
Abstract
Purpose
To assess the evidence in the current literature, identify the knowledge gaps and propose future standards for the use of pressure indices in peripheral arterial disease (PAD).
Methods
A search of all medical databases was performed to identify studies performed between 01/01/2000 and 31/12/2024, looking at the use of FFR or IFR in the management of PAD. The Newcastle-Ottawa scale was used to assess the quality of the papers. A comparison of the studies was performed using various parameters including; study design, cohort demographics, aim, lesions treated, hyperaemic agent used/pressure indices utilised, FFR endpoint and clinical outcomes.
Results
136 studies were found in initial search. Only studies investigating FFR were identified, none looked at IFR. Following the application of the exclusion criteria, 8 relevant studies with a total of 247 patients were included in the final analyses. No randomised controlled or prospective trials were found. Significant heterogeneity was observed in the methodology and data collection among the included papers. Despite this, the analysis demonstrated initial evidence showing the potential of pressure measurements to revolutionise diagnostic, intra-procedural and prognostic decisions in PAD, akin to the data that already exists in coronary artery disease.
Conclusions
Further standardised research of FFR is needed in peripheral vascular disease to improve objective understanding of physiological parameters pre and post-treatment. To this end, a standardisation tool has been proposed to homogenise and aid future research in drawing more robust conclusions for the use of pressure indices in PAD.
Introduction
Endovascular therapy (EVT) is currently the first-line procedural treatment option for the majority of patients with peripheral vascular disease (PVD). In recent years, while interventional techniques and devices have been developing rapidly, the clinical decision making and patient selection are essentially unchanged. 1
The main parameters integral to diagnosis, patient selection and the prediction of procedural outcomes remain clinical history and imaging investigations; such as duplex ultrasound, computed tomography angiography (CTA), magnetic resonance angiography (MRA), interventional angiography and ankle-pressure index (ABI). However, none of these methods is effective or practical at making an objective assessment of the lesion’s hemodynamic status, pre and post-intervention. Although the decision to intervene should consider the patient’s perceived symptoms as well as the actual impact on quality of life, the technical aspects of the procedures still depend on diagnostic methods that provide information limited to anatomical features, without offering insights into the significance of physiological functions.
Hence, there is a need for robust and accurate guiding measures to assess atherosclerotic lesions, in particular the equivocal ones properly, and to objectively optimise intervention techniques and treatment outcomes. 1
In the management of coronary artery disease, cardiologists routinely use indices derived from invasive intra-arterial pressure measurements to guide decision-making intraoperatively, including whether and how to treat.2,3 These indices are called the fractional flow reserve (FFR) and the instantaneous wave-free ratio (IFR). FFR is defined as the ratio between mean post-stenosis coronary arterial and aortic blood pressures under vasodilator-induced hyperaemic conditions. 2 In the last few decades, it has been used as the gold standard for assessing the functional severity of coronary artery lesions. 4
On the other hand, IFR is defined as the ratio between the mean values of post stenosis coronary arterial and aortic blood pressure during the diastolic wave-free period under non-hyperaemic resting conditions. 5 IFR can be measured without the need for vasodilator administration, and has emerged as an alternative index of stenosis severity.2,6,7
The key value of these pressure-derived indices are in determining whether a lesion is haemodynamically significant and measuring the change following the intervention. These indices can also be performed during the procedure, unlike CTA and ABI, and acted on immediately which makes them a helpful adjunct to angiography and intravascular ultrasound. This would also allow an objective assessment to be made, helping to provide standardised care.
While these methods have been widely researched within in the context of coronary disease, there has been little data related to peripheral vascular disease. Pressure-derived indices may be able to objectively assess the effectiveness of treatments and better guide interventional radiologists and vascular surgeons in treating and managing their PVD patients.
Methods
This study was split into 2 sections: a literature review, followed by an analysis of the relevant studies. The literature search followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.8,9
The aim of this review is: (1) To establish the current knowledge of FFR or IFR during peripheral endovascular revascularisation. (2) To identify any study that combined physiological measurements with other imaging guidance such as IVUS, angiography (2D or 3D) perfusion or any other perfusion measurement tool to assess clinical outcomes. (3) To identify the gaps in knowledge when compared to established practice in coronary arteries and recommend further steps in future research.
For the review design, it was decided to include any paper that looked at the use of FFR or IFR in the management of peripheral arterial disease. The ideal comparison was any modality that was not a pressure measurement, and the outcome was to identify if there was a benefit of using FFR and IFR over all other modalities. All medical databases, including PUBMED, EMBASE, COCHRANE and OVID were searched from 01/01/2000 until 31/12/2023. Another updated search was also conducted to cover the period from September 2023 to 31/12/2024. The search criteria focused on gathering papers looking at FFR or IFR in the management of peripheral vascular disease and were restricted to English manuscripts and only those including human participants in their research.
Papers that did not refer to peripheral vessels, i.e coronary arteries were excluded. Papers with single case reports, letters to the editor and commentaries were also excluded.
The search string was edited for each database to meet their requirements and is seen in Figure 1, the refined of the strategy was based on the vast literature on coronary arteries. Search Strategy
Two researchers (KK, AAR) then independently reviewed all the acquired papers, strictly filtering by applying our inclusion and exclusion criteria. A third member of the team (MS) then went through both sets of data to identify any discrepancies and resolve any differences of opinion. Each relevant paper was then analysed and data was extracted through pre-determined outcome variable seen in Figure 2. Data Collection Points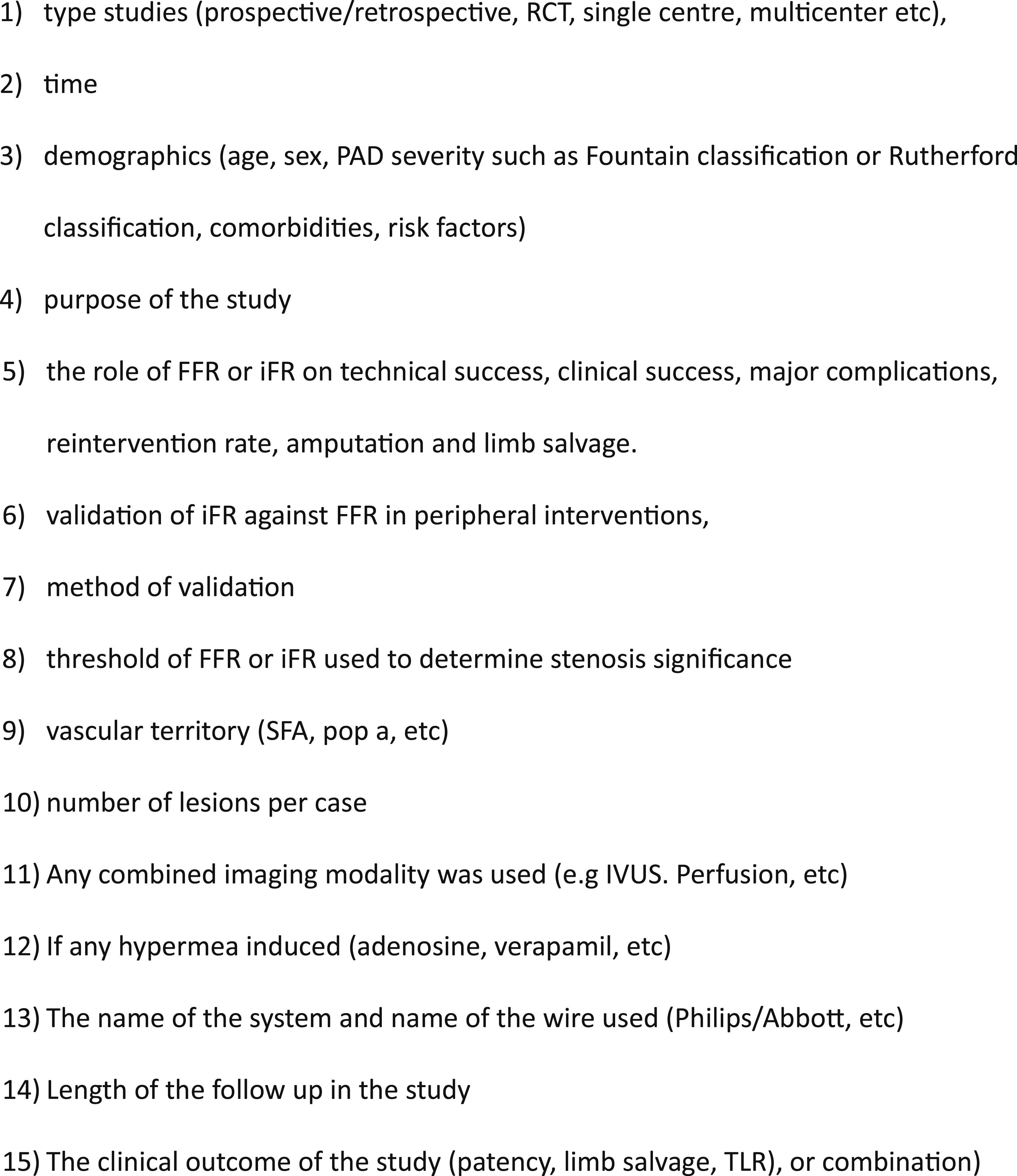
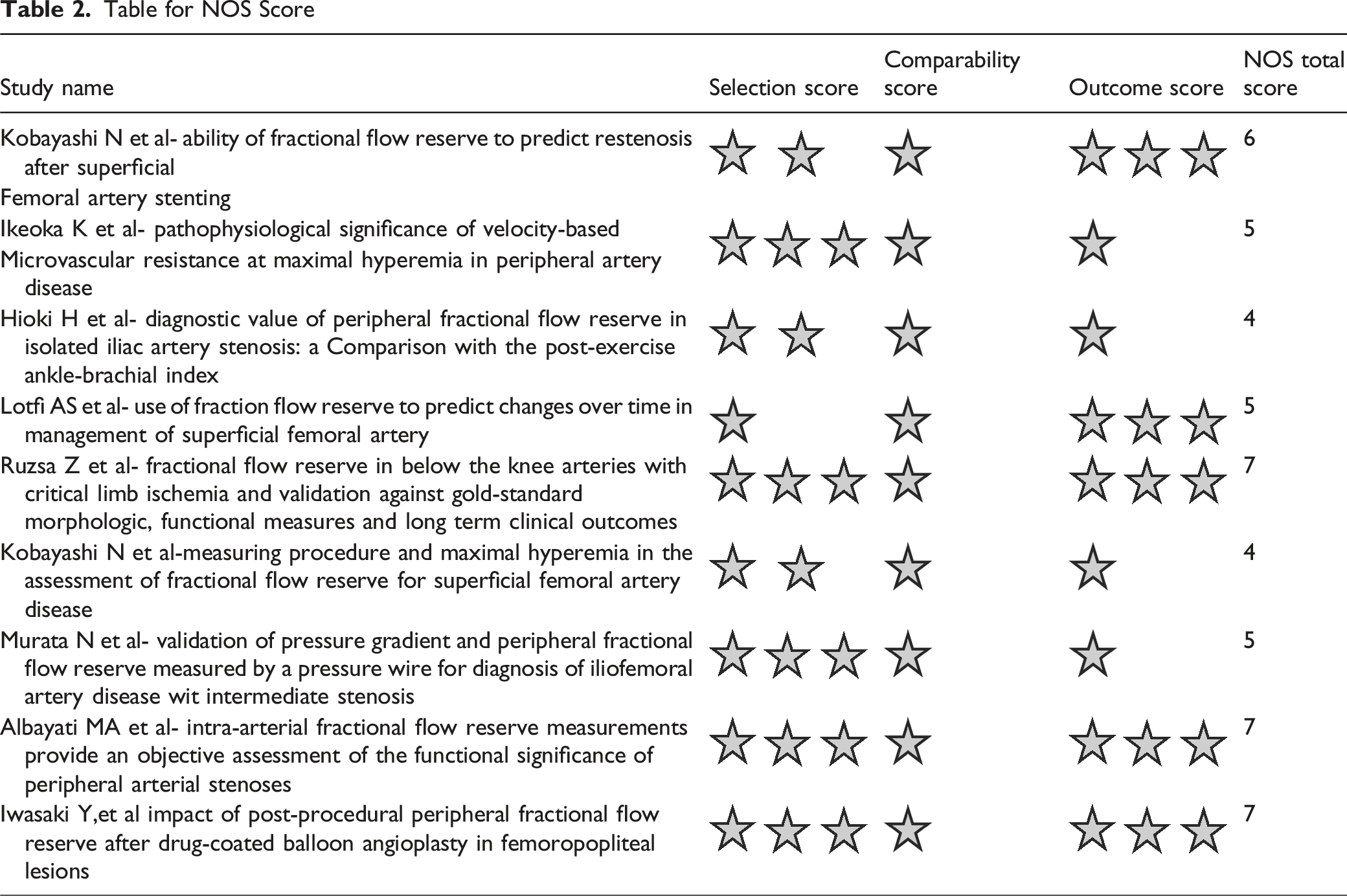
Subsequently, the Newcastle-Ottawa scale (NOS) was used to assess the quality of the papers. The NOS, recommended by the Cochrane Collaboration, contains 8 items, categorized into 3 dimensions: selection, comparability, and outcome or exposure for cohort studies or non-randomised case–control studies. Studies are graded one point each for all items except comparability which has the potential to score up to 2 points, with the maximum possible score being 9. Studies are rated from 0-9, with those studies rating 0-2 (poor quality), 3-5 (fair quality), 6-9 (good/high quality). 10
At this point, it was evident there was very little literature available for effective meta-analysis, and the studies lacked effective standardisation to compare results from their participant cohorts to measured parameters statistically. Instead, a narrative review of their results and findings was performed.
Results
There were 137 studies found in the aforementioned databases following the application of our search criteria. However, once we filtered their titles and abstracts, with the inclusion and exclusion criteria/removed duplications, only 12 studies remained. A further 4 studies were then removed following an extensive full article review, as were conference abstracts or review papers.11-19 Updated search until December 2024 found one more paper of 45 patients
19
. This left a total of 9 relevant studies as seen in Figure 3. All 9 studies were prospective single centre trials. PRISMA Flow Diagram for Screening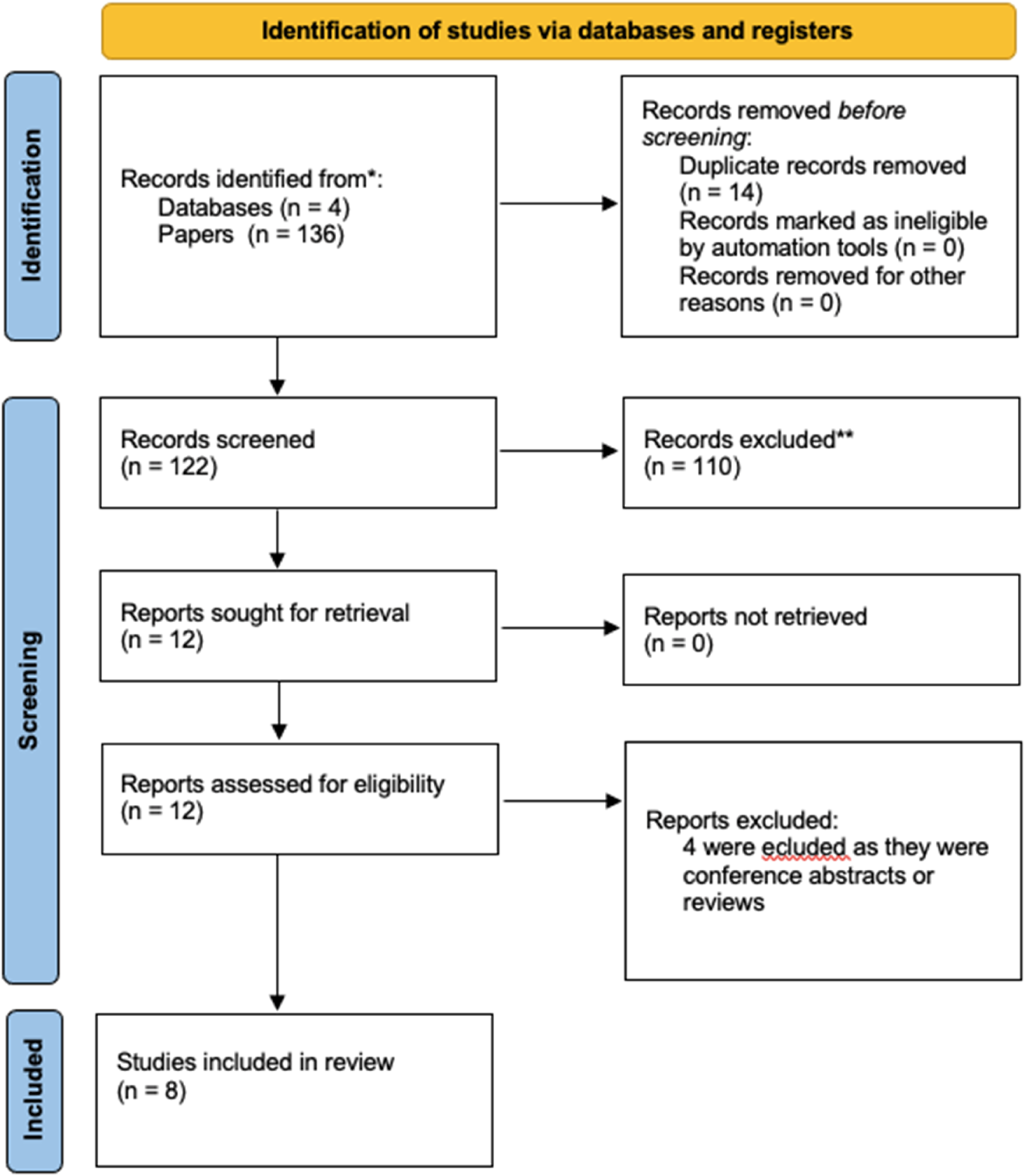
Within these 9 studies, there were 292 patients. There was no overall trend within these studies for demographics, but importantly all of them investigated FFR measurements and none looked at IFR. Different studies included participants with a stenosis at different anatomical locations, with 4 studies assessing superficial femoral artery lesions, 3 studies assessing iliofemoral lesions and one on below-knee lesions.
Comparison of the Relevant Studies
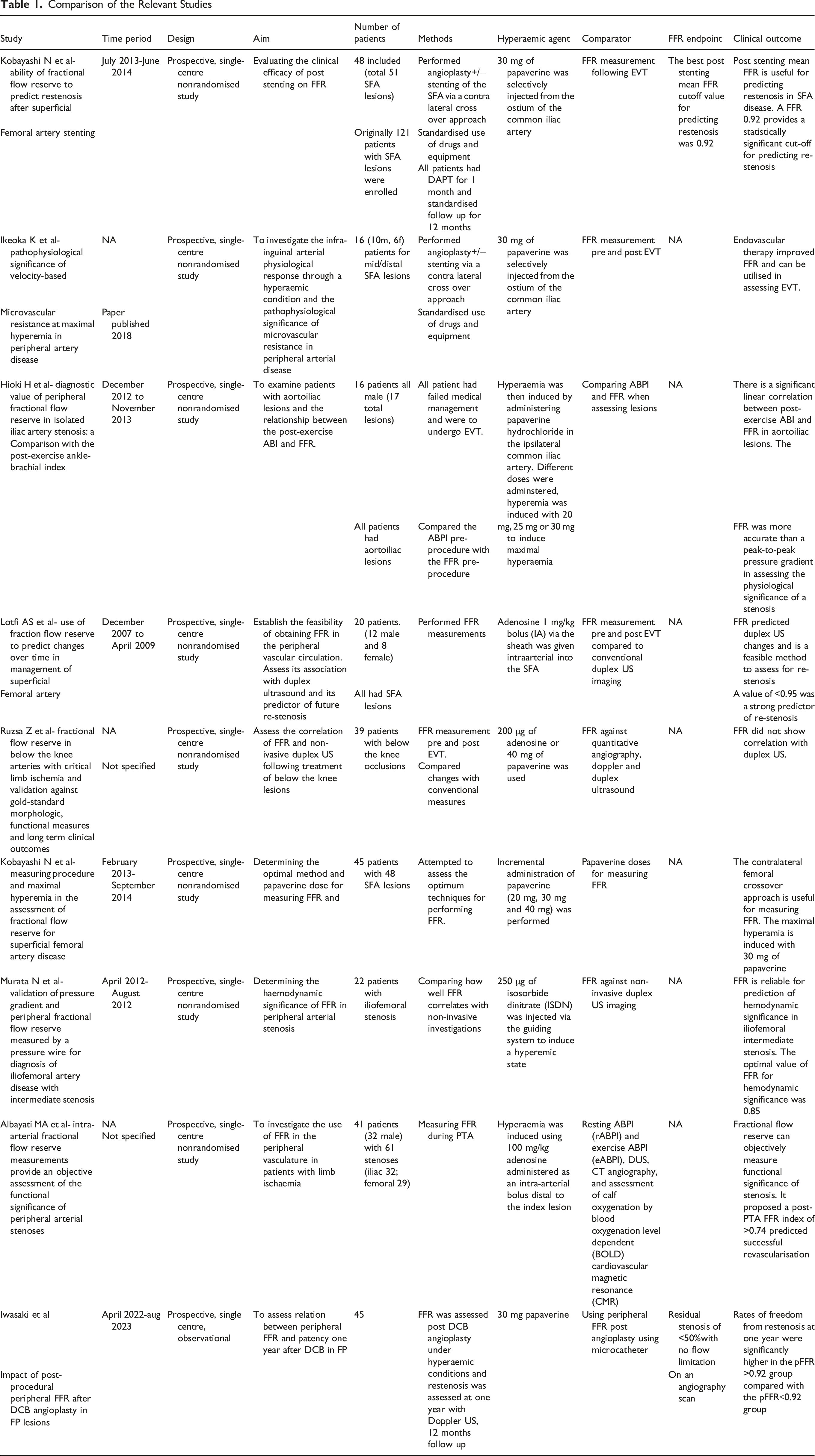
All 9 studies investigated the relation between FFR and clinical outcomes, however a range of different outcomes was used meaning their results are not directly comparable. The outcomes studied for each investigation are summarised in Table 1. All included studies focused on examining the physiology of stenosis and immediate benefits following the intervention. Only 1/8 studies 11 looked at long term outcomes, using the FFR data to help predict re-stenosis after 12 months. The other 8/9 focused on intra and early post-procedural use of FFR. Interestingly, all the papers identified a benefit to utilising FFR in the management of peripheral vascular disease.
The majority of the papers (6/9) utilised the same hyperaemic agent, papaverine, when measuring FFR. Two papers used adenosine and one paper isosorbide dinitrate. There was also variation in the manner FFR was utilised. Some papers (5/9) focused on the change in values following intervention, others compared FFR to another measure of stenosis severity to determine how effective it is as an assessment (3/9), and 1/9 looked at the optimal technique to measure FFR in the peripheral system.
Table for NOS Score
Discussion
The use of pressure-derived indices is well researched in the setting of coronary artery disease, with research demonstrating that FFR guided revascularisation has a 43% reduction in 1 year mortality in cardiac patients, against intervention without FFR. 21 This degree of uptake has not yet occurred in peripheral vascular disease despite the substantial improvements in outcomes seen in interventional cardiology.
This systematic search of the literature found 9 studies investigating the use of FFR in this setting. There were no randomised controlled trials or large prospective single or multicentre series. The 8 studies used different methodologies which precluded direct comparison of their results. However, the available work has demonstrated the potential benefits of FFR in the management of peripheral vascular disease through a range of outcomes. These studies have also suggested FFR values in their cohorts that can be used as a cut-off to assess treatment success and the probability of re-stenosis.
There was only one longitudinal study with a 12 month follow up of 48 patients and a total of 51 lesions. 11 This study indicated that following intervention, the patients that had re-stenosis generally had lower FFR values. The authors proposed that an FFR value of <0.92 post-stenting as an indicator of predicting re-stenosis. This highlights that FFR measurements could probably assess the need for intervention and provide an indication of how effective the treatment has been and risk stratify patients for the likelihood of re-stenosis.
All the studies had no complications from performing FFR measurements, suggesting that this was a safe addition to any already ongoing EVT and that giving a vasodilator, in FFR, does not have any morbidity or mortality. Furthermore, 7 of the 9 studies provided evidence that FFR was capable of identifying lesions and that it improved following treatment as seen in Table 1. Interestingly, 3 of the studies included a small number of patients with multiple lesions and their treatment did not appear to be standardised within each paper and the relevance was not considered.
Four studies suggested FFR cut-off values to predict re-stenosis in the cohorts they examined giving values of 0.92, 11 , 0.95 12 and 0.85. 13 It must be noted that the first 2 studies11,12 had cohorts of patients with SFA lesions whereas the latter study looked at iliofemoral stenosis. 13 This may be one of the confounding factors causing the discrepancy. The patient demographic, cohort size, lesion location, number of lesions, co-morbidities may just be a few factors which could influence FFR value cut-offs for predicting re-stenosis and treatment outcomes. Further research is essential to understand how peripheral vessel pressure gradients respond to these factors and to create standardised figures to assess patients post-treatment. Given the heterogeneity in methodology, equipment used, and endpoints among the included studies, this narrative review refrains from recommending a specific FFR threshold value. However, there is a clear trend across nearly all work in this field, indicating that FFR is likely to play a role in maximising both technical and probably clinical outcomes of PVD interventions.
A recent study of 41 patients with isolated iliac or superficial femoral arteries 14 concluded that FFR can be an objective measure to assess the functional significance of peripheral artery stenosis and proposed that it could be used to influence management decisions for patients at a more personalised level. It was also the only study to isolate patients whose symptoms persisted post treatment and proposed an FFR cut-off of >0.74 for successful revascularisation. The study had only 10 cases whose symptoms persisted, and so further data is needed to confirm this finding. The discrepancy between this suggested cut-off and previous estimates suggests that the relevant FFR level to determine whether revascularisation is appropriate and whether revascularisation has been successful may be different. The latest published single centre series of 45 patients examined the role of peripheral FFR post drug coated angioplasty 21 . The researchers also concluded that an FFR threshold of <0.92 could be a good predictor of restenosis at one year.
The oldest study by Lotfi et al, 12 compared FFR to conventional vascular imaging investigations, duplex ultrasound imaging, in 20 patient with SFA lesions. The study showed that FFR results could be used to predict the changes seen on duplex ultrasound. The doppler-derived peak systolic velocity, which is a known to predict the likelihood of restenosis, directly correlated with FFR. However, this authors suggested that further investigations were required to confidently draw any conclusions given the small sample size and non-randomised design.
The findings from the NOS checklist assessment reaffirmed the poor comparability of the studies and the inconsistencies of the factors examined, highlighting the lack of standard scientific expectation when assessing FFR in peripheral vascular disease. Therefore, future research should adopt a strict framework and design. It should take into account the complexities of PAD and some fundamental differences from coronary disease.
All papers included in this systematic review acknowledged the lack of statistical power. Across all 9 papers the total patient number was 292. This is a relatively small number and given all the limitations that have been discussed, and the variability of the chosen cut-off value for FFR within each study, it is clear that large, well designed studies are required to determine how FFR can be used in practice.
To address the gaps in knowledge, the following frameworks are suggested to guide future research in the field. 1. FFR predictive values should be compared against gold standard methods of diagnosing ischaemia and ideally combined with tissue perfusion assessment. Investigators should include, besides anatomical criteria, the assessment of FFR before and after intervention. 2. Prognostic importance of FFR in terms of limb salvage, tissue perfusion and stenosis recurrence rate should be evaluated in properly powered cohorts with longitudinal follow up of at least 24 to 48 months. These outcomes can be determined in patients without revascularisation or post revascularisation. 3. FFR measurements should account for the number, anatomical locations of lesions, the proximity of tandem lesions and should ideally address the role of inflow stenoses. 4. The practicality and cost effectiveness of implementing physiological studies should be compared to a control group using current practice.
Upon review of the manuscripts, the observed lack of standardisation is presumably attributable to the absence of comprehensive data regarding the utilisation of hyperaemic agents, pressure measurement techniques, and general procedural methods. Each centre has implemented its respective local protocols and preferences. The adoption of the aforementioned framework, in conjunction with multi-centre collaboration and a standardised study protocol, will be essential for conducting more rigorous future research.
The key finding in this review is that there is evidence that pressure indices have the potential to refine diagnostic, intra-procedural and prognostic decisions in peripheral vascular disease. They can give an indication of the haemodynamic burden of a stenosis, demonstrate an objective change pre and post intervention and may also allow interventional radiologists to estimate the likelihood of restenosis. At the very least this will provide invaluable information for when and how aggressively treatment should be offered. This is akin to the data that already exists with respect to coronary artery disease. 2 Similar to most radical changes in routine practice, the barriers to implementing radical changes in intervention practice are expected to be challenging. These hurdles should be addressed through collaboration with industry to smooth out workflow in angiosuite as well as designing pragmatic trials that allow timely recruitment and investigator engagement. The interventional community must be persuaded to use the physiology tools by creating the appropriate evidence and ensuring that no significant cost burden is incurred.
Conclusion
The FFR can potentially identify lesions which need intervention and those that do not, determine how effective an intervention has been and help risk stratify how the follow-up and monitoring plan should be structured. However, current data are limited, and considerably more research is needed before FFR can be used for peripheral vascular disease in routine clinical practice. Further work should consider the FFR and its correlation with other measures of ischaemia and with clinical outcomes and the impact of incorporating FFR into clinical decision making and should perform these studies in appropriately powered clinical studies.
Footnotes
Consent for Publication
All authors consented
Author’s Contributions
All authors participated in the study and have reviewed the final draft consenting for its submission
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Imperial College London Healthcare Biomedical Research Centre.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Medical databases