
Abstract
Keywords
Introduction
Chronic mesenteric ischemia (CMI), a condition often resulting from stenosis of the superior mesenteric artery (SMA), is relatively rare, with research by Terlouw et al 1 indicating an incidence rate of approximately 0.000092%. Clinically, it is mainly characterized by postprandial abdominal pain, anorexia, and weight loss. Due to its atypical symptoms, it is easily misdiagnosed as other diseases. In recent years, the shift towards endovascular treatment has marked a significant change in managing SMA stenosis, with this approach becoming increasingly preferred. 2 Notably, when the SMA ostium is occluded, the success rate of antegrade opening is extremely low. While open surgery remains an option, it poses greater risks of trauma, complications, and mortality compared to endovascular methods. The endovascular technique, especially the recanalization of the SMA origin via the pancreaticoduodenal arcade using a retrograde approach, has been explored in only a few case studies, predominantly employing bare-metal stents. 3 Our report adds to this body of literature by detailing a case from our hospital of complete SMA ostium occlusion. This case was successfully managed through retrograde recanalization via collateral circulation, employing a VIABAHN covered stent.
Case Report
A 60-year-old female patient, with a medical history of diabetes and hypertension, was admitted to the hospital due to recurring postprandial abdominal pain and anorexia persisting for 2 months. Diagnostic evaluations, including routine blood work, liver and kidney function tests, abdominal ultrasonography, and computed tomography angiography (CTA), led to the diagnosis of an occlusion in the SMA. The aortic CTA detailed 2 key findings: firstly, an occlusion at the SMA’s origin and mild narrowing at the origins of both the celiac axis (CA) and inferior mesenteric artery (IMA); secondly, it revealed the presence of multiple mixed and calcified plaques in the abdominal aorta, bilateral common iliac arteries, and the right external iliac artery, contributing to irregular luminal diameters.
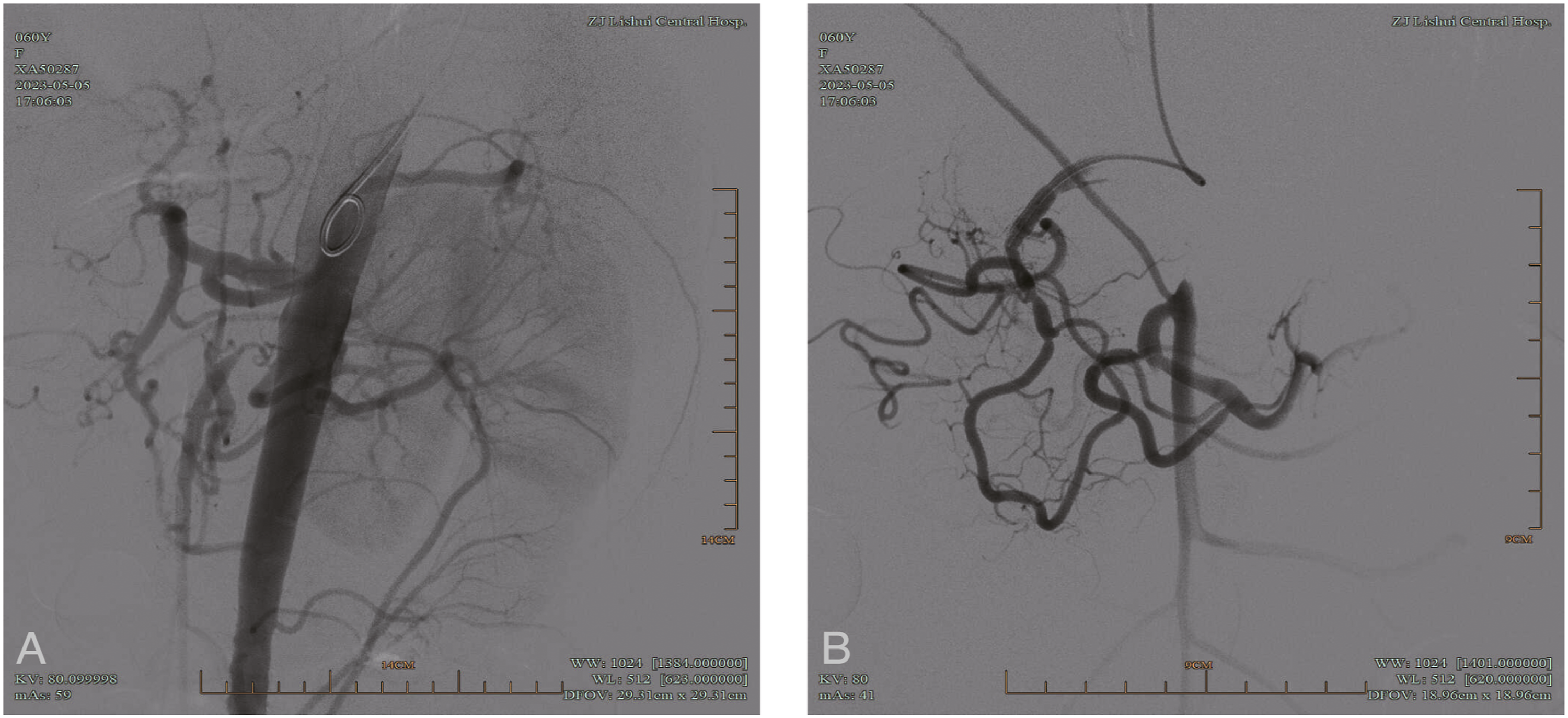
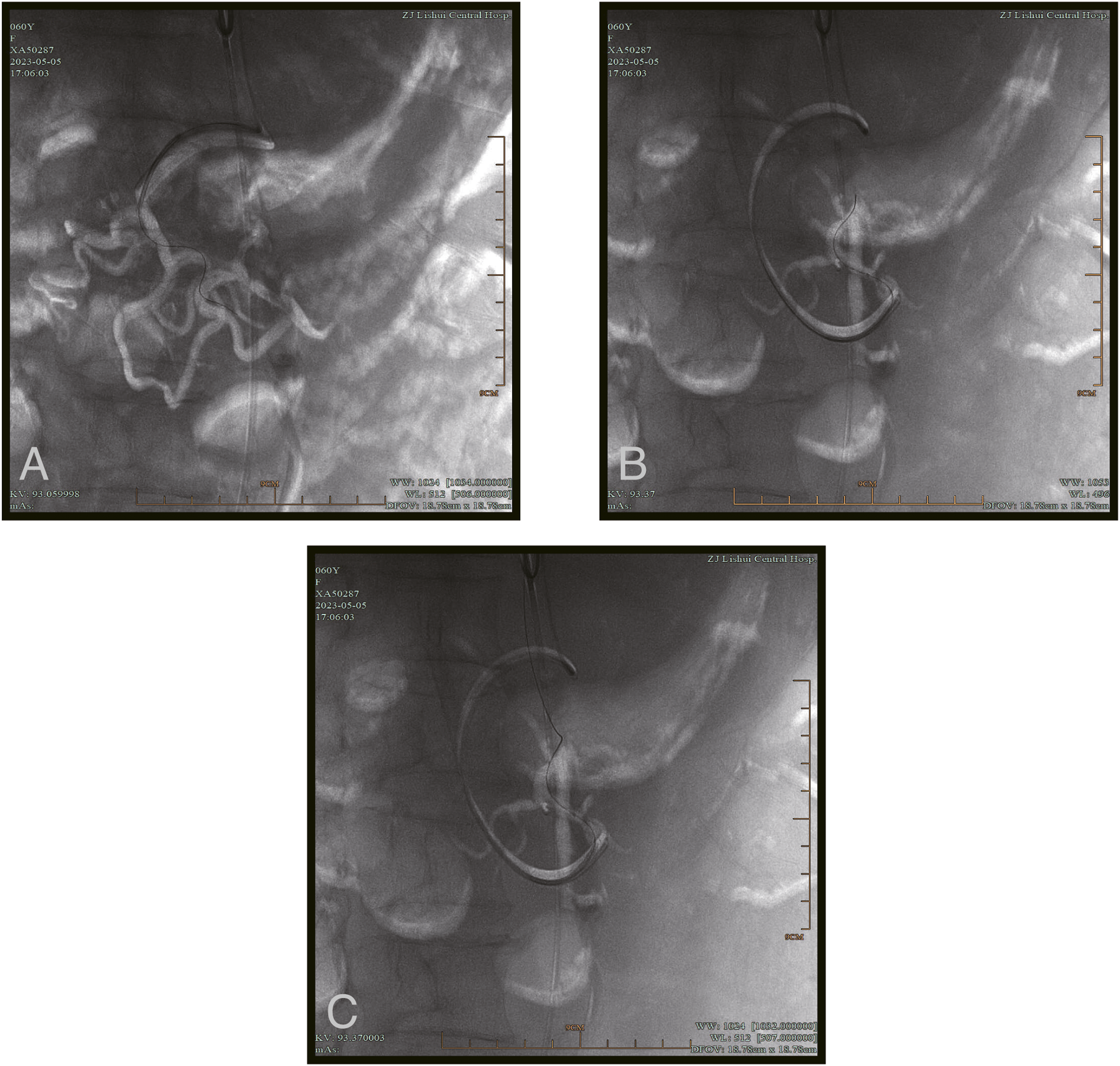
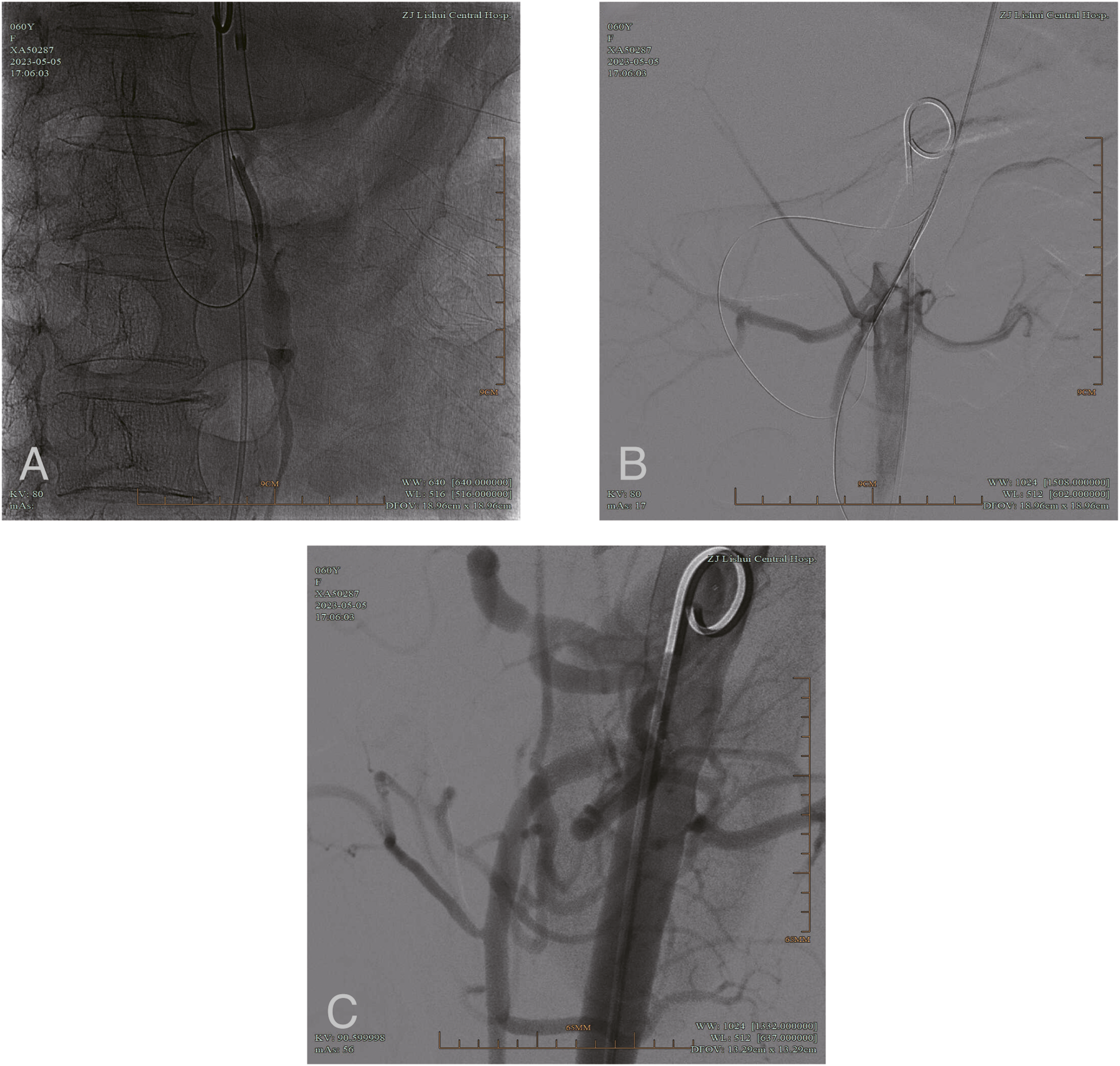
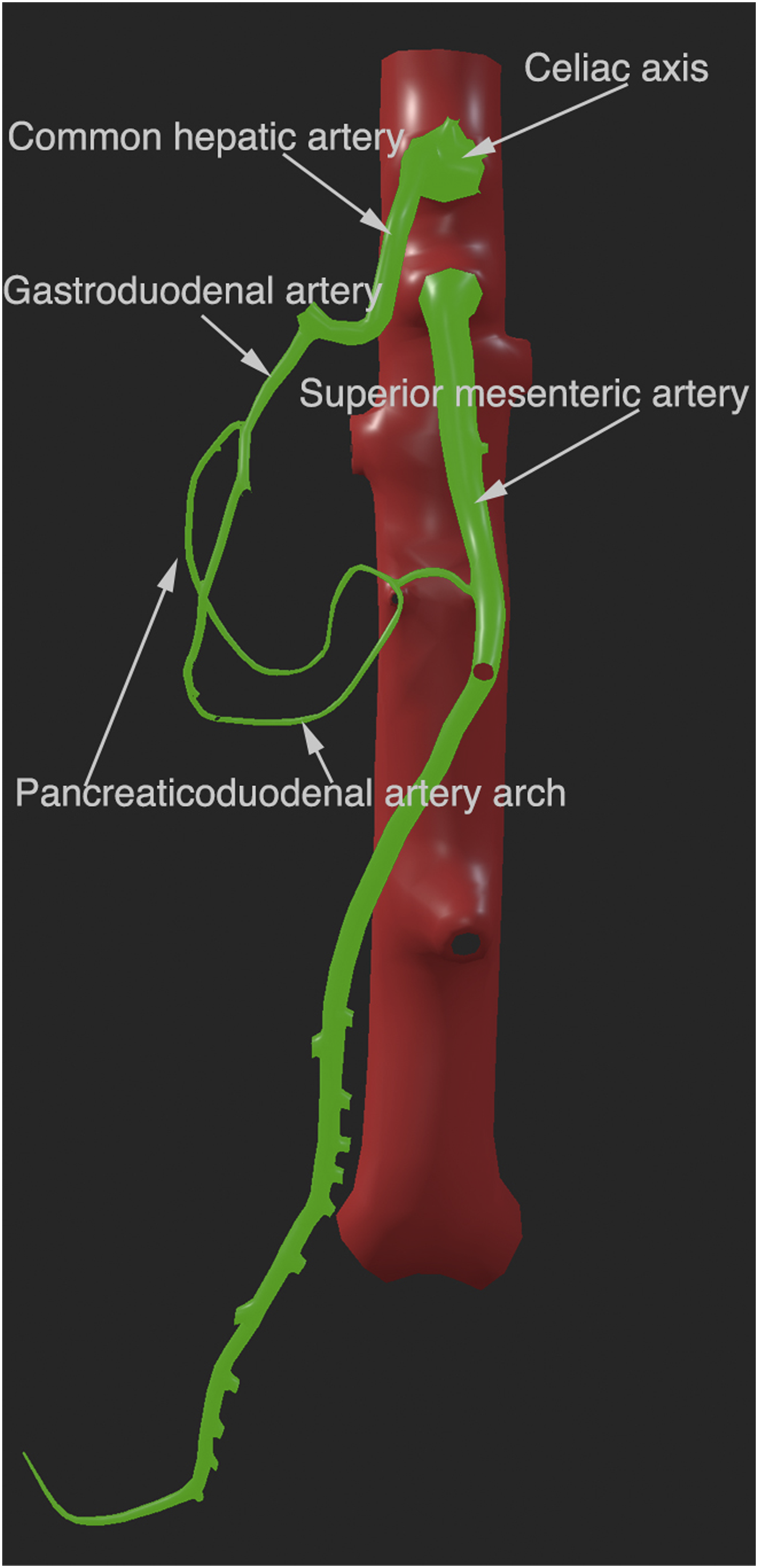
Preoperative CTA revealed an occlusion at the SMA’s opening, extending approximately 2 cm, with compensatory hypertrophy of the pancreaticoduodenal artery arch between the CA and SMA (Figure 1). Prior to the endovascular treatment, a 5F sheath (TERUMO, Shibuya, Tokyo, Japan) was inserted through a puncture in the left antecubital fossa, subsequently exchanged for a 6F, 90 cm long sheath (Cordis, Miami Lakes, Florida 33014, USA) and a pigtail catheter (Cordis, Miami Lakes, Florida 33014, USA). Intraoperative abdominal aortography confirmed the complete occlusion at the SMA’s origin. For detailed imaging, a 5F pigtail catheter was inserted into the right femoral artery. The 6 F sheath allowed the advancement of a multipurpose angiographic (MPA, Cordis, Miami Lakes, Florida 33014, USA) catheter into the gastroduodenal artery. Hand-injected angiography through this setup revealed significant compensatory hypertrophy of collaterals between the CA and SMA (Figure 2). A microcatheter (Boston Scientific, Marlborough [https://www.bostonscientific.com/en-US/products/embolization/Renegade_HI-FLO_Microcatheter.html]), accompanied by a V-14 guidewire (Boston Scientific, Marlborough, MA, USA) and guided by the roadmap, navigated retrogradely through the pancreaticoduodenal artery arch, crossing the occluded segment into the abdominal aorta (Figure 3). Following this, a 3 mm × 30 mm pre-dilation (ClearStream Technologies, Enniscorthy County Wexford, Ireland) was performed, and a V-18 guidewire (Boston Scientific, Marlborough, MA, USA) was antegradely placed through the SMA using the post-dilation vascular channel (Figure 4A and B). A 6 mm × 25 mm VIABAHN (W. L. Gore & Associates, Newark, USA) covered stent was then introduced and centered on the occlusion, extending slightly into the abdominal aorta. The stent was deployed and post-dilated with a 5 mm balloon (Cook Medical, Bloomington, USA). Subsequent angiography confirmed the stent’s optimal placement, with the SMA remaining patent and distal vessels clearly visualized (Figure 4C). The procedure concluded with the removal of the catheter sheath and the application of pressure dressing at the puncture site. Postoperative administration of at least 6 months of dual antiplatelet therapy with aspirin and clopidogrel. The main retrograde approach during the treatment process is shown in Figure 5. Preoperative imaging from computed tomography angiography suggested that the pancreaticoduodenal arcade, located between the celiac axis (CA) and the superior mesenteric artery (SMA), had undergone compensatory hypertrophy. Intraoperative angiography. (a) Abdominal aorta angiogram showing SMA origin occlusion, (b) gastroduodenal artery catheterization revealing compensatory hypertrophy in the pancreaticoduodenal arch between CA and SMA. Intraoperative angiography depicting retrograde passage through the pancreaticoduodenal artery arch. (a) Deployment of a multipurpose angiographic (MPA) catheter in conjunction with a V-14 guidewire and microcatheter, facilitated by roadmap navigation into the pancreaticoduodenal artery arch, (b) targeting the SMA stenotic segment, (c) translesional entry into the abdominal aorta. Angiography post-balloon dilation and stent implantation. (a) Balloon dilation of the occluded segment, (b) utilizing the pre-dilated channel for antegrade passage through the SMA with placement of a V-18 guidewire, (c) implantation of a 6 mm × 25 mm VIABAHN covered stent and post-dilation, with angiography via a pigtail catheter placed in the femoral artery. Retrograde approach diagram. The green section depicts the retrograde route starting from the celiac trunk, progressing through the common hepatic artery to the gastroduodenal artery, and extending to the pancreaticoduodenal arterial arc which connects to the superior mesenteric artery.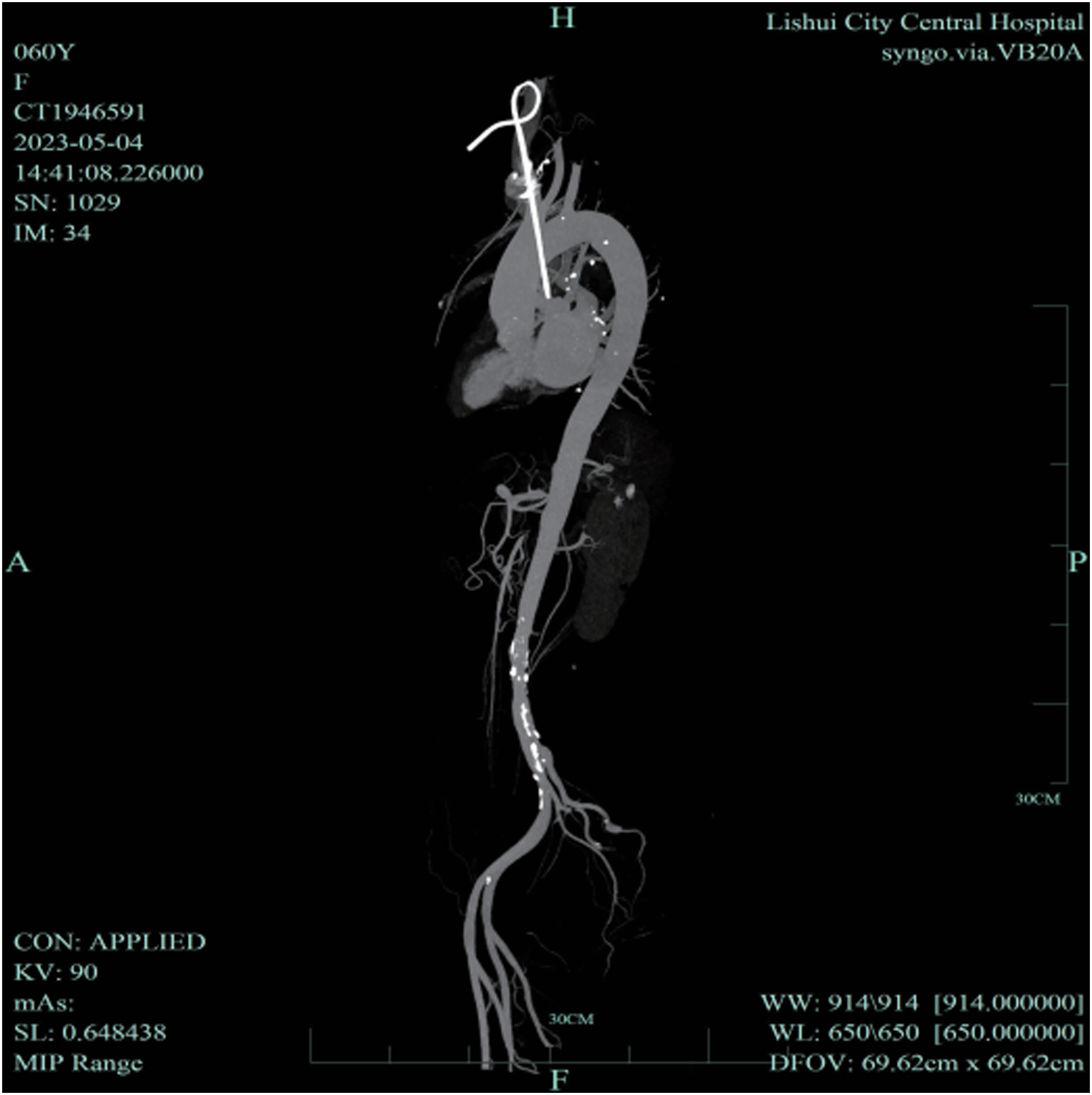
The patient’s abdominal pain resolved postoperatively, and she resumed normal eating by the second day. A 6-month follow-up CTA showed the SMA stent well-maintained, with clear imaging of the distal SMA, confirming the success of the intervention (Figure 6). CTA at 6-month post-operative follow-up.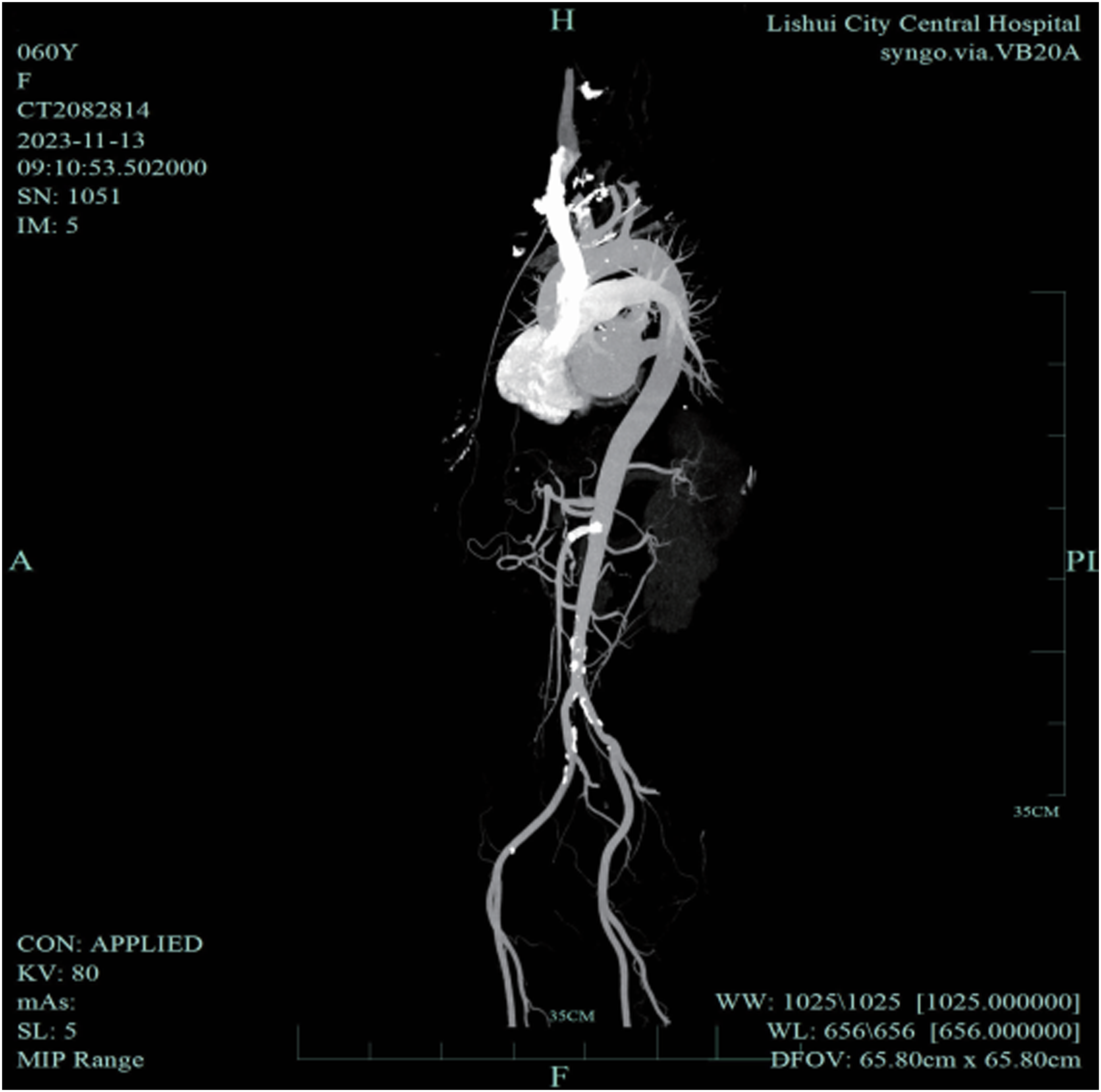
Informed Consent
Informed consent has been obtained from all individuals included in this study.
Ethical Approval
The research related to human use has been complied with all the relevant national regulations, institutional policies, and in accordance with the tenets of the Helsinki Declaration and has been approved by Ethics Committee of Lishui Municipal Central Hospital.
Discussion
Mesenteric ischemia, a condition where visceral arteries fail to supply sufficient blood to meet metabolic demands, can be acute (AMI) or chronic (CMI), with arteriosclerosis being a notable factor in CMI. SMA stenosis or occlusion, the most severe form of CMI, often presents as postprandial abdominal pain and weight loss. Acosta’s epidemiological studies show a prevalence of 12.8 cases per 100 000 annually, accounting for 1%–2% of gastrointestinal diseases.4,5 Its rarity and vague symptoms often lead to misdiagnosis and inappropriate treatment. Advances in imaging technologies, particularly CTA, has enabled more effective identification of SMA stenosis cases, predominantly occurring at the artery’s origin. These cases often escalate to acute mesenteric arterial thrombosis, with mortality rates much higher than those for acute mesenteric arterial embolism, owing to the broader impact on blocked vessels and the intestinal segment involved. In light of the severe implications of SMA lesions, proactive intervention is advocated when stenosis exceeds 70%. 6
The primary objective in treating SMA stenosis is to re-establish intestinal blood flow, aiming to alleviate pain, prevent intestinal gangrene, and improve nutritional status. 6 Surgical options mainly consist of antegrade and retrograde bypasses. The antegrade bypass, which involves creating a pathway from the abdominal aorta above the celiac trunk to the SMA, interrupts the renal-abdominal aorta but offers the benefit of maintaining forward arterial flow and achieving high long-term patency. 7 However, this method poses risks such as hemodynamic instability and potential distal arterial embolism. Alternatively, the retrograde bypass, extending from the distal abdominal aorta or iliac artery to the SMA, presents a less complex anatomical challenge but risks twisting the graft vessel. 8
With advancements in interventional techniques, endovascular treatment has emerged as the preferred approach for SMA stenosis. 9 In their study, Wu et al introduced a technique that involves making an incision in the abdomen to access the distal segment of the Superior Mesenteric Artery (SMA). They then performed a puncture under roadmap guidance, followed by retrograde insertion of a catheter guidewire for the purpose of stent implantation. 10 In a similar context, Chen YH and his team adopted a method that begins with a minor abdominal incision to reveal the mesentery. This procedure involves using ultrasound guidance for puncturing the distal SMA, followed by retrograde traversal of the occlusion into the abdominal aorta, and then connecting a catheter, inserted via the brachial artery, to a retrograde guidewire for antegrade passage through the lesion. The procedure is completed with balloon dilation and stent placement. 11 Both techniques, which fall under hybrid surgery, are marked by significant trauma, complexity, and heightened risks of vascular complications like rupture, dissection, and bleeding due to the retrograde approach to vessel puncture.
The extensive collateral circulation exists among the three visceral arteries: the CA, SMA, and inferior mesenteric artery (IMA). Typically, the CA communicates with the SMA via the pancreaticoduodenal arcades. Obstructions in these main visceral arteries can lead to varying degrees of collateral circulation enlargement, a concept central to the retrograde recanalization of the SMA. Detailed review of preoperative and intraoperative imaging is crucial to determine the feasibility of this approach. The advantages of retrograde opening, similar to those in arteriosclerosis obliterans (ASO) of the lower extremities, include: 1) Easier navigation through lesions due to less dense calcification and fibrous content in atherosclerotic plaques at distal ends; 2) Reduced risk of accidental entry into arterial branches; 3) This approach enhances the likelihood of entering the true lumen in instances where smaller vessels enter larger ones subintimally; 4) In cases of obstructed antegrade recanalization, further attempts might exacerbate a dissection. Conversely, retrograde recanalization, moving upward through the occluded segment, lessens the risk of worsening a dissection due to the reverse blood flow direction.12–15 Additionally, retrograde recanalization is no longer applicable when there is insufficient collateral compensation or when anatomical abnormalities are present.
In the realm of SMA stenosis treatment, endovascular therapy offers distinct advantages over surgical methods, including reduced trauma, higher rates of technical success, expedited postoperative recovery, fewer complications, and lower mortality. 16 Despite these benefits, one notable limitation of endovascular treatment is its inferior long-term patency compared to surgical bypass. The standard practice in endovascular intervention currently involves the use of self-expanding metal bare stents for SMA opening lesions. These stents, however, are prone to in-stent restenosis (ISR), primarily due to intimal hyperplasia and the inherent structural deficiencies of their mesh design. 17
To mitigate these issues, the introduction of VIABAHN covered stents marks a significant advancement. The stents provide better flexibility and radial support, leading to enhanced long-term patency rates. 18 Drawing upon our experiences from treating central venous stenosis (CVS), we adapted this technology for a case of SMA opening occlusion being reported here. 19 This application reflects a strategic adaptation of the technique, showcasing its versatility and effectiveness in different vascular contexts. A notable advancement in this area was reported by Kirii et al, in 2021, who described the successful retrograde recanalization through the celiac axis with the implantation of a covered stent for treating occlusions at the origin of the SMA. 20 Furthermore, research indicates that stents coated with expanded polytetrafluoroethylene, particularly those with a heparin coating, effectively reduce platelet aggregation and inhibit intimal proliferation.21,22 Such covered stents are also known to be beneficial in addressing intimal injury and reducing the detachment of arterial wall emboli.
Conclusion
The results of this study demonstrate that the retrograde treatment of SMA opening lesions via the pancreaticoduodenal artery arch using a VIABAHN covered stent is a highly safe and minimally invasive endovascular treatment method. The near to midterm efficacy is confirmed to be positive.
Footnotes
Acknowledgments
The authors would like to thank the patient for his willingness to give his consent and approval for publication of this report.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Zeyi Zhao. The first draft of the manuscript was written by Jie Zhang. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. Jie Zhang and Zeyi Zhao contributed equally to the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during this study are available from the corresponding author on a reasonable request.