
Abstract
Background
Post-thrombotic syndrome (PTS) impacts the patient’s quality of life. Available scales to determine its severity remain controversial, therefore, it is of importance to identify new auxiliary methods for the assessment of this sequelae. Measurement of skin hardness (MSH) might be decisive in tracking PTS. The purpose of this study is to assess if the use of durometry is an objective measure to evaluate prognosis of affected limbs in patients with PTS. We compared MSH of extremities with PTS vs healthy limbs, as well as their variation after 3 months of medical treatment to evaluate if durometry can be used to find differences. We strongly believe that measuring and keeping track of skin changes specifically skin hardness can be a useful factor in the prognosis and treatment of PTS.
Methods
Prospective cohort study from January 2021 to February 2022 in patients with unilateral PTS. The MSH of the affected limb was compared to the healthy limb. A calibrated durometer was used, 4 measurements were completed at the time of diagnosis and subsequent follow-up were carried out after 3 months of treatment. The percentage of healing (in case of ulcers) and adherence to treatment was carefully monitored. The statistical program R was used.
Results
A total of 1088 durometric measurements were performed on 17 patients, and 34 limbs. The MSH in limbs with PTS was 39.09 and in the control limbs (19.8) (P = <.00001). After 3 months of treatment, the MSH in PTS varied in PTS limbs (39.09 to 30.4) (P = <.000012). Adherence to treatment was 70.5%.
Conclusions
MSH varied between healthy limbs and the ones with PTS, before and after treatment. Durometry might represent a method for assessing skin changes in patients with PTS.
Keywords
Introduction
Post-thrombotic syndrome (PTS) is the most common complication of deep vein thrombosis (DVT), ranging from 20% to 50% of patients. It is characterized by a variety of symptoms and signs such as pain, heaviness, edema, induration and hyperpigmentation of the skin, and in severe cases is characterized by the presence of ulcers.1,2 The classifications most commonly used for diagnosis and monitoring of PTS are Villalta and CEAP, which include signs and symptoms to establish their severity.3,4 Although the standardization of these scales have been recommended in order to unify concepts in PTS, limitations in their sensitivity and specificity have been brought up because the overlap of symptomatology in other pathologies and symptoms not included in the scale may go unnoticed. 5
The durometer is a portable device with a scale of 0 to 100 Units set by the manufacturer, 6 invented in 1920 by metallurgist Albert Shore 7 used as an international standardized measure to determine the surface hardness of materials such as: plastics, rubber and non-metallic materials. 8 It has been used in several medical scenarios to measure skin hardness, for example: in scleroderma,9-11 lipodermatoesclerosis,12-14 venous ulcers 15 and to measure tissues in different types of pathologies.14,16-22 Training for researchers takes approximately 15 minutes making it easy to use and an excellent option for skin induration evaluation in PTS. So far, no scales have been developed to determine the severity of the signs of PTS such as edema or skin hardness. Therefore, in this study Measurement of skin hardness (MSH) will be used to assess PTS by comparing MSH of affected limbs vs healthy limbs, as well as its significant changes after 3 months of medical treatment and the association of MSH with some clinical variables like, ulcer healing as well as changes occurring in these after a 3-month treatment (considering treatment adherence).
Methods
A prospective cohort study was conducted from January 2021 to February 2022, at the Dr. Valentín Gómez Farías Regional Hospital of the ISSSTE, Zapopan, Jalisco. Inclusion criteria: indistinct sex and gender, >18 years old, unilateral PTS (Villalta score of more than 5 points or CEAP greater than or equal to 4 at 3 months after DVT diagnosis according to SVS guidelines PTS definition), total body mass index > 18 kg/m2 and < 30 kg/m2. Exclusion criteria: peripheral arterial disease (ankle-brachial index ABI <0.9 o previously diagnosed), history of recurrent DVT, history of bilateral DVT, patients that have already used compression at the time of the start of the study, CEAP stages 1 to 3, associated rheumatologic disease, lymphedema or terminal diseases. Demographic variables (sex, age, comorbidities) as well as Villalta score and CEAP were collected.
To obtain the MSH values, a REX GAUGE™ durometer was used (model 00, 1250 Bush Parkway Buffalo Grove, Il 60089, REX GAUGE COMPANY, INC) Figure 1. MSH was performed with the patient in dorsal decubitus, with the meter located at “0”, the durometer was positioned with an angle of 90° at the peri malleolar level, making 4 measurements in the following sites: 10 cm above the internal malleolus and then 25 cm from the same starting point over the same delimited area. In patients with active ulcers, the measurement was taken in the center of the ulcer. In the healthy contralateral leg, measurements were taken using the same technique Figure 2. Excluding measurements made from the bone prominences or when the patient tensed the muscle, for more exact values. REX GAUGE™ durometer, model 00 used in this study. The durometer was positioned with an angle of 90° at the peri malleolar level to get the Measurement of skin hardness.

Obtaining at least 8 different measurements in affected limb and 8 in the healthy one. This process was repeated twice by 2 different blinded researchers. Mean and standard deviation (SD) of measurements were calculated to assign a single number of MSH to each limb and it was used for comparative statistics. Once the measurements were taken, the physician office evaluation continued as usual, and the measurement results were not taken into consideration when selecting the type of treatment for each patient. The treatment consisted of use of compression stockings of 30-40 mmHg daily up to the calf. In patients with ulcers, TIME 23 (Tissue, infection/inflammation, moisture balance and edge of wound) approach for topical ulcer treatment was implemented for management as well as pentoxifylline. In addition, each patient was given a brochure with basic venous hygiene measures to persuade adherence to treatment. 24
After 3 months of treatment, the patient attended a control consult. MSH was performed again, and the Villalta Score and CEAP were determined. In addition, we conducted a test focused on detecting adherence to the use of compression stockings, based on the study of Vein Act Program. 25 The patients who admitted not using the compression stockings, underwent further questioning to evaluate non-adherence. 26 Additionally, it was asked whether they used the prescribed stockings as indicated. In patients with PTS CEAP C6, the healing time of the ulcer was measured by comparing the area in square centimeters (cm2) to the first measure obtained in their first consult and 3 months later. Measures of central tendency were used for demographic data, Student’s T test was used to compare MSH averages between the limb with PTS and the healthy limb, as well as with the values obtained after 3 months of treatment. The intraclass correlation coefficient (ICC) test was used to measure variations in inter and intra observer measurements. Finally, with the Spearman test, a correlation was made between the results of the MSH, Villalta score and square area of the ulcer (both at the beginning of the protocol and at 3 months). The statistical program R was used.
This protocol was carried out in accordance with the Regulations of the General Health Law, that specifically involve ethical aspects of human research (article 23) and the approval of the Research and Ethics Committee of the Dr. Valentín Gómez Farias Hospital with the registration number: ISSSTE/CEI/508/2021. All patients signed written informed consent.
Results
Demographics.
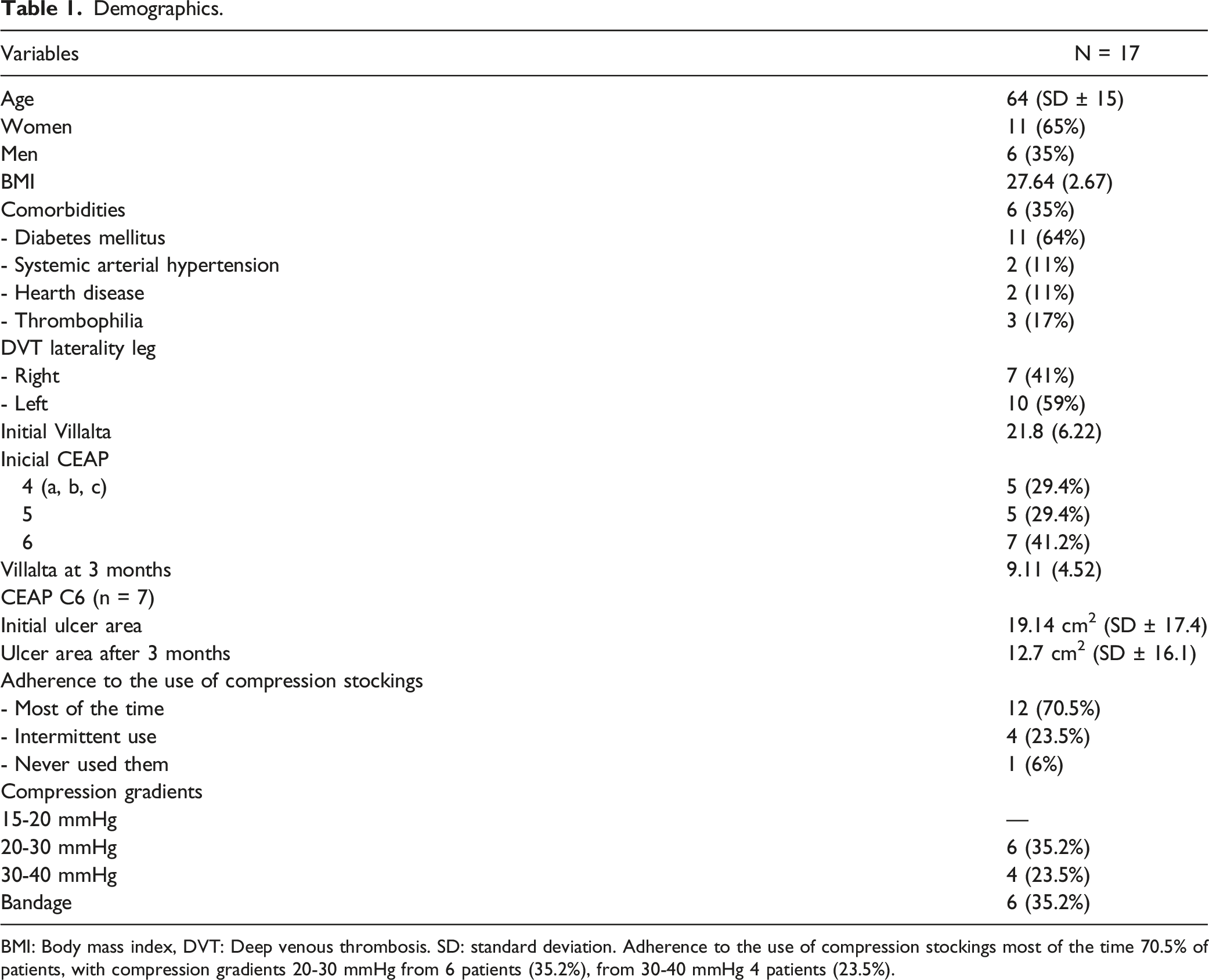
BMI: Body mass index, DVT: Deep venous thrombosis. SD: standard deviation. Adherence to the use of compression stockings most of the time 70.5% of patients, with compression gradients 20-30 mmHg from 6 patients (35.2%), from 30-40 mmHg 4 patients (23.5%).
Results of durometry measurements

PTS: post-thrombotic syndrome; MSH: Measurement of skin hardness.
An adherence questionnaire answered by the patients reported; use of compression stockings most of the time by 70.5% of patients, intermittent use 23.5%, never used 6%. Compression gradients 20-30 mmHg from 6 patients (35.2%), and 30-40 mmHg from 4 patients (23.5%). At 3 months the Villalta scale was 9 points on average (SD 4.5) with severity decrease compared to the initial scale, CEAP at 3 months: 1) stage 4: 7 patients (41.3%), 2) CEAP 5: 4 patients (23.5%) and 3) CEAP 6: with 6 patients (35.2%) with the ulcer area calculated being at 19.14 cm2 (SD 17.4) and 12.7 cm2 at 3 months (SD 16.1) Figure 3. Overall, E1 (evaluator 1) obtained an average of 39.54 units of limb hardness with PTS at the peri malleolar level with a range of 25 to 55.75, and a SD of 8.3. While E2 (evaluator 2) scored an average of 38.64 units with a range of 20 to 54 with a SD of 8.7. With no statistically significant difference (P = .76); E1 obtained an average of 19.92 units of hardness in the control limb at the peri malleolar level with a range of 8 to 27, and a SD of 4.81; while E2 obtained an average of 19.8 units of hardness with a range of 8 to 26.5 with a SD 6.4. With no statistically significant difference (P = .95). The evaluators obtained a ICC of .8325 for limbs with PTS and .8424 for contralateral limb. At 3 months of conservative management, E1 obtained an average of 30.9 units of limb hardness with PTS at the peri malleolar level with a range of 18.75 to 48.75, and a SD of 6.82; while E2 scored an average of 30 units with a range of 19 to 41.75 with a SD of 7.56. With no statistically significant difference (P = .71); E1obtained an average of 19.63 units of hardness in the control limb at the peri malleolar level with a range of 9 to 26.5, and a SD of 4.89; while E2 obtained an average of 19.32 units of hardness with a range of 5.75 to 29.25 with a SD of 6.14. There was no statistically significant difference (P = .87). The evaluators obtained an ICC of .86 for limbs with PTS and .84 for contralateral limbs. Dispersion graphics of the correlation between the size of the ulcer (mm2) and the MSH at the initial and after 3 months of treatment. MSH: Measurement of skin hardness.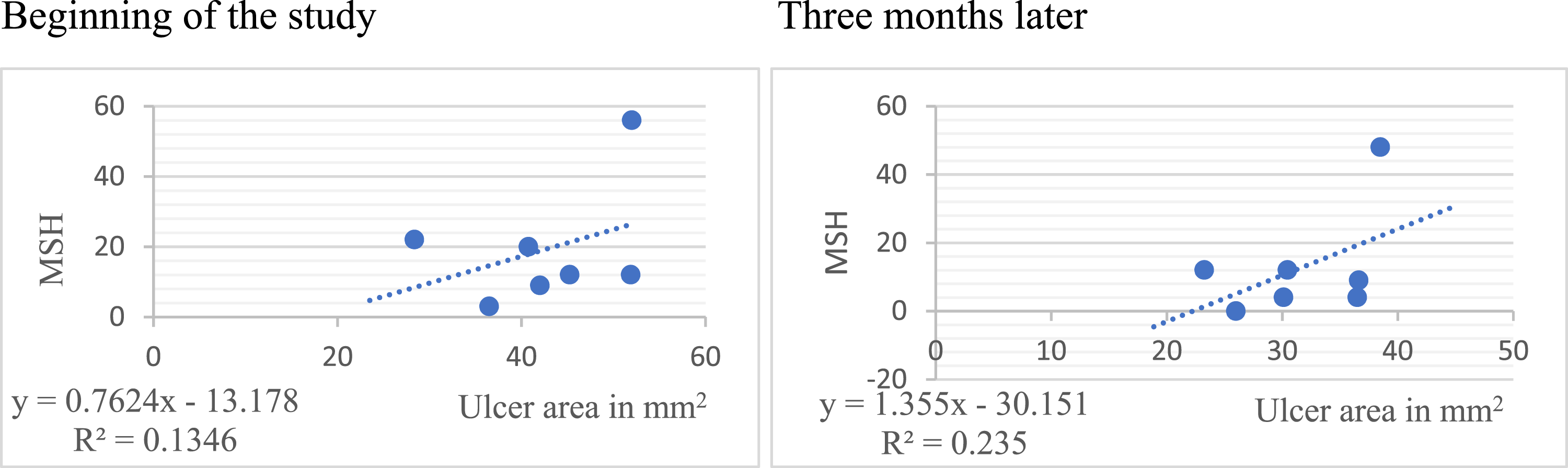
Finally, correlation between the size of the ulcer (mm2) in CEAP 6 subgroup and the MSH at the initial and after 3 months of treatment are summarized in Figure 3, and correlation of the MSH with the initial Villalta scale and after 3 months of treatment in Figure 4 (correlation of .66 and .6, respectively). Correlation of the peri malleolar MSH with the initial Villalta scale and after 3 months of treatment. MSH: Measurement of skin hardness.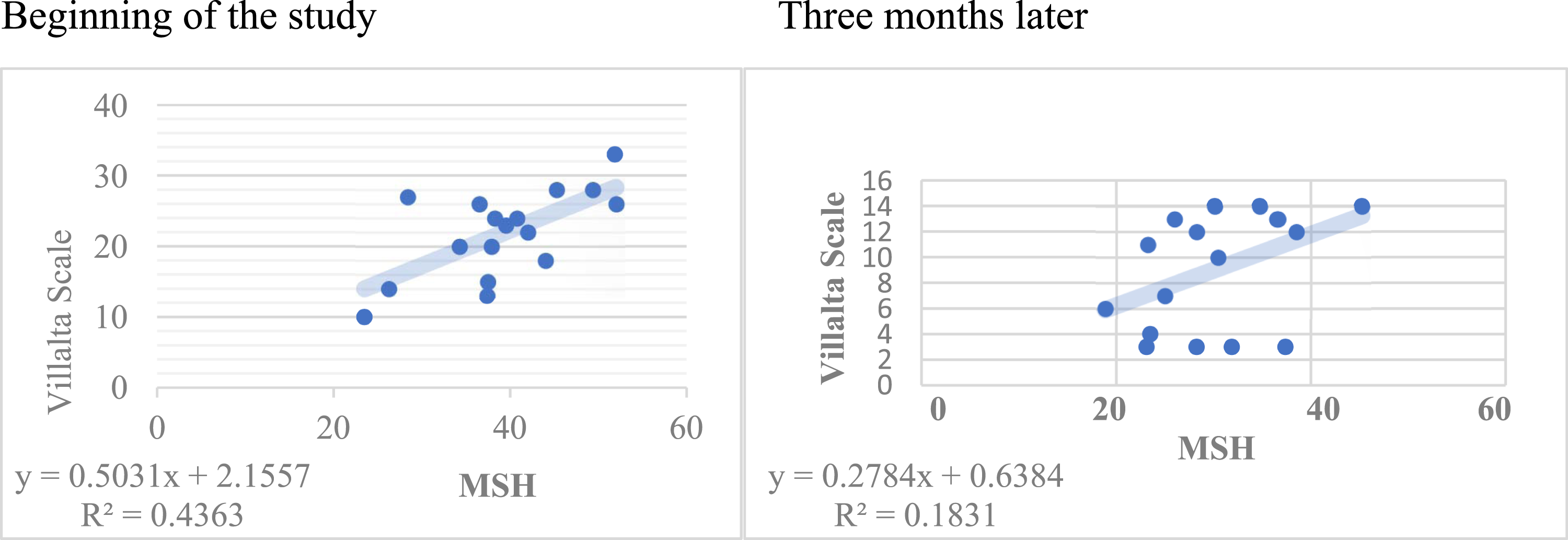
Discussion
Thrombo-embolic disease is a global public health problem; in Mexico the exact incidence and prevalence is unknown. Approximately 50% of patients with DVT without adequate follow-up and treatment develop PTS over time with important dermatological changes such as lipodermatosclerosis or venous ulcers which impact the patient’s quality of life. These complications lead to increase in hospital stay due to inadequate follow up and treatment which in turn increase work absence and medical disability as well as cost of healthcare services. Therefore, early diagnosis, which we intend with the implementation of durometry, effective intervention and treatment is of great importance; with which the patient and the healthcare institutions would benefit.
Skin hardness present in lipodermatosclerosis has prognostic significance, so it is very important to have objects that measure this alteration. 15 The durometer has been used in patients with lipodermatosclerosis as well as venous ulcers to determine skin hardness as a method of diagnosis. It is easy-to-use, economic, non-invasive tool compared to other diagnostic methods. Studies suggested that the durometer could be an objective measure and a prognostic factor in terms of the healing of venous ulcers and an elevated MSH score may be linked to a poor prognosis of ulcer healing. 8 The durometer is considered a diagnostic method along with MSH on a linear scale, in patients with the same pathology and with the same degree of induration. 6 It is currently used as a standard non-invasive tool to measure skin hardness in patients with systemic sclerosis.6,10
In the analysis carried out in this study, skin hardness had a statistically significant difference over the area of the lesion in the limb with PTS compared to its contralateral limb, which varied 3 months after the conservative treatment was performed. Adherence to treatment was assessed with a questionnaire in which more than 70% used compressive therapy most of the time, impacting the results obtained. Decrease in the square area of ulcerative lesions as well as a decrease in severity on the Villalta scale and a decrease in severity in the classification of CEAP. There was a high ICC between evaluators when comparing the MSH performed.
Limitations of our study: first and most important is the limited sample size; second, COVID pandemic limited the number of consultations; and third, the lack of unified treatment since it could interfere with the results obtained.The most positive outcome is that this study can open paths to carry out more complementary studies on durometry in PTS, with measurements being taken at different times, under different therapeutic schemes to reach a future validation of its sensitivity and specificity with a larger sample size and with multicenter studies. Considering each patient as a unit of analysis correlated with the clinical context.
Durometry is useful in the assessment of MSH with adequate correlation and agreement between evaluators for patients with PTS in advanced stages compared to healthy skin of contralateral extremity at the time of consultation and 3 months after treatment, correlating with the Villalta scale with P statistically significant. However, these results can be further supported through more studies with a larger sample and analyzing the effects of the therapeutic scheme over time.
Conclusions
Findings in this study strongly suggest that durometry may be a feasible option in stratification for both diagnostic and follow-up protocol for the approach in PTS. MSH varied between healthy limbs and limbs with PTS, as well as after receiving treatment. More studies with larger sample numbers are needed as it could identify and predict those patients at risk of pre-ulcerative lesions. Thus, determining a form of evaluation with a great cost-benefit. Durometer use as an objective instrument in the MSH assessment in PTS with intra-evaluator and Inter-evaluator correlation and concordance is highlighted, both for the control group and in the affected group. The durometer could be considered as a clinical tool for future clinical trials 9 and which could be extrapolated to the vascular field, in order to demonstrate if it is an objective metric tool for evaluation in PTS and if it is reproducible.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
This study was presented and won third place at the of the Mexican Society of Angiology, Vascular and Endovascular Surgery, AC. Cancun, Quintana Roo, Mexico. November 1-5, 2022.
Ethical Approval
This study has been approved by the Research and Ethics Committee of the Dr. Valentín Gómez Farias hospital with the registration number: ISSSTE/CEI/508/2021.
Informed Consent
All patients signed written informed consent.