
Abstract
Background
With increasing use of imaging to diagnose human pathology, newer aortic anomalies are being identified. An intra-aortic cord is one such abnormality, which requires differentiating from an intimal flap of dissection, to avoid major surgery or prolonged surveillance. The aim of this study was to bring forth a unique feature of the intra-aortic cord on imaging, using volume rendering reformatting and identify similar findings in published literature and hence establish the role of the ‘Dimple’ sign.
Methods
Review of both our institutional imaging (2 cases) as well as the published literature (6 cases), to identify presence of a diagnostic sign that is seen on volume rendered imaging of aorta.
Results
The ‘Dimple sign’ is unique to the intra-aortic cord and is noted on the images of 4 out of 6 prior publications. Two publications did not use volume rendering. Including our cases, the Dimple’ sign is seen in 6 out of 8 cases. The Dimple sign arises due to tethering of the cord to the aortic wall leading to umbilication of the aortic wall inwards.
Conclusions
The Dimple sign can be very easily noted on volume and/or cinematic rendering and is a useful sign to diagnose an intra-aortic cord and help differentiate it from an intimal flap.
Introduction
An intra luminal cord of the aorta, is a congenital variant of aortic development. Embryologically, the development of the aorta that begins in the third week of gestation, as a complex process, makes the aorta susceptible to various congenital anomalies. In the last 2 decades, the usage of computed tomography (CT) has increased exponentially and CT angiogram (CTA) of the aorta has become the main modality of choice for aortic imaging. In addition, the aorta is a visible macro structure on all CT scans of thorax and abdomen; performed, post contrast for evaluation of any other organ or pathology. Rapid acquisition, high spatial resolution, thin slices, along with the ability to interrogate large datasets to reformat and report, has probably led to increase in identification and diagnosis of rare anomalies such as an intra-aortic cord.
An intra-aortic fibrous cord is an incidental finding and can be misinterpreted by imagers as an intimal flap of aortic dissection. It is therefore important to differentiate the 2 abnormalities on imaging and help guide patient management.
This article presents 2 cases, describes imaging features which are unique to this cord and introduces the ‘Dimple sign’ which will help future imagers to easily differentiate a cord from a flap. This sign has never been used by imagers to describe an aortic cord or other aortic pathology on a CT.
Case 1
A 71-year-old female patient, presented to emergency department with acute abdominal pain. A CT scan of the abdomen revealed ischemic bowel secondary to a superior mesenteric artery (SMA) thrombus. Surgeons undertook emergency laparotomy satisfactorily. Post laparotomy, completion imaging was performed of the thoracic aorta with a CT angiogram to find a source of the thrombus; ‘a linear horizontal filling defect in the aortic arch, spanning the aortic lumen was noted on the CT and felt most likely to be artefactual as it had an extremely atypical appearance for thrombus or dissection’ (Figure 1). CT angiogram of case 1 showing a linear intra-aortic filling defect (red arrow) on standard axial (A) and Transparent rendered reformat highlighting the umblicated ends (red arrows) that cause the dimples. (B).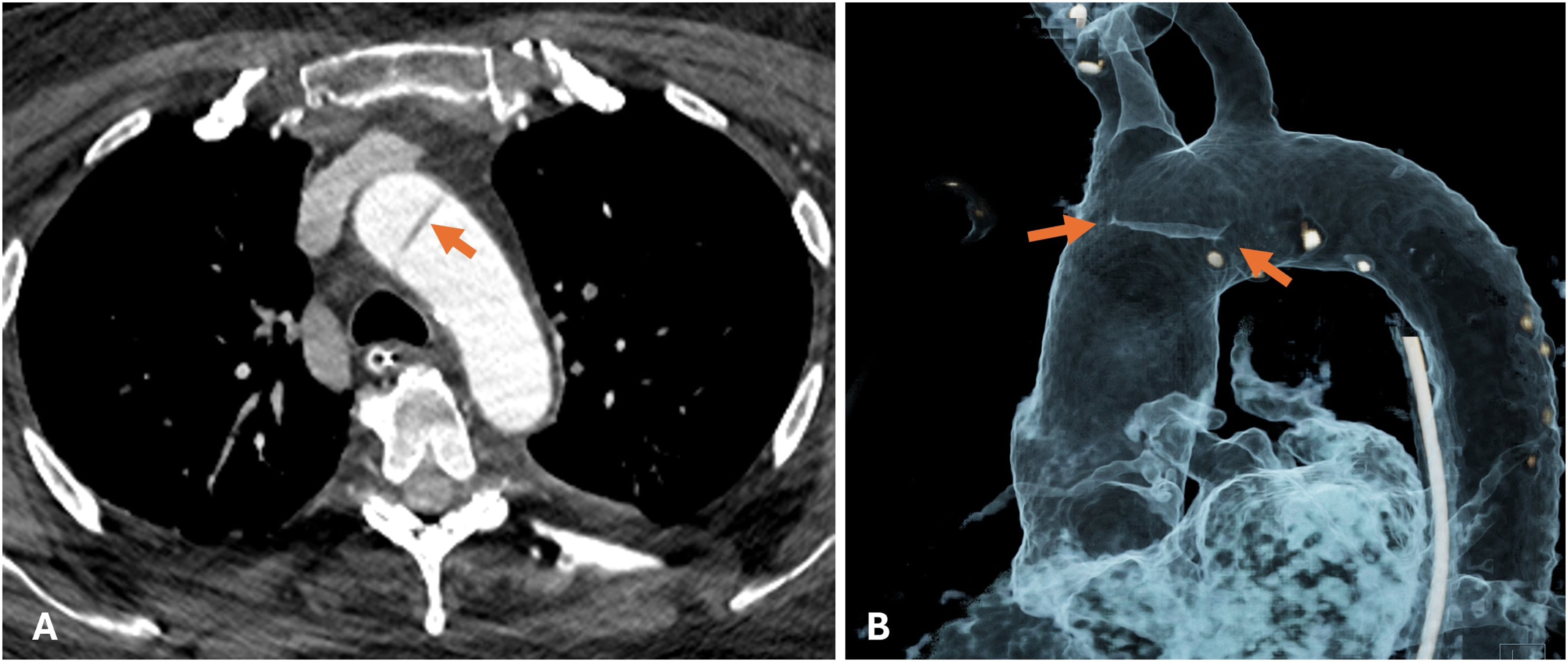
In the post operative period, patient developed new symptoms of chest pain. CT pulmonary angiogram (CTPA) was done to rule out a pulmonary embolism. The CTPA again revealed the linear horizontal filling defect as before. A dedicated review of all scans concluded the presence of a SMA origin atheroma as the possible cause of distal SMA embolization and bowel ischemia. The intra-aortic linear horizontal lesion was now diagnosed as an intra-aortic cord with classical CT features on standard axials and ‘DIMPLE SIGN’ on 3D volume or cinematically rendered images (Figure 2). Cinematic Volume rendered views of either side of aorta (A, B) reveals the ‘Dimples’ or umbilications at sites of tethering of cord to aortic wall.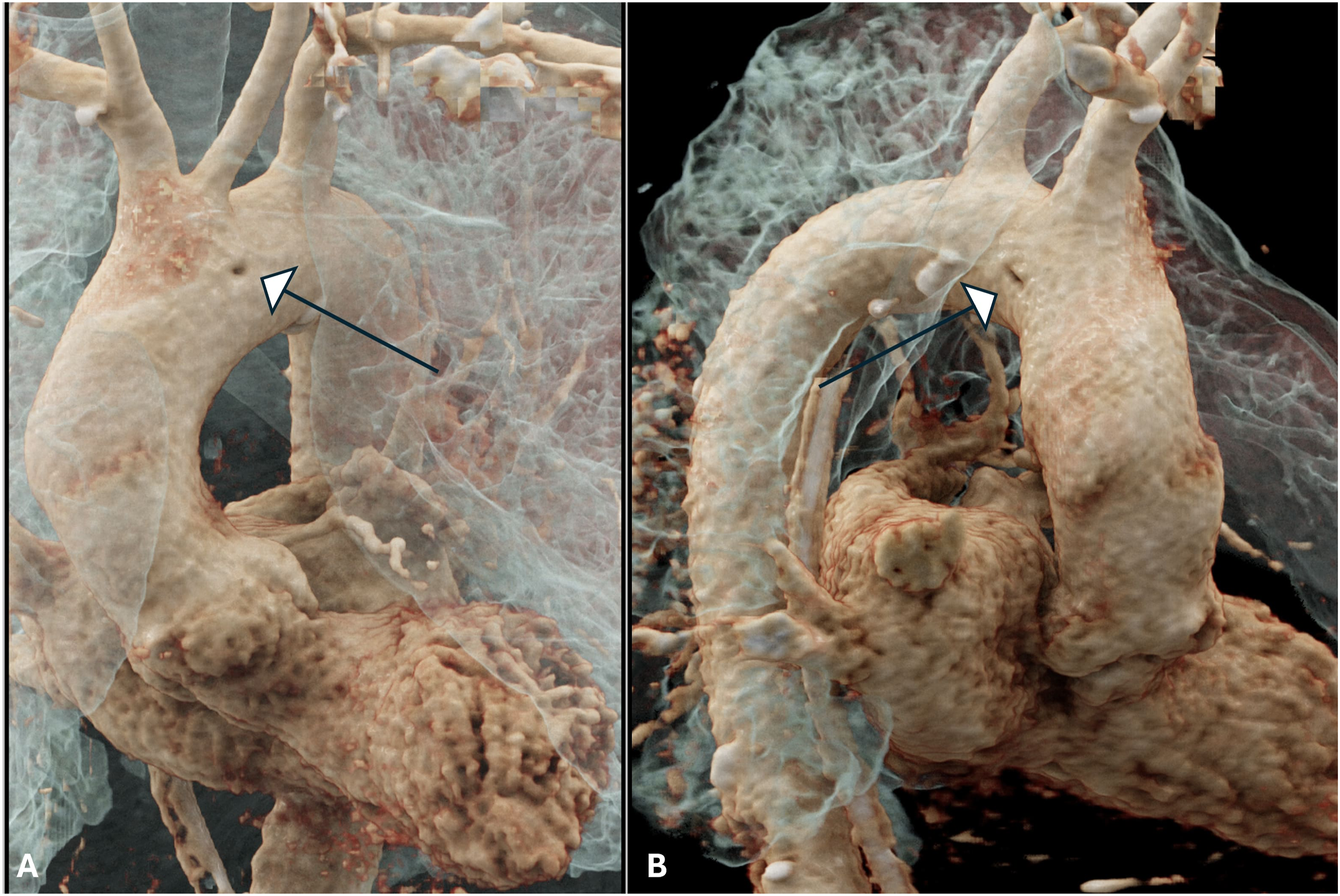
Case 2
A 45-year-old male patient, involved in a road traffic accident was brought to the emergency department. He underwent a poly trauma CT, which revealed multiple lumbar vertebral fractures and bilateral rib fractures. In addition, an intraluminal flap like lesion was noted in the infra renal aorta close to its bifurcation, suspected to be an intimal tear of the abdominal aorta. The patient underwent a repeat scan after 48 hours, which showed no change in the appearance of this ‘flap like’ suspected aortic injury. There was no remodelling of aorta. Close examination of both the CT scans showed no change in the peri aortic tissues with the soft tissue inflammatory changes and bleeding confined to the paraspinal region, in relation to the lumbar spine fractures. 3D volume rendered and cinematically rendered images once again confirmed the CT based ‘DIMPLE SIGN’ of tethering of the cord across the 2 opposite walls of the aorta (Figure 3). It was also apparent that a maximum intensity projection (MIP) can lead to obscuring of the cord Figure 4. CT angiogram volume rendered views of case 2 showing the corresponding dimples (arrows) or indentations of sites of attachment of the cord in the infra renal aorta, ruling out an acute pathology such as dissections or intimal tears.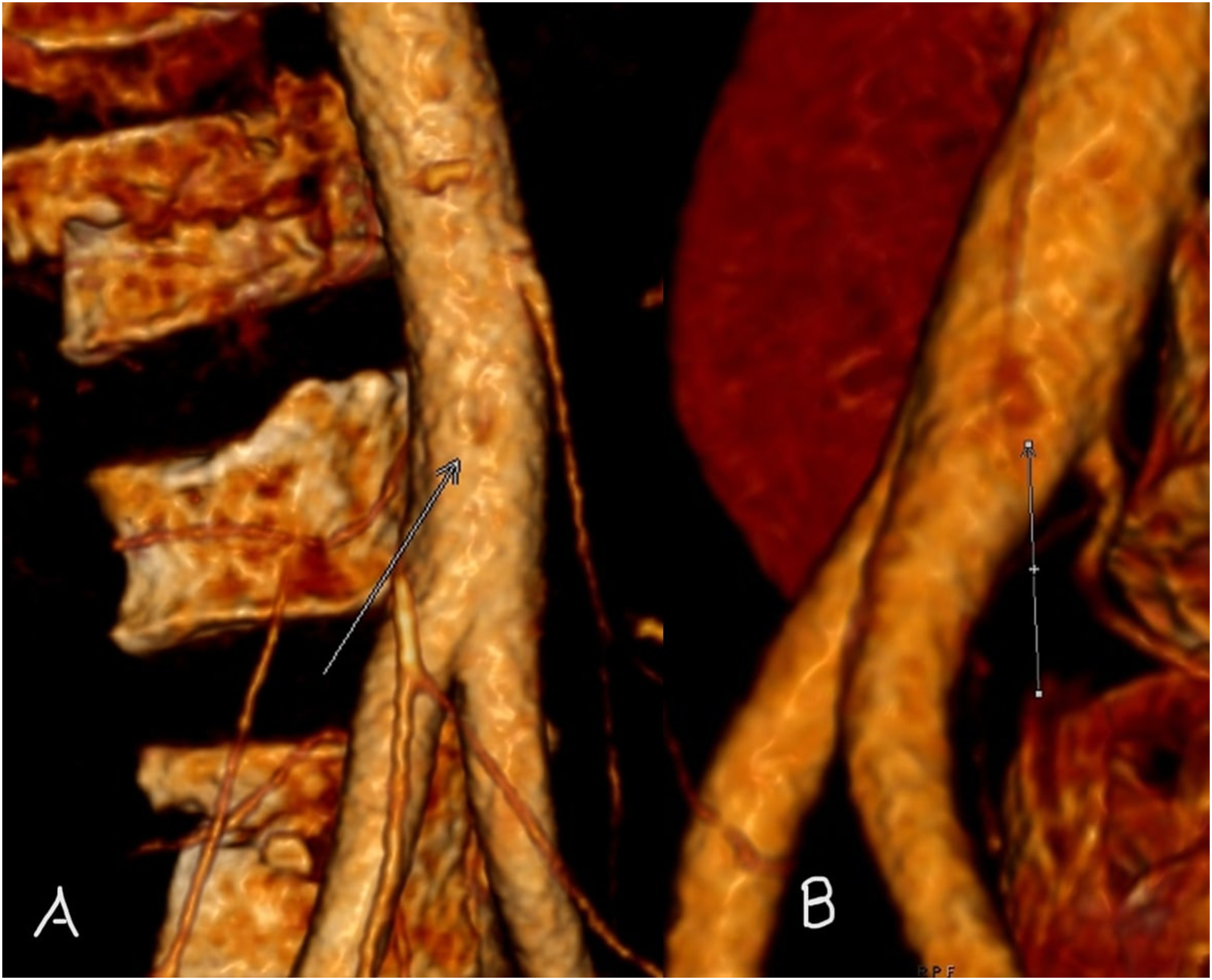
Literature Review
A review of the literature revealed only 6 published clinical reports of intra-aortic cords or bands, although congenital bands of the aortic valve have been reported more frequently since 1953.
1
The first clinical report in literature to describe an intra-aortic band like lesion was by Bonde P in 2010.
2
The cord was located along the inner arch, assumed to be a dissection flap and operated on. Intra operatively, it was noted, not to be a dissection but a band. Histopathology of the excised intimal band consisted of elastic connective tissue. More recently case reports have been published of intra-aortic fibrous cord, noted on computed tomography and magnetic resonance imaging. These reports emphasise the nature and role of the cord in the differential of a dissection flap or thrombus.3-5 Coronal multiplanar reformat (MPR) (A) and coronal maximum intensity projection (MIP) (B), reveal masking of the cord on MIP reformats and thus highlighting the need to review vascular CT on raw data at the correct window level.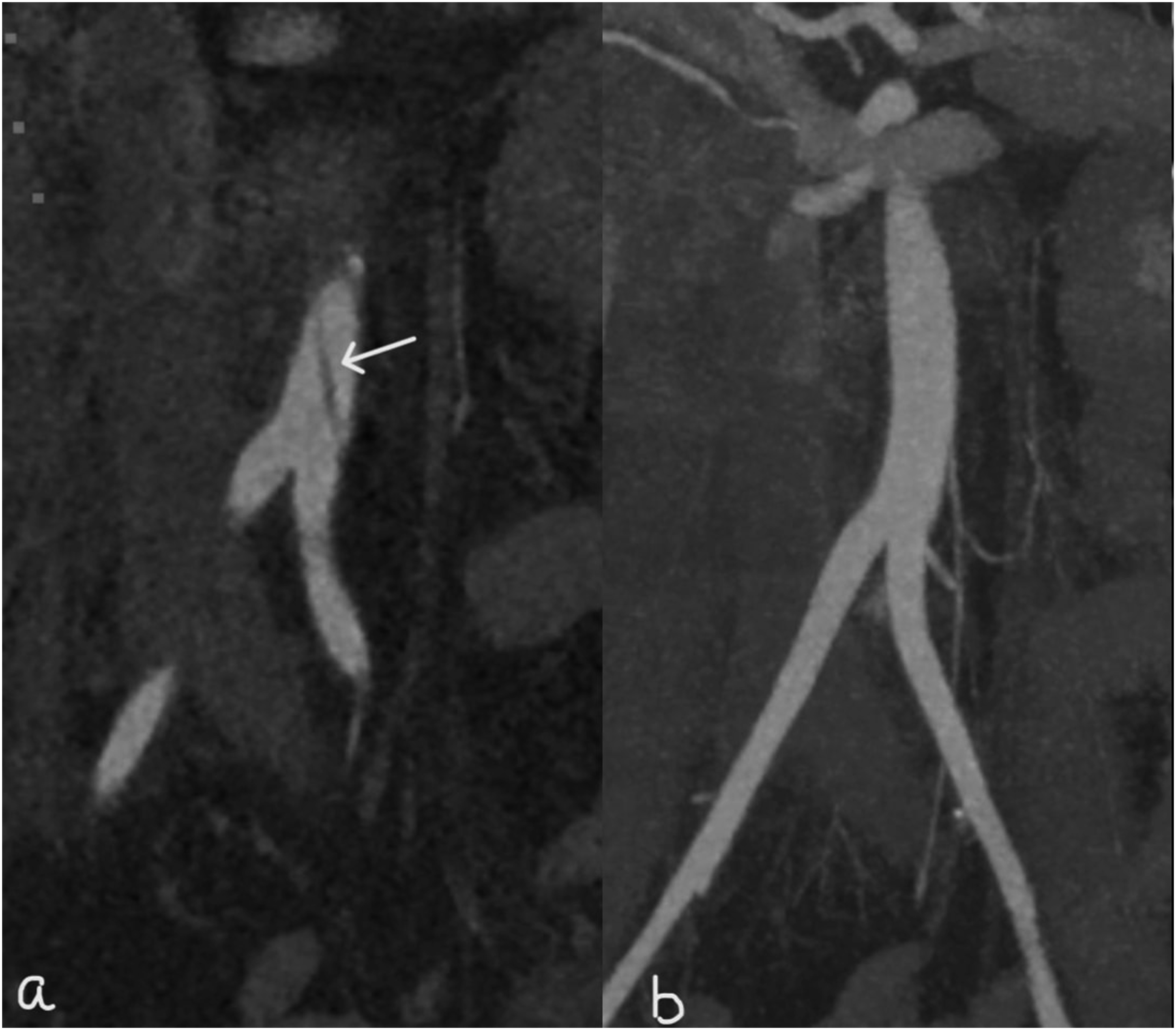
A detailed embryological reasoning is provided by d’Ostrevy et al in their case report of a cord in a patient with a stroke. 6 They propose the development of the aortic arch - which begins in the third week of gestation- is a complex process and incomplete regression to lead to vestigial remnants manifesting themselves as aortic cords especially in distal arches and this also explains the more often occurrence of the cord in the aortic arch. 7
With increasing use of imaging in clinical evaluation of patients, the intra-aortic cord, is noted in the aorta beyond the arch too.
Depicting the Publications on Intra-aortic Cord and the Occurrence or Not of the DIMPLE SIGN on Retrospective Review of the Volume Rendered CT Images as Published.
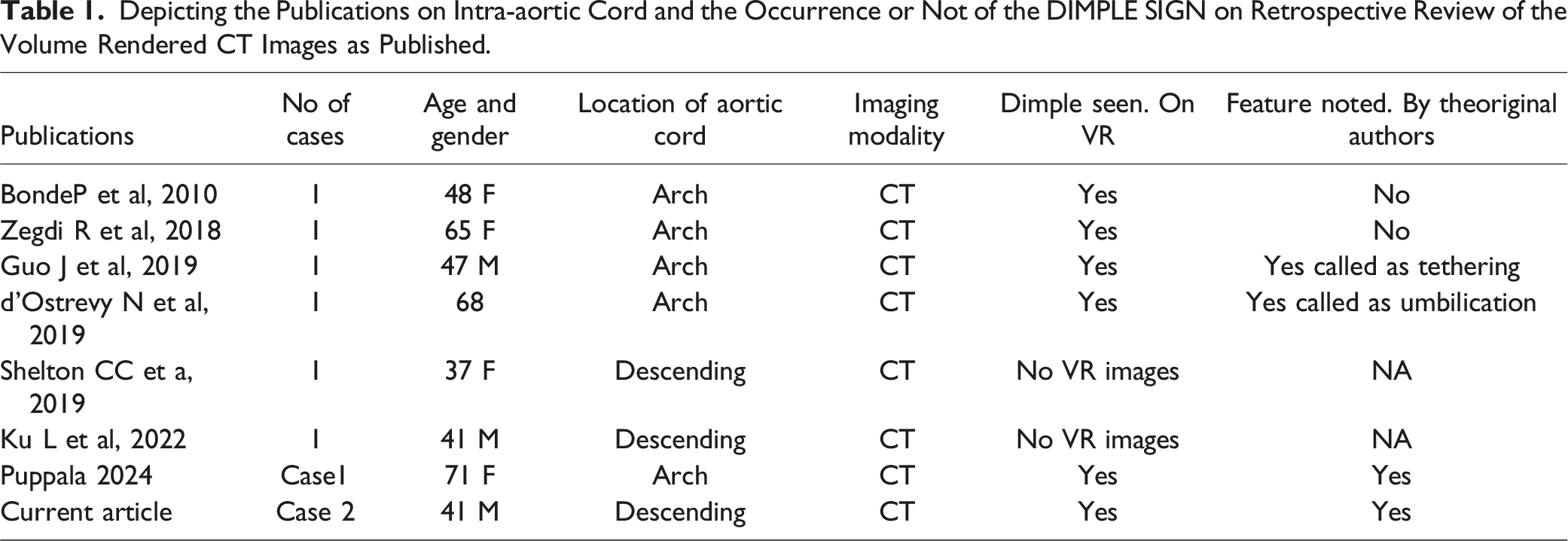
The cords or bands as reported, are no more than 1.5 to 3 mm thick (wide or diameter) and 2-5 cm in length. They can arise close to ostia of aortic branch vessels such as the subclavian artery or the common iliac artery as in our case.3,4 They are lined by intima and could predispose to thrombus formation or adherence but no case report of the same has been published. One case report of an aortic band in descending aorta that had calcified confirms the possibility of the presence of intimal lining. 8 The authors however describe it as a band and compare it to the bands found in the aortic valve. No volume rendered images are provided to confirm the presence of DIMPLE SIGN of the band that is another name for the cord.
Clinical Implication
Acute aortic syndrome and aortic intimal injuries have may mimics and pitfalls. 9 It is important to understand and identify an intra-aortic cord or band, to manage patients correctly and avoid multiple follow up imaging or an unwanted surgery. 2 It is also vital to note that MIP view can mask the cord. Although not published, the cord could be a hypothetical source of distal embolus,. A band in the aortic valve has however been reported to impair a transapical device implantation in a pig. 10
Conclusion
Intra-aortic cords and bands, need differentiating from intimal flaps to avoid unwanted surgery or repeat imaging. The ‘DIMPLE SIGN’ on volume rendered CT, is a useful unique feature of the intra-aortic cord which is not seen in other aortic pathologies and could be used to help differentiate from an intimal flap, diagnose, and guide patient management.
Footnotes
Acknowledgement
To Dr R Hyland (Consultant radiologist, UK) for manuscript and Dr P Bonde (Consultant United States of America) advise on intra-aortic cords.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.