
Abstract
Aortic pleomorphic sarcomas are rare, aggressive vascular tumors often presenting with nonspecific symptoms that delay diagnosis. We describe a 53-year-old male who presented with isolated lower extremity claudication. Examination revealed absent pulses in the left leg, and duplex vascular ultrasound showed monophasic flow. CT angiography demonstrated a 48 mm infrarenal abdominal aortic aneurysm extending to the iliac bifurcation, a bulge in the left common iliac artery, and high-grade stenosis in a short segment. The patient underwent surgical repair with a Y-graft. Histopathological analysis confirmed undifferentiated pleomorphic sarcoma with a high Ki67 index (65%) and absence of specific immunohistochemical markers. Postoperative PET-CT revealed metastatic disease involving lungs, liver, and bones. The patient subsequently received systemic chemotherapy. This case highlights the diagnostic challenges of undifferentiated pleomorphic sarcoma when they present with isolated ischemic symptoms rather than signs of malignancy Early recognition through imaging and histopathology is essential, as surgical resection remains the cornerstone of treatment despite poor prognosis.
Introduction
Intermittent claudication, most often caused by peripheral arterial disease (PAD), results from atherosclerotic stenosis leading to inadequate blood flow during ambulation. 1 However, the differential diagnosis includes neurogenic claudication from lumbar spinal stenosis, which typically improves with spinal flexion 2 ; musculoskeletal disorders such as osteoarthritis or tendinitis3,4; and chronic exertional compartment syndrome (CECS), particularly in young, active individuals. 5 Accurate differentiation among these vascular, neurologic, musculoskeletal, and compartmental causes is essential for appropriate diagnosis and management.
Aortic pleomorphic sarcomas are rare but highly aggressive primary vascular tumors. 6 These malignant neoplasms primarily affect large arteries, especially the aorta, and histologically consist of high-grade spindle cells, epithelioid cells, or pleomorphic cells. 7 Most cases are initially asymptomatic, with symptoms varying depending on tumor size and location. These symptoms include chest pain, dyspnea, embolic events, and. aneurysm-like imaging findings. 8
The exact etiology of these tumors remains unclear, but genetic mutations and environmental factors are believed to play a role. Imaging modalities, particularly contrast-enhanced magnetic resonance imaging (MRI) and computed tomography (CT), are crucial in assessing the lesion’s relationship with vascular structures. 7 However, because of their rarity and nonspecific clinical presentation, these tumors are often misdiagnosed or detected at advanced stages. While many cases present with systemic embolic events or cardiovascular symptoms, some patients may exhibit only localized vascular compromise, making early recognition challenging.
Here, we present a rare case of aortic pleomorphic sarcoma initially manifested solely as lower extremity claudication. This case underscores the diagnostic difficulties associated with vascular sarcomas and the importance of considering vascular neoplasms in patients presenting with atypical imaging findings.
Case Report
A 53-year-old male patient presented to our clinic complaining of reduced walking distance and claudication. The patient had no cardiovascular risk factors or a history of chronic diseases. The right lower extremity pulses were palpable on physical examination, whereas the left lower extremity pulses were non-palpable. Vascular Doppler imaging revealed a monophasic flow pattern in the left lower extremity. The ankle-brachial index (ABI) was measured as 1.1 on the right and 0.2 on the left.
Based on the patient’s symptoms and physical examination findings, further evaluation with CT angiography was performed. Imaging revealed a 48 mm infrarenal abdominal aortic aneurysm at the iliac bifurcation level, along with an initial bulging and a short segment of high-grade stenosis in the left common iliac artery (Figure 1). However, the stenosis was due to aneurysmal compression, not atherosclerosis. These findings suggested that the patient’s symptoms were related to arterial obstruction secondary to aneurysmal compression and led to the decision to perform surgical intervention. (A) 48-mm Aneurysm at the Iliac Bifurcation level; (B) An Initial Bulging in the Left Common Iliac artery; (C) A Short Segment of High-Grade Stenosis in the Left Common Iliac artery; (D) Iliac Arteries Showing Similar Filling Patterns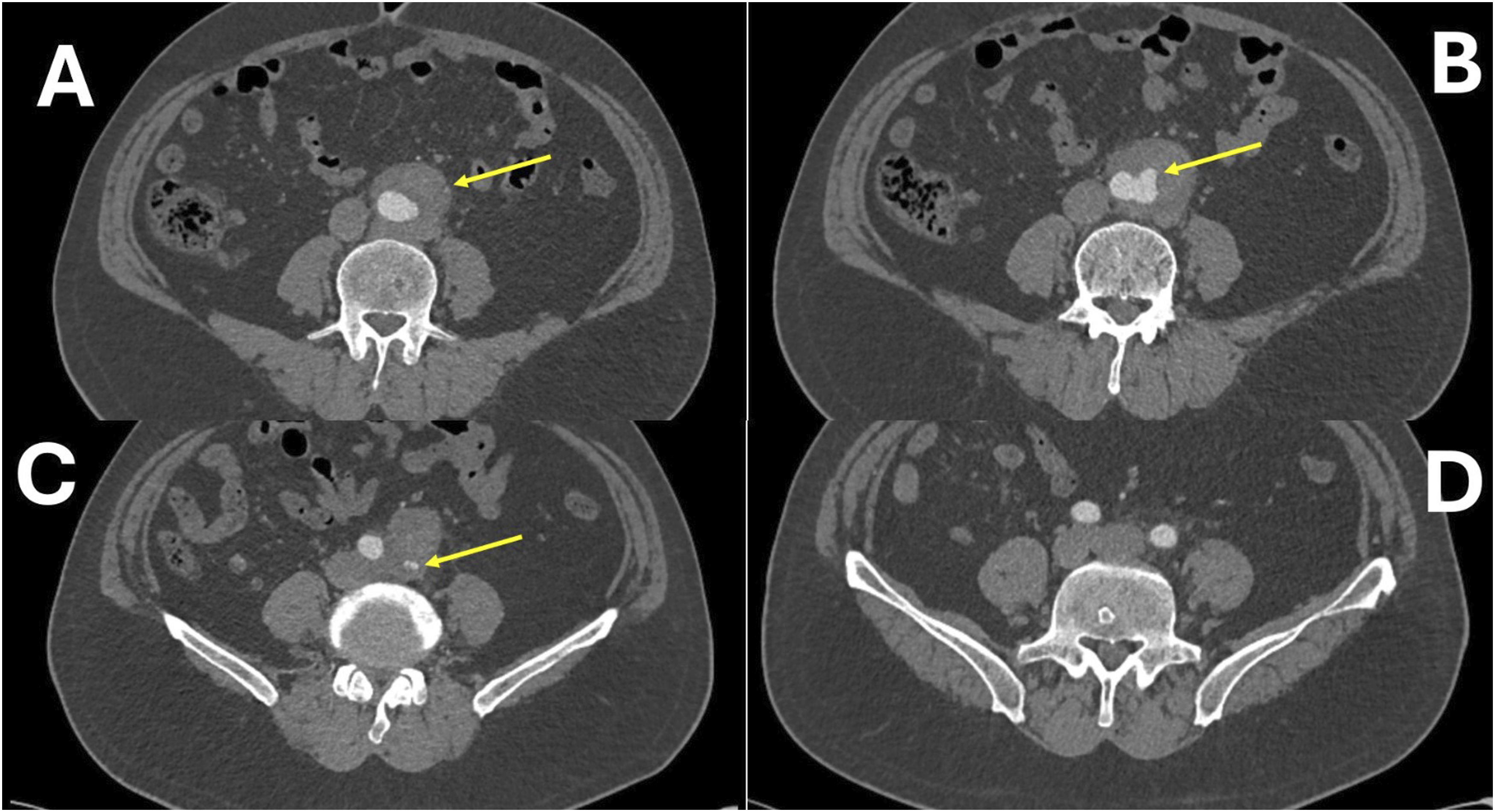
Detailed Laboratory Findings
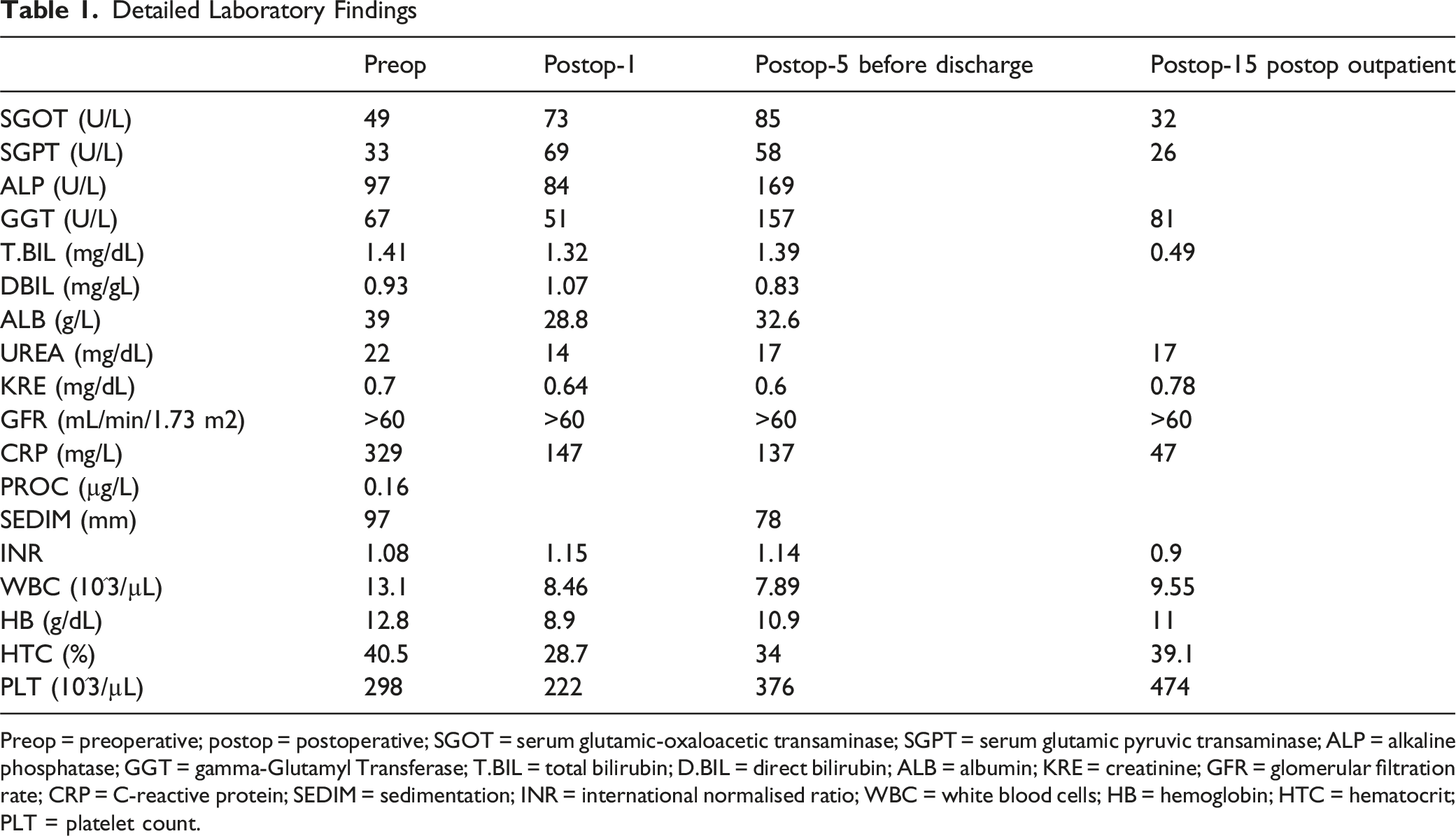
Preop = preoperative; postop = postoperative; SGOT = serum glutamic-oxaloacetic transaminase; SGPT = serum glutamic pyruvic transaminase; ALP = alkaline phosphatase; GGT = gamma-Glutamyl Transferase; T.BIL = total bilirubin; D.BIL = direct bilirubin; ALB = albumin; KRE = creatinine; GFR = glomerular filtration rate; CRP = C-reactive protein; SEDIM = sedimentation; INR = international normalised ratio; WBC = white blood cells; HB = hemoglobin; HTC = hematocrit; PLT = platelet count.
The patient underwent surgery under general anesthesia, during which infrarenal clamping was performed, and a 14-7 Y graft was implanted. Intraoperatively, the lesion was observed to have a non-atherosclerotic and atypical appearance (Figure 2). Therefore, pathological samples were taken from the aorta and surrounding lymph nodes for further examination. The procedure was uneventful, and the patient was transferred to the intensive care unit in stable condition. Intraoperative Atypical Appearance of aneurysm. P: proximal, D: Distal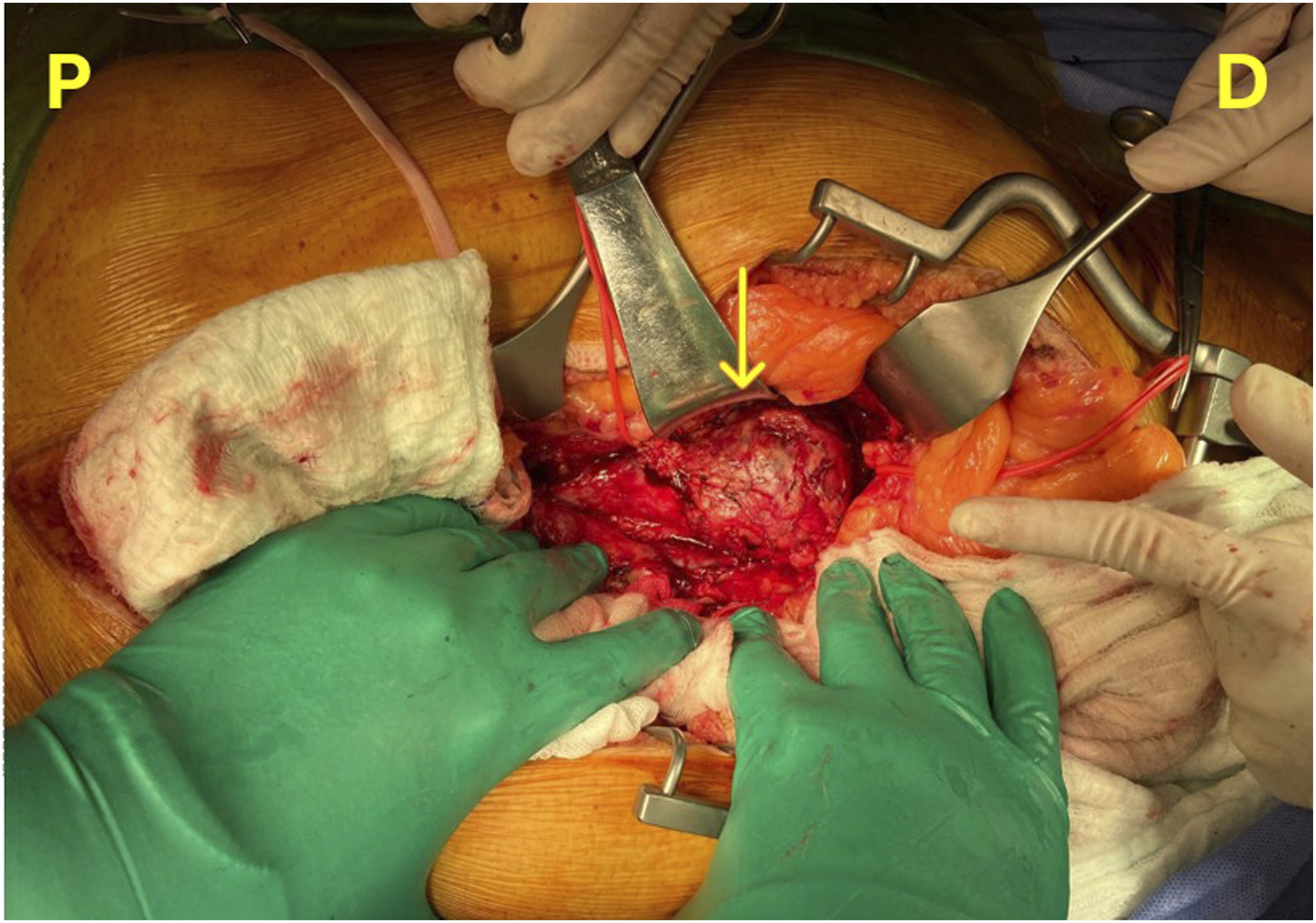
Postoperatively, the patient was extubated at the 4th hour, and hemodynamic parameters remained stable. Early mobilization was initiated on the first postoperative day, and palpable pulses were noted in both lower extremities. Postoperative ABI measurements were 1.1 on the right and 1.0 on the left. Wound healing progressed without complications, and the patient was discharged on the 5th postoperative day. Detailed laboratory findings are presented in Table 1.
Histopathological examination of the biopsy specimens revealed undifferentiated pleomorphic sarcoma. Histochemical analysis of the aortic wall showed preserved elastic fibers, while immunohistochemical staining was negative for desmin, cytokeratin AE1/AE3, CD34, S-100, and EMA. The Ki67 proliferation index was 65%, with sparse positivity in reactive cells. Lymph node analysis revealed positivity for CD20, CD10, and Bcl-6, whereas CD5, CD3, and CD43 positivity supported the presence of T-cell populations. The Ki67 proliferation index was high in germinal center cells.
Based on this diagnosis, a systemic evaluation was performed. PET-CT imaging identified widespread metastatic lesions, with significant involvement in the lungs, liver, and bones (Figure 3). The patient was discussed in a multidisciplinary oncological board, and systemic chemotherapy was initiated as the primary treatment strategy. PET CT Image of the Patient, Multifocal Metastases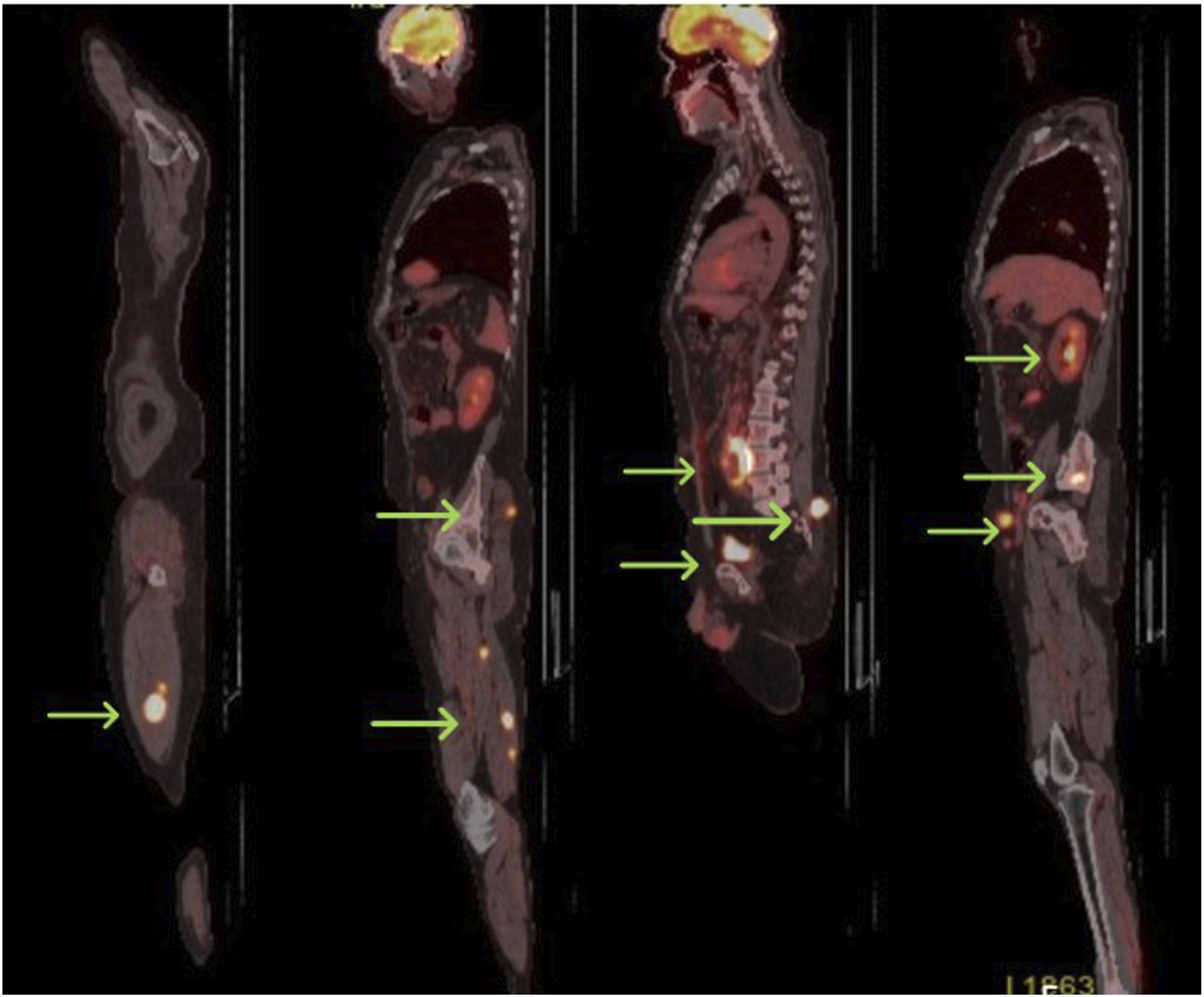
The patient has now completed the 6th postoperative month and is currently under oncological follow-up with ongoing chemotherapy treatment. He received a regimen of ifosfamide and adriamycin for oncological treatment. His current condition remains stable, with preserved lower extremity circulation. The patient’s functional status has significantly improved compared to the preoperative period, with an increased walking distance. However, due to the presence of metastatic disease, the long-term prognosis remains uncertain.
Discussion
Aortic pleomorphic sarcomas are rare tumors that are often diagnosed at an advanced stage due to their nonspecific symptoms. 6 While these tumors typically present with systemic embolic events or cardiovascular symptoms, our case highlights a much rarer presentation: isolated lower extremity claudication. This uncommon initial symptom led to a delayed diagnosis, illustrating the challenges associated with identifying vascular sarcomas in patients without overt cardiovascular complaints. In the systematic review by Rusthoven et al. 9 the majority of pleomorphic cases were diagnosed at an advanced stage, often with established metastatic disease at the time of presentation. Computed tomography angiography (CTA) typically demonstrated only intraluminal masses or arterial occlusions, whereas definitive diagnosis required histopathological confirmation. The pooled data revealed that pleomorphic subtypes were uncommon but highly aggressive, with most patients identified at late stages of disease. Prognosis was poor, with short overall survival frequently reported, and a high incidence of distant metastases observed among these patients.
In this case, CT angiography revealed a bulging appearance at the iliac bifurcation, accompanied by a short segment of high-grade stenosis in the left common iliac artery. This radiological finding raised the possibility of either direct tumor invasion or extrinsic compression by the mass effect of the sarcoma. Primary aortic sarcomas can exhibit intraluminal, mural, or extraluminal growth patterns, each with distinct clinical implications. Intraluminal tumors often lead to embolic complications, whereas extraluminal growth can result in vascular compression, mimicking atherosclerotic stenosis or aneurysmal degeneration. 9 Progressive claudication in the absence of typical risk factors for peripheral artery disease prompted further investigation with contrast-enhanced CT, which revealed an intraluminal mass extending within the distal aortic wall, raising suspicion for malignancy. While atherosclerosis and aortic aneurysms are more common causes of vascular obstruction, certain atypical imaging features—such as asymmetric bulging, abrupt luminal narrowing without significant calcification, and heterogeneous contrast enhancement—should prompt consideration of malignancy. The presence of well-maintained distal arterial flow initially suggested atherosclerotic disease; however, the atypical non-atherosclerotic intraoperative appearance of the lesion, along with histopathological confirmation of pleomorphic sarcoma, confirmed the malignant etiology. 10 This case highlights the diagnostic challenge posed by vascular sarcomas, as their imaging features can overlap with more common vascular pathologies. In cases where standard vascular pathology does not fully explain the clinical presentation, early tissue sampling and advanced imaging techniques, such as PET-CT or MRI, are crucial for achieving an accurate diagnosis and preventing delays in definitive treatment.
Surgical intervention remains the primary option for patients with obstructive vascular tumors, but preoperative suspicion is crucial in determining the appropriate management strategy. A misdiagnosed sarcoma may lead to incomplete resection or inappropriate endovascular interventions, which could delay definitive treatment. 7 Therefore, vascular surgeons and interventional radiologists should maintain a high index of suspicion in cases where imaging features are not entirely consistent with typical aortic pathologies.
The diagnosis of aortic sarcomas remains a challenge due to their rarity and the lack of specific preoperative markers. In this case, imaging played a crucial role in guiding surgical decision-making. CT angiography (CTA) often fails to detect aortic pleomorphic sarcoma, as it assesses only the vessel lumen and usually shows nonspecific findings. In contrast, 18F-FDG PET/CT identifies hypermetabolic activity in most cases, helping differentiate from benign thromboembolic or atheromatous processes and detect distant metastases. Contrast-enhanced MRI, especially with perfusion or ECG-gated cine sequences, reveals the tumor’s relationship with adjacent structures, providing critical information for surgical planning. PET/CT and MRI are essential for comprehensive staging and management but are typically reserved for patients with suspected malignancy or when the extent of disease is uncertain.11,12 While CT and MR angiography are the primary modalities for evaluating intravascular lesions, definitive diagnosis relies on histopathology. This highlights the necessity for early imaging in patients with unexplained ischemic symptoms, particularly when routine workup does not reveal an obvious cause.
Surgical resection remains the mainstay of treatment for aortic pleomorphic sarcomas, as curative options beyond surgery are limited. In this case, the tumor was resected with negative surgical margins, yet long-term prognosis remains uncertain due to the aggressive nature of these malignancies. The role of adjuvant therapy in cases where complete resection is achieved remains controversial, though the potential for recurrence necessitates close postoperative surveillance.
This case underscores the need for heightened clinical suspicion when evaluating patients with isolated claudication and no clear vascular etiology. Early imaging and timely surgical intervention may improve outcomes by facilitating diagnosis before the tumor reaches an unresectable stage. Future studies should explore optimized diagnostic pathways for vascular sarcomas to enable earlier recognition and treatment.
Conclusion
Aortic pleomorphic sarcomas are rare malignancies that can present nonspecific symptoms, making early diagnosis challenging. Since these symptoms can overlap with atherosclerotic disease, neurological disorders, or musculoskeletal conditions, maintaining a high index of clinical suspicion is essential when evaluating claudication. A detailed history and physical examination are critical to differentiate true vascular claudication from pseudoclaudication. This case highlights the importance of considering malignancy in patients with unexplained claudication and atypical vascular findings. When standard vascular pathologies do not fully explain the clinical picture, particularly in cases of rapidly progressing symptoms or unexplained obstruction, early diagnosis is crucial because it can significantly impact treatment despite the aggressive nature of the tumor. Advanced imaging modalities, such as PET-CT or MRI, and histopathological confirmation should be utilized. Early recognition and timely surgical intervention remain crucial for optimizing outcomes. Increased awareness among clinicians can help prevent misdiagnosis and facilitate prompt, appropriate management of these aggressive tumors.
Footnotes
Ethical Considerations
Ethical approval was granted by the Ethics Committee of Ege University Faculty of Medicine. The study’s ethics committee application number is 2025-4957 and its approval number is 25-4 T/53.
Consent to Participate
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Author Contributions
In this manuscript, ZÜ was responsible for data collection and writing, SK contributed to literature review and writing, and Fİ was involved in concept development and writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.