
Abstract
Purpose
We report the case of an acute type B dissection with high-risk features treated with multilayer stent.
Case Report
A 50-year-old female patient presented to the emergency department with an acute type B aortic dissection. Conservative medical treatment did control blood pressure but did not alleviate her dissection symptoms. She was treated endovascularly with multilayer stents extensively covering the whole dissected area. HThe aortic arch side branches, visceral arteries and renal arteries remained patent after treatment. The recovery was uneventful, and she was discharged the day after the intervention. At 6- and 12-month follow-up, the patient remained asymptomatic, the true lumen volume increased and all side branches remained patent.
Conclusion
We present a case of the use of a multilayer stent for acute type B aortic dissection. This technique allows to treat the whole dissection with low risk of paraplegia or side branch occlusion. Long-term results of ongoing clinical studies should confirm the place of the multilayer stent as a treatment option for type B aortic dissection.
Keywords
Introduction
The optimal treatment for type B aortic dissections (TBAD) is still a matter of debate, despite developments in surgical and endovascular techniques. For uncomplicated TBAD, medical treatment of hypertension remains the gold standard. 1 In case of complicated TBAD (e.g., rapid aortic expansion, aortic rupture and/or hypotension/shock, visceral, renal, or limb ischemia, paraplegia/paraparesis, peri-aortic hematoma, recurrent or refractory pain, and refractory hypertension despite adequate medical therapy), invasive treatment should be considered. In recent years thoracic endografts have been widely accepted as the preferred treatment choice mainly because of their lower complication and mortality rates compared to an open surgical procedure.2,3 However, when the dissection extends into the distal thoracic or visceral aorta, and requires treatment, traditional stent grafts which would increase the risk of aortic branch occlusion, resulting in stroke or paraplegia, 4 are not appropriate. In such situations, additional treatment with bare metal stents (Provisional ExTenTion to Induce COmplete ATtachment - PETTICOAT) may be considered. Nevertheless, long-term results with this approach showed progressive dilatation of the distal aorta prompting the need for additional options.5,6
The multilayer stent (Intressa Vascular; Isnes, Belgium) is a self-expanding, multilayer, cobalt alloy stent consisting of a three-dimensional braided wire mesh. Despite inconsistent results in aortic aneurysm, 7 the stent has raised physician’s interest for the treatment of dissection due to its mechanical properties, reopening the true lumen by approximating the dissection flap to the aortic wall and providing mechanical support to the aortic wall. 8 This recentralizes blood flow in the true lumen and stabilizes the dissection, while ensuring the aortic branches remain patent through the open mesh design of the stent. 9
In this paper we report on the use of the multilayer stent as emergency treatment of an acute TBAD.
Case Report
A 50-year-old female presented to the emergency department at the onset of acute severe chest and upper back pain. Her medical history consisted of controlled stage II hypertension, treated with losartan. No other comorbidities were present. Laboratory testing showed normal kidney functions. Blood pressure was 170/90 mmHg at presentation.
Subsequent diagnostic contrast-enhanced computed tomography (CT) revealed a type B aortic dissection (TBAD) that extended from the left subclavian artery (LSA) to the right common iliac artery (RCIA) (Figure 1A). Only the right renal artery (RRA) originated from the false lumen. The maximum compression was at T5 level, where the true lumen was compressed to less than 10% of the total diameter (Figure 1B). CT-scan at presentation. A: Type B aortic dissection extending from left subclavian artery to right common iliac artery. B: Compression of the true lumen at T5 level.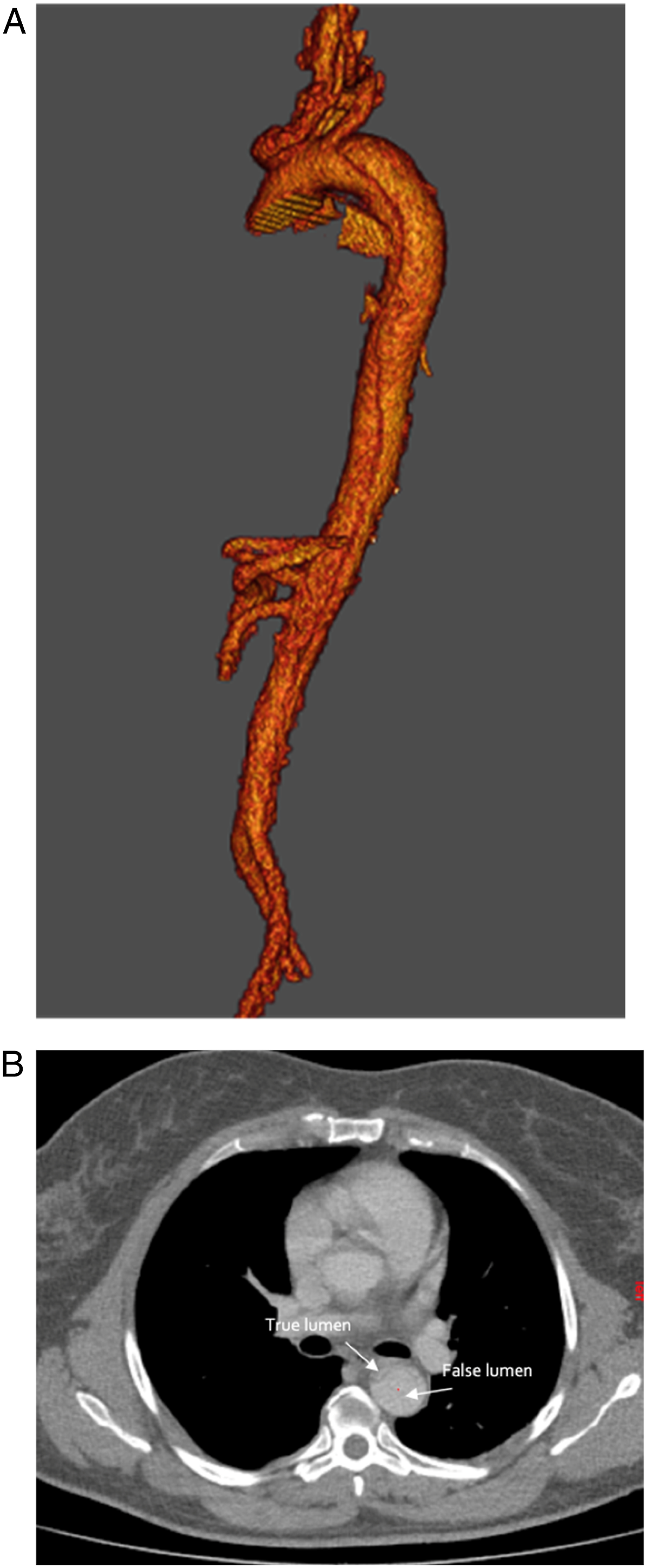
Despite primary medical treatment with intravenous metoprolol and sodium nitroprusside and oral beta blockers controlling the blood pressure, the patient’s symptoms did not improve. Because of her persistent back pain over 4 days, invasive treatment was deemed necessary. Moreover, due to the involvement of the visceral aorta into the dissection, it was deemed necessary to treat the dissected aorta extensively. As the site was located in the Brazilian state of Tocatins, more than 2000 kilometers away from the closest vascular center, the decision was made to treat the patient locally.
The procedure was performed on day 4 after symptoms onset, under local anesthetic and sedation. Unilateral ultrasound-guided right femoral access was obtained by a preclose technique with two Proglide devices (Abbot Vascular, Santa Clara, California). Proper guidewire introduction and advancement in the true lumen was ensured by angiographic guidance. Through a 20 Fr sheath, two overlapping multilayer stents were implanted. To ensure a sufficient healthy landing zone and obtain adequate proximal seal, decision was made to deliver the proximal stent over the aortic arch. The open mesh structure of the multilayer stent made this possible, ensuring preserved perfusion of the supra-aortic branches.
No rapid pacing nor adjunctive procedure were necessary for the deployment of the stents. Angiogram at the end of the procedure showed approximation of the entry tear and total exclusion of the false lumen in front of the entry tear, with patent side branches, particularly the supra-aortic arteries, mesenteric arteries and both renal arteries. Total procedure time was 68 minutes. Less than 100 milliliters of contrast agent were administered.
The patient was completely asymptomatic after the procedure. She remained in the ICU (Intensive Care Unit) for 12 hours postoperatively. There were no signs of stroke or spinal cord ischemia. Postoperative kidney function tests remained normal. The next day she was discharged from the hospital in good health. Dual antiplatelet therapy (DAPT), i.e., clopidogrel and acetylsalicylic acid, were started as per our site standard practice after endovascular procedures.
At follow-up examinations after 6 and 12 months, the patient remained asymptomatic. Review of the CT scans confirmed that the stent had reopened the true lumen to the original aorta diameter, with stable true and false lumen diameters and volumes between 6 and 12 months. The 12-month follow-up CT scan revealed that the false lumen at the proximal end of dissection completely disappeared (Figure 2A). Also, the maximum diameter of the false lumen significantly decreased whereas the true lumen diameter increased (Figure 2B). All supra-aortic and visceral branches were patent (Figures 2C and 2D). CT-scan at 12-months follow-up. A: Complete remodeling of the aorta at entry tear level with an increase of the true lumen diameter from 13.7 mm prior to the implantation (left hand side image) to 30.5 mm at 12 months (right hand side image). B: Increase of the true lumen diameter after the stent implantation, example: increase at the right renal artery ostium level from 9.2 mm prior to the implantation (left hand side image) to 18.7 mm at 12 months (right hand side image). C: Patent aortic arch vessels. D: Patent visceral and small intercostal arteries.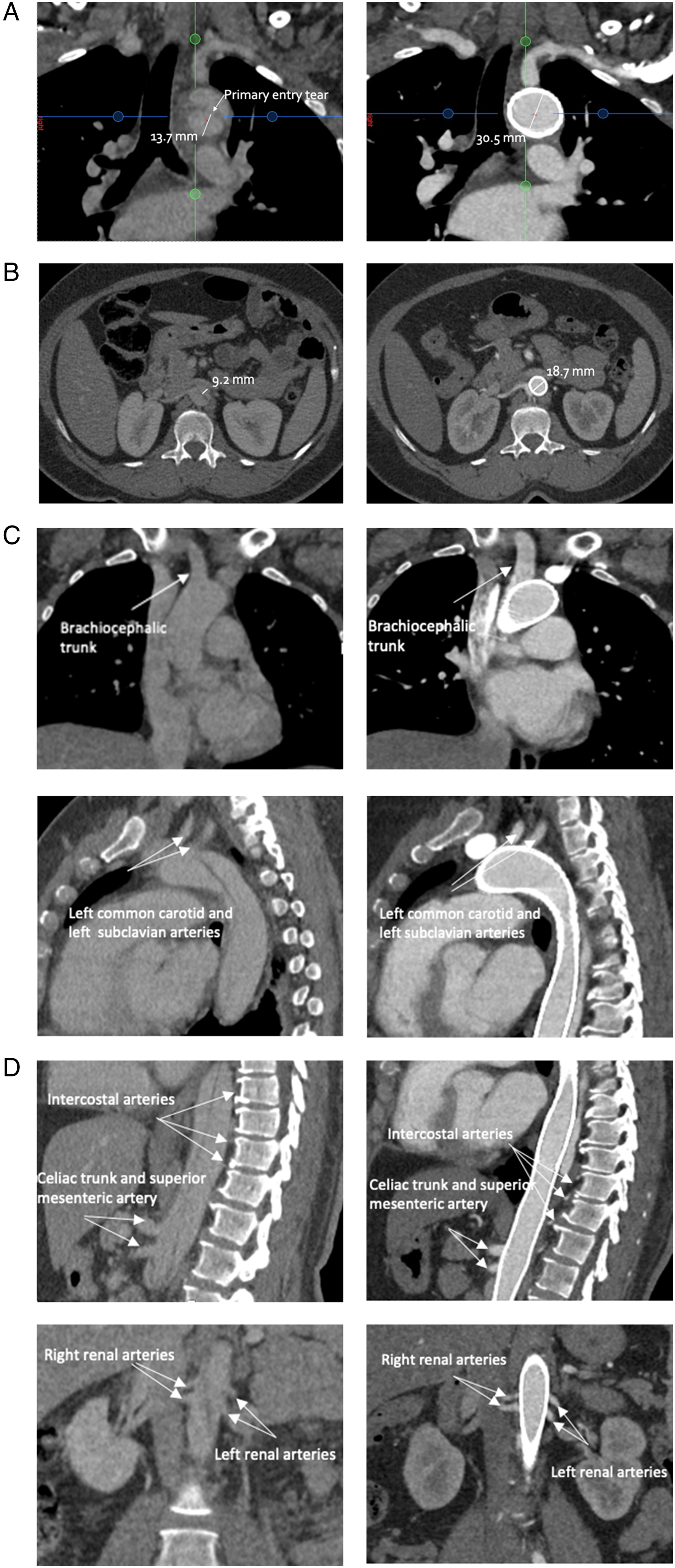
Discussion
The use of the multilayer stent in aortic dissection has already been documented elsewhere, mostly in chronic dissection with encouraging results, leading to recommendations by clinical experts to consider aortic dissection as an indication for this multilayer stent.8,10,11 As a result, a clinical investigation for use in non-acute aortic dissection has been initiated (NCT03033771).
This case report represents one of the first described cases of the treatment of acute type B dissection using a multilayer stent. In such an acute phase, the stent reopened the true lumen, reapproximating the mobile dissection flap onto the aortic wall, thereby closing the proximal entry tear and recentralizing the flow in the true lumen.
In our case the use of a multilayer stent offered several advantages.
First, the extent of the dissection necessitated to treat the entire aorta including coverage of vital branches such as both carotid arteries. The multilayer stent exhibits a radial force suitable to ensure approximation of the dissection flap to the aortic wall and true lumen reopening. Yet coverage of native side branches does not lead to occlusion as per the open-mesh design which allows to maintain physiological blood flow to aortic branches.12,13 Since its first documented use in aortic dissection, 14 short-term results of the use of the multilayer stents in thoracic dissections in studies show no association with paraplegia or visceral ischemia.11,15 In our case all side branches remained patent at 1-year follow-up.
Second, the patient presented at a hospital very far from the nearest vascular center. The multilayer stent provided a safe, simple endovascular treatment option in this setting. The procedure time in our case was just over an hour. This is much shorter than those related to stent grafts. 16 The shorter procedure time, less fluoroscopy time and less total contrast agent administered (less than 100 mL) could also make endovascular treatment of aortic dissection with the multilayer stent a reasonable alternative to stent grafts in other settings.
Finally, an additional benefit of the multilayer stent is the short hospital stay. Although this was not the primary reason to choose a multilayer stent for our patient, she left the hospital in good health after only one day.
Our paper bears several limitations. By design, it only describes our experience with a single patient. Furthermore, the follow-up duration is only 1-year. Long-term results for multilayer stents in TBAD are unavailable as of yet, though short and midterm results are promising with high technical success rates and no complications related to disease progression up to 3-year follow-up. 11 Larger studies and longer follow-up are needed to define the role of multilayer stents in the management of aortic dissections.
Conclusions
We present the first recorded case of the use of a multilayer stent for an acute type B aortic dissection with high-risk features and involvement of the visceral aorta, requiring extensive treatment. This technique may prove of great value in diminishing the risk of paraplegia or end-organ ischemia when treating the distal descending thoracic and visceral aorta with current treatment options. Long-term results of ongoing clinical studies are awaited to support multilayer stent implantation as a treatment option for aortic dissection.
Footnotes
Author’s Note
Case presented at EuroPCR on 19th May, 2022.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Intressa Vascular.