitioner; (b) goals written by an occupational therapist to target P-SADS; (c) referrals documented by OT practitioners to another IRF provider to address P-SADS; and (d) a directed content analysis of narrative treatment notes where OT practitioners documented addressing P-SADS during a treatment session. The directed content analysis of the treatment notes involved mapping documented treatment strategies to the Hildebrand (2015) evidence review, which analyzed OT interventions for emotional changes after stroke. The review categorized the available evidence into six categories, including: exercise- or movement-based interventions, stroke education only interventions, behavioral therapy only interventions (including any psychotherapeutic framework), education and behavioral interventions, care support and coordination interventions, and community-based interventions. Reviewer training involved weekly meetings throughout data analyses, familiarization with the statistical software and navigating the EHR, defining variables for extraction, and pilot testing all phases of data collection on 10% of cases, prior to full data extraction.
For the semi-structured interviews, the OT clinical team lead and study team member served as a point of contact for scheduling time for participants to complete online interviews during the workday in a private location. Potential participants were individually contacted by the study team via e-mail, with instructions to reply if interested in participation. Consenting participants then completed online semi-structured interviews via Zoom in December 2021-January 2022. The hour-long interview assessed perceptions of: (a) OT P-SADS care provision, (b) barriers and facilitators to addressing P-SADS, and (c) the acceptability and utility of OT addressing P-SADS in the IRF setting. Participants also completed a brief, online demographic and clinical experience survey, including age, gender, race, ethnicity, years of practice, and years of practice in stroke rehabilitation. The semi-structured interview guide was iteratively designed and informed by literature reviews, the EHR analyses completed on OT practitioner P-SADS documentation, and with clinician input. In addition, the semi-structured interview guide was tested on an OT practitioner with IRF experience prior to data collection.
Data Analyses
Qualitative analyses in the study used thematic analysis with an essentialist perspective (Braun & Clarke, 2006). Thematic coding was used to identify patterns of emergent and recurring themes, reported by three or more individual participants (Braun & Clarke, 2006). Theme identification included a combination of inductive and deductive methods (Kiger & Varpio, 2020; Vaismoradi et al., 2014). Inductive theme identification included content analysis of interview text to determine meaning through participant words and sentence structures (Braun & Clarke, 2006; Kiger & Varpio, 2020). Deductive theme identification involved the categorization of barrier and facilitator themes according to the National Academy of Medicine’s framework at the environment (i.e., regulator, payer level), health care organization (i.e., the health care facility and structure), care team (i.e., frontline providers), and patient levels (Reid et al., 2005).
Descriptive analyses were conducted with SPSS v. 28, and NVivo 12 was used for the directed content and semi-structured interview analyses. The qualitative analysis methods used in this study followed Kiger and Varpio’s (2020) guide for thematic analysis of qualitative data, adapted from Braun and Clarke (2006). The semi-structured interviews were audio-video recorded and transcribed verbatim. Two independent coders reviewed audio transcripts and developed a draft codebook. The codebook was then tested on an interview not yet analyzed. Discrepancies were resolved through consensus during weekly meetings. Twelve OT practitioners were available for interview participation, indicating sufficient availability of participants a priori for data saturation, which was defined as no new emerging themes in the data analyses (Hagaman & Wutich, 2017). Interrater reliability was calculated for the directed content evidence categories and for the semi-structured interview analyses. Rater agreement across all instances of coding was ≥0.90, indicating excellent agreement (McHugh, 2012).
Results
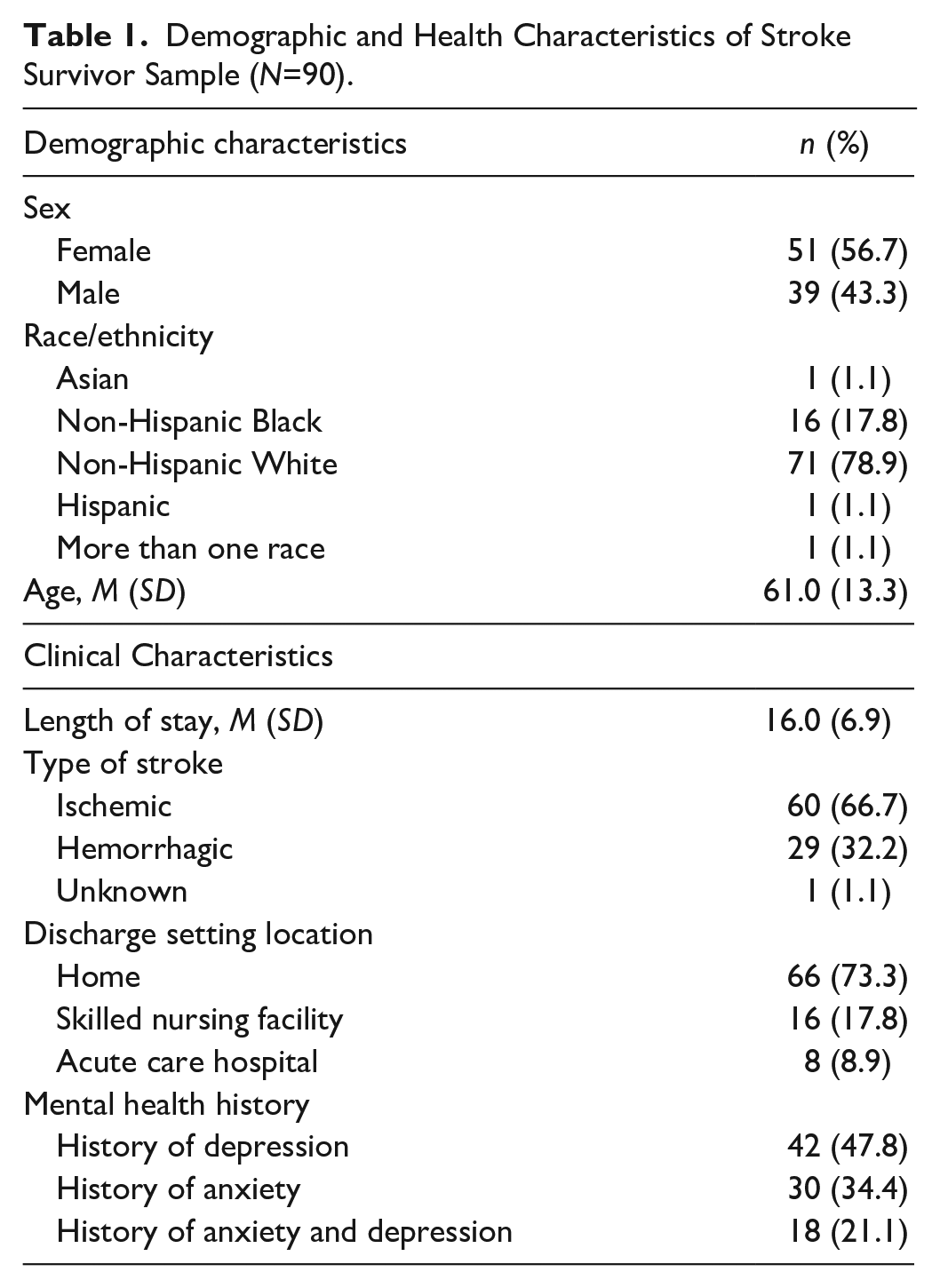
Of the 213 stroke survivors admitted to the IRF during the review period, 90 (42%) patients met inclusion criteria. The majority of stroke survivors (M age = 61.0±13.3 years) were non-Hispanic White (78.9%) and had a previous history of anxiety (34.4%), depression (47.8%), or both (21.1%). Table 1 includes a summary of stroke survivor demographic and clinical characteristics.
Demographic and Health Characteristics of Stroke Survivor Sample (N=90).
Evaluation and Assessment
OT practitioners (N = 23) did not document any objective P-SADS screens, nor were any goals written to target reduced P-SADS, despite the fact that P-SADS were identified as a barrier to performance in 18% of patients in weekly progress notes. OT practitioners documented ADL-focused goals in all patients (e.g., independence with dressing). On evaluation, OT practitioners documented P-SADS observations through subjective assessment in 11 (12.2%) patients. Subjective P-SADS assessments included documentation regarding patient’s body language (e.g., flat affect, poor eye contact) or patient verbal disclosure through self-report of P-SADS. Two referrals were documented by OT practitioners in the narrative daily treatment notes (one referral was made to rehabilitation psychology and the attending physiatrist and another referral was made to rehabilitation psychology only).
Treatment
Sixty patients (67%) had narrative notes explicitly documenting P-SADS treatment by OT practitioners that were used for the directed content analyses. Thus, OT did not document any instances of addressing anxiety or depressive symptoms in the EHR among 30 (33%) of the 90 stroke survivors with P-SADS during the 2019 review period. OT practitioners frequently used supportive treatments, documented in 46 (77%) patients. Supportive treatments that were repeatedly documented by therapists included empathetic listening and therapeutic use of self. For the latter, OT practitioners used their own traits and experiences to build rapport with patients. Of the 60 patients that had narrative notes documenting P-SADS, OT practitioners reported observing P-SADS in 22 (36.7%), patients but did not document any remediation strategies. Interventions documented by OT practitioners to address P-SADS included all six categories from the Hildebrand (2015) review and Table 2 includes examples of interventions documented in this study, mapped to the review categories.
Interventions Documented Mapped to Hildebrand (2015) Evidence Categories (N = 60).
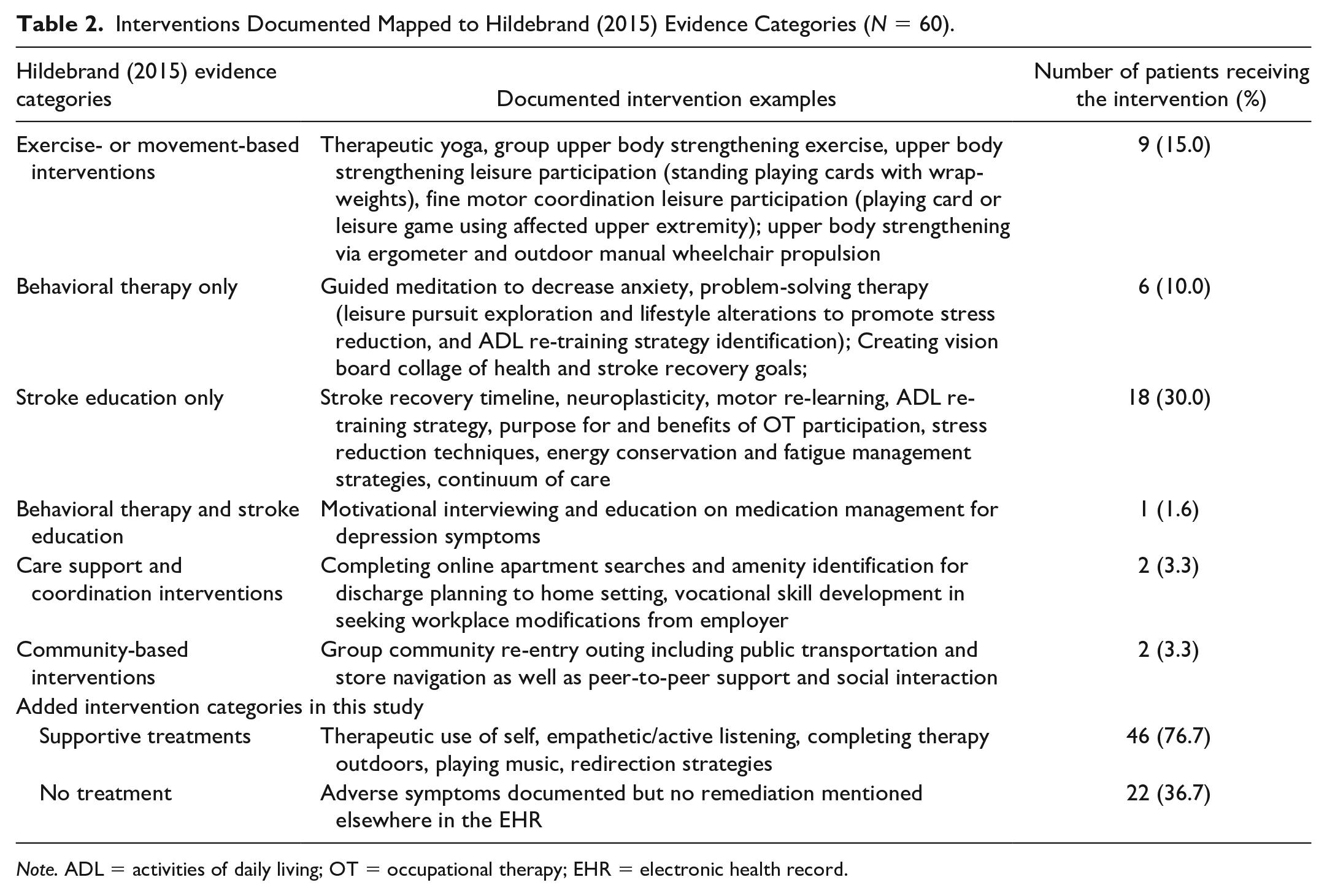
Note. ADL = activities of daily living; OT = occupational therapy; EHR = electronic health record.
Semi-Structured Interviews
OT practitioner participants in the semi-structured interviews were all occupational therapists, female, non-Hispanic White, and had, on average, been practicing for ≥5 years in the IRF setting. Table 3 is a summary of OT participant demographic and clinical experience characteristics.
OT Participant Demographic and Clinical Experience Characteristics (N = 11).
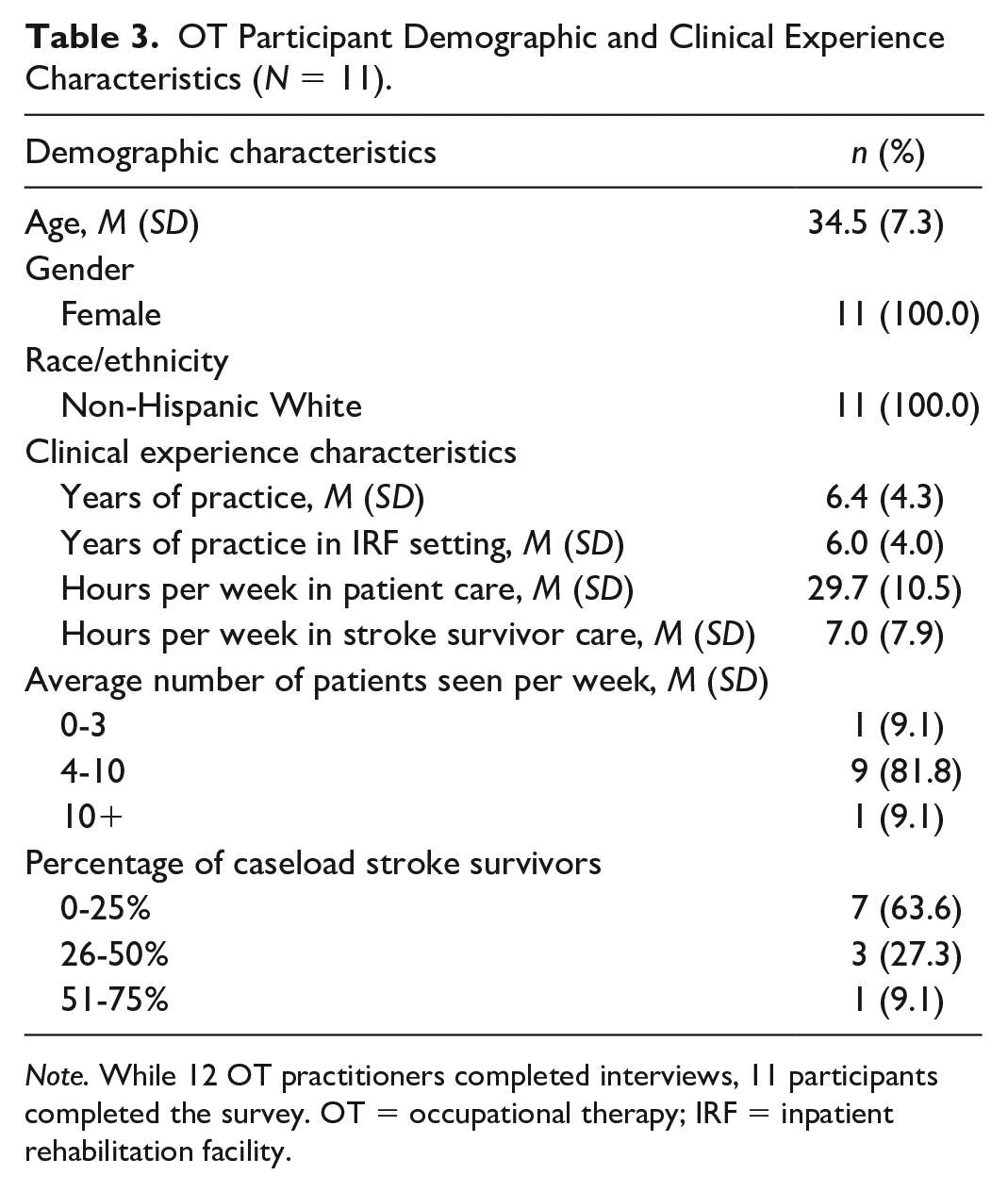
Note. While 12 OT practitioners completed interviews, 11 participants completed the survey. OT = occupational therapy; IRF = inpatient rehabilitation facility.
Table 4 is a summary of common themes and illustrative quotes identified in the semi-structured interviews.
Summary of Common Themes and Illustrative Quotes.
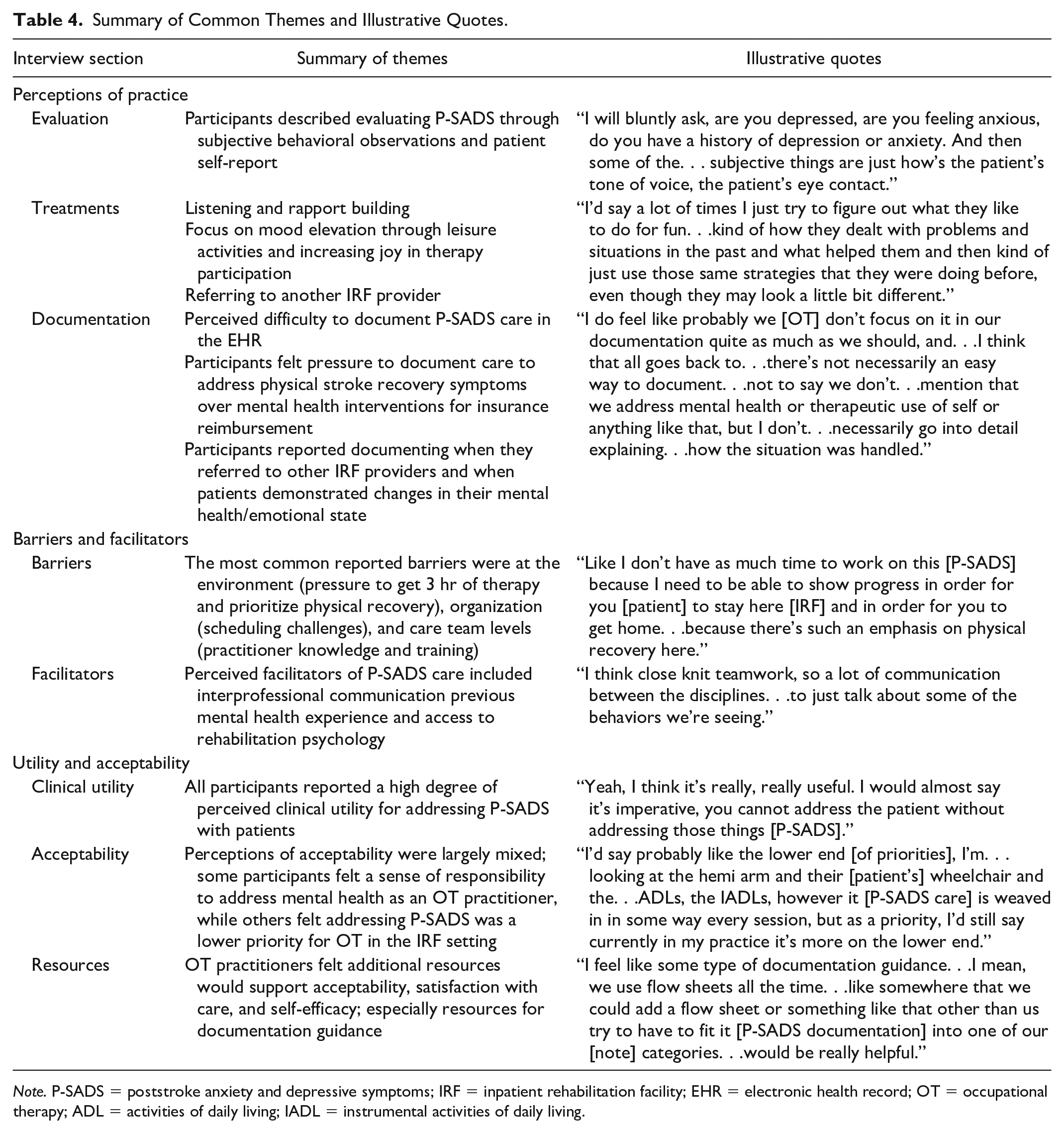
Note. P-SADS = poststroke anxiety and depressive symptoms; IRF = inpatient rehabilitation facility; EHR = electronic health record; OT = occupational therapy; ADL = activities of daily living; IADL = instrumental activities of daily living.
Perceptions of P-SADS Practice
OT practitioners described a highly client-centered practice, focused on using supportive techniques (e.g., therapeutic use of self, empathetic and active listening) for establishing trust and rapport with patients. A participant stated: I really try to get to know my patients pretty well and ask a lot of questions about their family and you know, their interests and what they like to do. . . so I think that helps create that rapport that is required and just the trust, so that they. . .feel comfortable.
Furthermore, connecting with patients on client-centered occupations that were perceived to elevate mood was also an emphasis in P-SADS treatment strategies (e.g., imbedding a valued leisure activity into strength/movement-based treatments or playing music during therapy). One participant stated, “If they’re [the patient] big card player[s], we have all of that here that we can stand, add wrap weights. . .to engage in their strengthening, endurance, standing tolerance goals, while doing something fun.”
Perceived Barriers and Facilitators
The most common barriers reported by participants to addressing P-SADS were at the environment level (reported by nine [75%] participants), organization level (reported by six [50%] participants), or the care team level (reported by five [42%] participants). OT practitioners reported pressure from insurance oversight to prioritize physical recovery over mental recovery of patients. Participants felt that they would like to be able to prioritize mental health more, but limited length of stay and competing priorities (i.e., patient safety, ADL and instrumental ADL completion, cognition, etc.) made balancing all areas within the OT scope of practice feel, at times, overwhelming. One participant stated: Our [OT’s] whole-ism is like, you know, a double edged sword. It’s like really cool, but it’s also like. . .there’s no way I can do all this and be good at all of it and yeah sometimes I’m like what the heck do I address first?
Participants reported their lack of training in mental health as a barrier to implementing P-SADS care, as they felt there were limited resources specific to OT perspectives for treating stroke survivor mental health. One participant stated, “We need more [resources]. I mean, we need any.”
Participants reported facilitators of addressing P-SADS most commonly at the care team level, reported by eight (67%) participants. In addition, participants felt good team communication and having access to rehabilitation psychology were helpful in addressing P-SADS. Participants also cited co-treating with rehabilitation psychologists in instances where patient participation was significantly affected by P-SADS.
Perceived Utility and Acceptability for Addressing P-SADS
All participants reported high clinical utility for addressing P-SADS in IRFs. Participants reported appreciating the inter-connectedness of how adverse mental health symptoms can interfere with therapy participation, readiness to receive therapeutic education and training, and motivation to participate in tasks. Overall, participants indicated fair acceptability and comfort with writing goals to target reduced P-SADS as well as implementing mental health interventions for P-SADS, but felt additional training and documentation resources would be beneficial to increase self-efficacy. One participant stated, “I think more like continuing ed [education] and more people talking about it [mental health] openly would be super helpful.”
Discussion
This study sought to characterize OT P-SADS care and identify factors that influence P-SADS care delivery in the IRF setting. Findings suggest that improvement in OT practitioner P-SADS evaluation and treatment approaches are warranted, as clinicians did not follow recommended evidence-based guidelines for addressing P-SADS (AHA/ASA, 2016; Hildebrand, 2015; Kneebone et al., 2012). No objective P-SADS screens were identified in the EHR review, and no P-SADS goals were written by any provider in the current study. Integration of EHR results with interview findings also corroborate subjective P-SADS evaluation and assessment practices. This is troubling, as the AHA/ASA (2016) guidelines recommend P-SADS screening for all stroke survivors with objective, validated assessments. In addition, P-SADS screening with validated assessments has been associated with improved health outcomes for stroke survivors (Towfighi et al., 2017).
During the 2019 EHR review period in this study, no guideline enforcement existed in the United States for P-SADS screening during inpatient rehabilitation from CMS (CMS, 2021b). The IRF where this research was conducted followed CMS requirements for OT to assess Functional Independence Measure and Section GG scores for eating, grooming, upper body dressing, lower body dressing, toileting, bathing, and problem-solving. Beginning on October 1, 2020, CMS required depressive symptom screening in IRFs through the Patient Health Questionnaire-2 to 9 via section D of the Inpatient Rehabilitation Facility Patient Assessment Instrument (CMS, 2021b). There is currently no guideline enforcement for anxiety symptom screening or guidance for goal writing to address P-SADS in U.S. IRFs. In addition, the ADL-focus of the goals identified in the present study likely reflects the current health-care payment system, to prioritize physical ADL-based goals. Guidance for goal writing to target mental health components of functioning is warranted to address barriers to occupational performance and participation. These findings also support the need for policy changes surrounding P-SADS evaluation and goal setting practices in the IRF setting, to encourage P-SADS screening (especially for anxiety symptoms) and assessment by all qualified providers, including OT, and to ensure that comprehensive stroke recovery is supported in IRFs.
OT practitioners documented and reported few evidence-based interventions to address P-SADS (AHA/ASA, 2016; Hildebrand, 2015). Many providers in this study cited therapeutic use of self as an intervention strategy, however, while therapeutic use of self may be a useful tool to facilitate a positive therapist-patient relationship, therapeutic use of self is not defined as an intervention (Burson et al., 2017). Training in therapeutic use of self is provided in OT curricula in accordance with the Accreditation Council for Occupational Therapy Education (ACOTE, 2021), however, there is little research documenting how practitioners use and implement therapeutic use of self in practice. Given the frequent utilization of therapeutic use of self in this study, further research investigating the application of therapeutic use of self in OT mental health care is needed.
Participants in this study also frequently documented and described leisure-based interventions as a treatment to improve mood. A systematic review of leisure therapy for improving functional outcomes found mixed results, with potential promise for increasing short-term mood and quality of life, but fewer documented long-term benefits (Dorstyn et al., 2014). The common use of leisure activities to address P-SADS identified in this study indicates a need for additional research and resources for distinguishing and clarifying interventions versus supportive techniques in evidence-based P-SADS treatment.
This study’s findings corroborate previous literature that OT practitioners report barriers that negatively affect the quality of care they provide to stroke survivors (Juckett et al., 2020; Simpson et al., 2018). Limited time for providers to keep up with current literature as well as pressure for insurance reimbursement to prioritize physical recovery over mental recovery were perceived to negatively affect care delivery and explains the limited evidence-based P-SADS care observed in this study (Juckett et al., 2020; Simpson et al., 2018). These findings point to how practice settings influence evaluation and treatment strategies among OT practitioners, wherein navigating how to addresses mental functioning in the current medical system limits the ability to provide holistic stroke rehabilitation. The lack of P-SADS care observed in the present study may also have been influenced by OT practitioners’ current inability to bill for mental health care services (American Occupational Therapy Association, 2022). Subsequent work investigating the efficacy of OT-delivered mental health interventions that assess mental and physical functioning, in addition to policy support for OT to bill for mental health care services, is needed to support comprehensive stroke recovery.
Discrepancies in the integration of EHR and interview findings in this study centered on the use of rehabilitation psychology by OT practitioners. While participants reported referring patients experiencing P-SADS to rehabilitation psychology, there were only two instances of inter-provider referral documented for the 2019 review period. Furthermore, participants reported that they perceived completing a treatment session with rehabilitation psychology (or co-treating) as facilitative for addressing P-SADS with patients. However, there were no instances of co-treating documented in either OT or rehabilitation psychology treatment notes. The environmental, organizational, and care team-level barriers observed in this study and others reflect fragmented P-SADS care delivery, especially between OT and rehabilitation psychology (Simpson et al., 2018). In addition, these findings suggest that OT practitioners may have verbal referral and treatment decision discussions, but may not formally document these interactions in the EHR. There are currently no studies examining the relationship between OT and rehabilitation psychology in U.S. IRFs, and further investigation of this relationship is needed to better understand and support stroke survivor mental health, especially given the importance of rehabilitation psychology for addressing P-SADS reported by participants in this study.
Internal and external organizational strategies to guide OT P-SADS clinical decision-making are needed to meet the needs of practitioners regarding the perceived utility for OT addressing P-SADS in IRFs, as well as to enhance the mixed perceptions of acceptability for OT P-SADS care. Educational curricula supported by ACOTE, and continuing education opportunities should incorporate evidence-based strategies for addressing P-SADS, as this study’s results suggest that additional training materials and capacity building interventions for OT practitioners could increase self-efficacy and acceptability for addressing P-SADS in IRFs. The lack of setting- and discipline-specific resources and training also explain the limited evidence-based P-SADS care delivery observed in this study and others, across the continuum of care (Pisegna et al., 2022; Simpson et al., 2018). The paucity of resources to guide OT P-SADS care also highlights the need for investigation of P-SADS management in settings with less access to and fewer infrastructure supports for mental health care (e.g., rural settings and skilled nursing facilities) (Hong et al., 2018). Resource allocation and research guided by implementation science theories, models, and frameworks are needed to justify to regulatory entities that addressing P-SADS in IRFs can support physical functional and neuromotor recovery, in addition to mental health, are needed (Murrell et al., 2021; Towfighi et al., 2017).
Limitations
This work was conducted at one academic medical center facility and therefore may not reflect practices at other IRFs, as this setting may have access to greater resources (i.e., rehabilitation psychology) which may have affected the findings. Furthermore, care implemented in practice might not have been documented or accurately captured by OT practitioners in the EHR, and therefore, documented care in the EHR may not reflect what was implemented in practice. In addition, because OT practitioners cannot currently bill directly for mental health interventions, this may make clinicians reluctant to document mental health treatment but rather to incorporate mental health goals into occupational participation or performance goals. Furthermore, the participants included in this study were all licensed occupational therapists, non-Hispanic White females, and had been practicing, on average, for ≥5 years. This limited demographic variability is consistent with trends across the OT field overall, but research incorporating greater representation of perspectives and health-care providers (e.g., OT assistants and rehabilitation psychology) is needed (Taff & Blash, 2017).
Conclusion
Minimal evidence-based OT P-SADS evaluation and treatment in inpatient rehabilitation was documented and described in this study. The limited evidence-based care was explained by multi-level barriers to implementing P-SADS care, including limited time, pressure to prioritize physical recovery, and minimal education and training for addressing P-SADS. This work identified gaps in the quality of mental health care provided to stroke survivors and spotlights opportunities to improve OT services in stroke rehabilitation. Building from this work, collaborative care to promote interdisciplinary mental health care is needed, in addition to OT practitioner resources for addressing P-SADS to facilitate functional participation and comprehensive stroke recovery in the IRF setting.
Supplemental Material
sj-docx-1-otj-10.1177_15394492231151886 – Supplemental material for Occupational Therapy for Poststroke Anxiety and Depressive Symptoms in Inpatient Rehabilitation
Supplemental material, sj-docx-1-otj-10.1177_15394492231151886 for Occupational Therapy for Poststroke Anxiety and Depressive Symptoms in Inpatient Rehabilitation by Janell Pisegna, Rachel Knebel, Lisa Juckett, Amy Darragh, Deborah S. Nichols-Larsen and Jessica L. Krok-Schoen in OTJR: Occupation, Participation and Health
Footnotes
Acknowledgements
The authors would like to thank Jodelle Jones for their support in the completion of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Bonita Kraft Doctoral Occupational Therapy Student Scholarship through the American Occupational Therapy Foundation.
Ethical Approval
This study was approved by The Ohio State University Institutional Review Board (study approval number 2021H0052).
Informed Consent
This study was approved by the institutional review board and informed consent was obtained for all participants.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.