
Abstract
Background
Bilateral limb occlusion after endovascular repair of abdominal aortic aneurysms (EVAR) is an uncommon entity. The relationship between graft kinking and unilateral limb occlusion is widely described in the literature. Our aim is to report a case of complete endograft thrombosis due to bilateral limb kinking secondary to aneurysm sac shrinkage, treated by endovascular means.
Case report
A 67 year-old male with history of EVAR with an Incraft® endograft (Cordis, Bridgewater, NJ, USA) four years before, presented at the emergency department with disabling claudication of the right lower extremity and a better tolerated 10-month left extremity claudication. Complete endograft thrombosis with bilateral limb kinking and a remarkable reduction of the aneurysm sac was observed in the computed tomography angiography. An endovascular repair was performed, through bilateral open femoral access and with angiographic control through percutaneous left brachial access. Bilateral recanalization was achieved and the endograft was re-lined with two 10x150 mm Viabahn (WL Gore & Ass., Flagstaff, AZ, USA). Both sides were extended with a 11 × 50 mm Viabahn (WL Gore & Ass., Flagstaff, AZ, USA). The final angiographic control showed bilateral patency with no residual stenosis and the patient recovered distal pulses. Follow-up showed complete patency and no complications at 17 months.
Conclusions
Bilateral limb occlusion is a rare complication with technically challenging treatment options. Aneurysm sac shrinkage can affect the endograft configuration, leading to limb distortion and occasionally to bilateral limb occlusion after EVAR. Special attention should be put on imaging follow-up to detect these complications before occlusion occurs.
Background
Endograft limb occlusion is a potential complication of endovascular aneurysm repair (EVAR). It represents a major cause of secondary intervention and the third most common cause for readmission. 1 Its incidence rates range from 0% to 7%.2,3 Compared with unilateral limb occlusion, bilateral limb occlusion is relatively uncommon, with a reported incidence ranging from 0% to .6%.4,5
Many endograft limb occlusions can be attributed to mechanical complications, especially endograft kinking, which is thought to be the predominant underlying cause of occluded limbs.6,7 Development of kinks can be related to iliac tortuosity, endograft twisting, compression by the thrombus within the excluded aneurysm and changes in aneurysm morphology after sac shrinkage in a successful EVAR.8,9
Although many mechanisms have been proposed concerning unilateral limb occlusion, scarce data are available regarding bilateral endograft limb occlusions. 10 We present a case of bilateral limb occlusion after EVAR, treated by endovascular means.
Case Presentation
A 67 year old male, former smoker, with history of hypertension and dyslipidemia, presented at the emergency department of our institution with sudden disabling intermittent claudication on the right leg and a better tolerated 10-month left limb claudication. Physical examination showed complete absence of pulses in both lower limbs with maintained mobility and no sensitive impairment.
He had a prior EVAR with an Incraft® endograft (Cordis, Bridgewater, NJ, USA) 4 years before, for a 54 mm abdominal aortic aneurysm (AAA). (Figure 1) The proximal diameter of the main body was 30 mm with 11 mm gates. Both limbs had been extended with 20 × 120 limb grafts and sealed in common iliac arteries. The post-EVAR follow-up protocol included a 30-day and 12-month contrast-enhanced computed tomography (CTA), which confirmed limb patency without mechanical kink as showed in Figure 1C and 1D. Also a Duplex ultrasound (DUS) was performed at 6-month and yearly after the first year CTA control. A 5-year CTA was scheduled according to our institution’s surveillance protocol, but finally was not performed as the complication described in this case report arose first. (A) Pre-EVAR computed tomography angiography. (B) EVAR intraoperative final angiography. C and D: 1-month follow-up computed tomography angiography.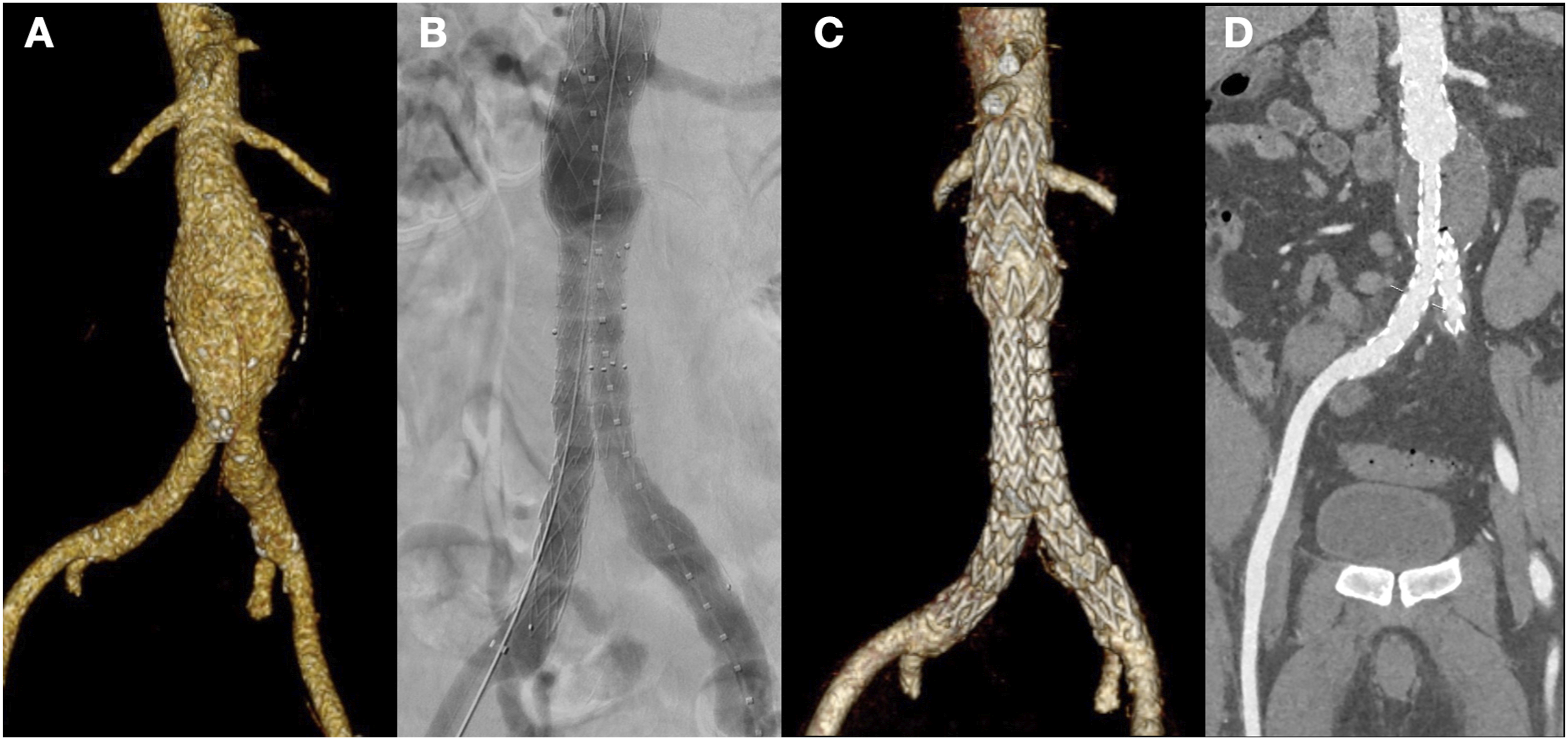
Immediately upon admission, a CTA was performed and revealed a bilateral limb occlusion with thrombosis that extended to the main body of the endograft; renal and visceral arteries were unaffected. There was a remarkable decrease in the size of the aneurysmal sac (21 mm) and both iliac extensions were kinked in the overlap area with the main body limbs. (Figure 2) Computed tomography angiography: complete endograft occlusion with aneurysm sac shrinkage.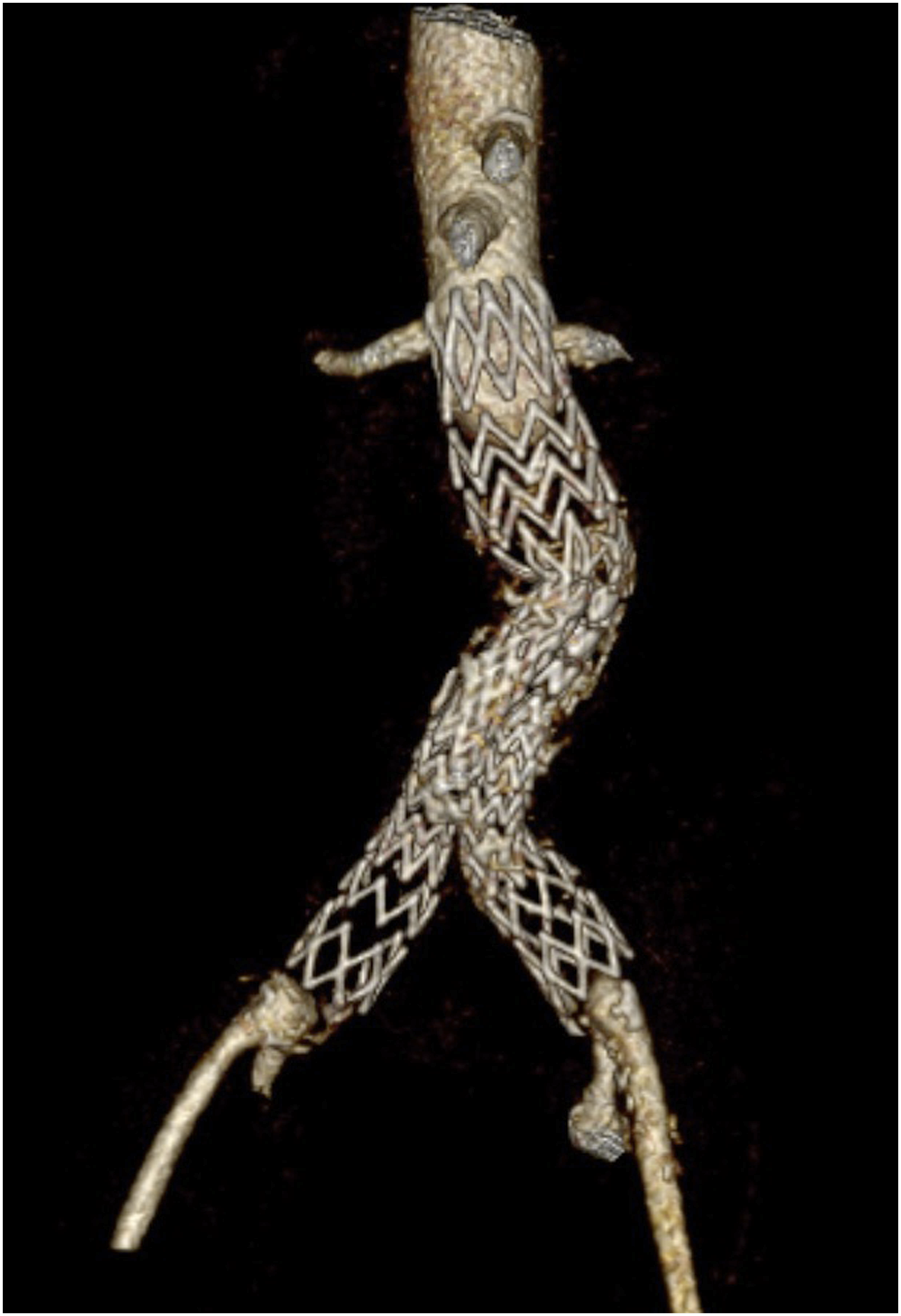
Under general anesthesia, an open bilateral femoral approach was performed, controlling the femoral bifurcation to prevent distal embolization. In addition, a percutaneous left brachial access was obtained and an angiographic pigtail catheter was advanced to the visceral aorta. The initial angiography confirmed the CTA findings. (Figure 3A) Intraoperative images. A: Initial angiography. B: Results after recanalization.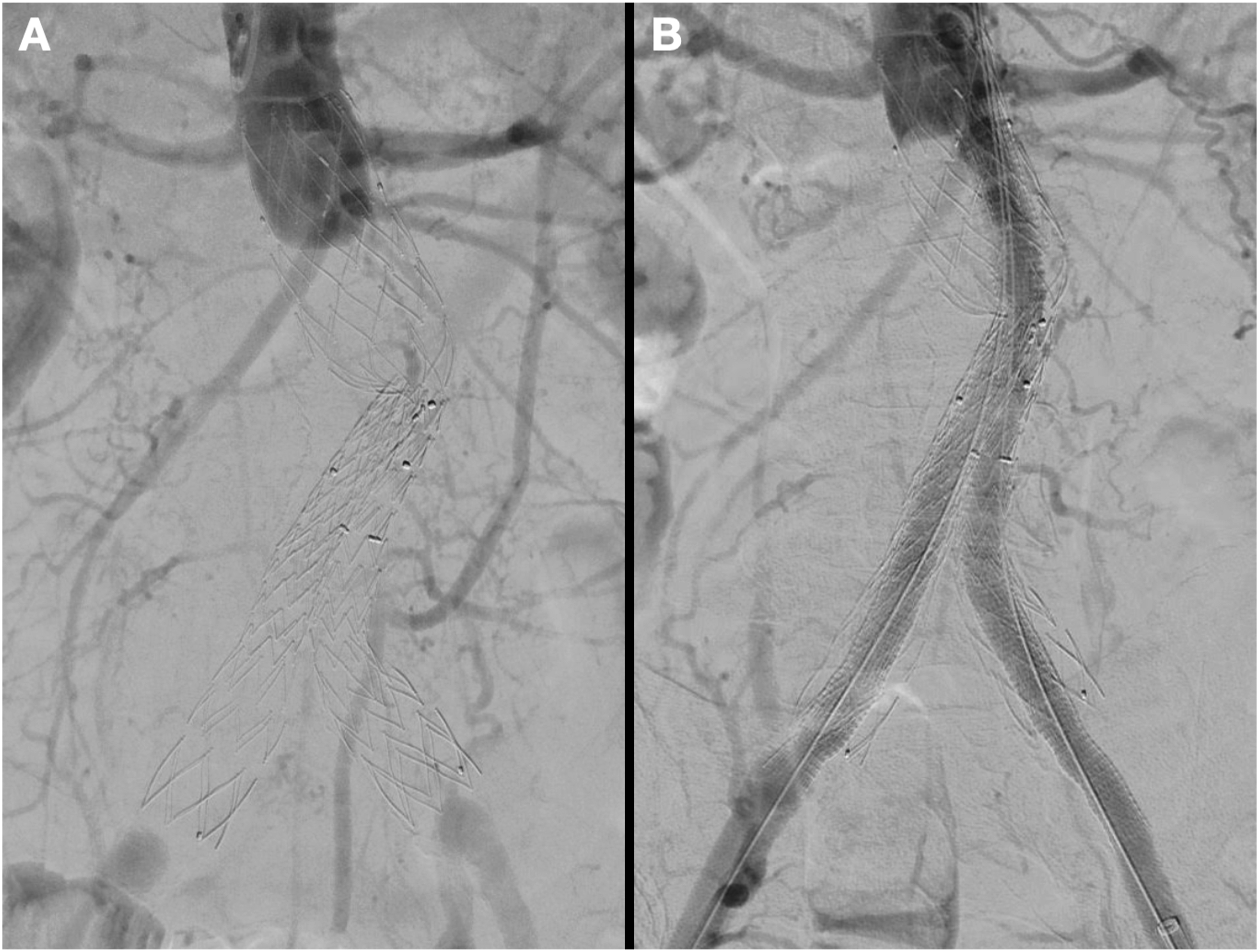
Bilateral recanalization with a 0,035” straight tip hydrophilic Terumo® guidewire (Terumo Interventional Systems, Inc., Somerset, NJ, USA) was obtained. The guidewires were exchanged for Back-Up Meier® guidewires (Boston Scientific, Marlborough, MA, USA) and a 12F DrySeal® Flex Introducer Sheath (WL Gore & Ass., Flagstaff, AZ, USA) was placed through both femoral accesses. A 10 × 150 mm Viabahn® (WL Gore & Ass, Flagstaff, AZ, USA) was advanced through each access and both were simultaneously deployed distal to the ostium of the lowest renal artery, performing a kissing stent technique. Both sides were extended with a 11 × 50 mm Viabahn® (WL Gore & Ass., Flagstaff, AZ, USA) into the previous endograft limbs.
The final angiographic control showed bilateral patency with resolution of the previous kinking, although an unintentional occlusion of the left hypogastric artery was detected.(Figure 3B) In the immediate postoperative period the patient recovered bilateral distal pulses and he was discharged home five days later with no perioperative complications and under antiplatelet monotherapy with salicylates.
After 17-months of follow-up, both limbs remain patent and the patient maintains distal pulses with complete resolution of claudication symptoms. (Figure 4) No buttock claudication or other clinical manifestations arose related to the occlusion of the left hypogastric artery. Follow-up computed tomography angiography: endograft patency with no kinking signs.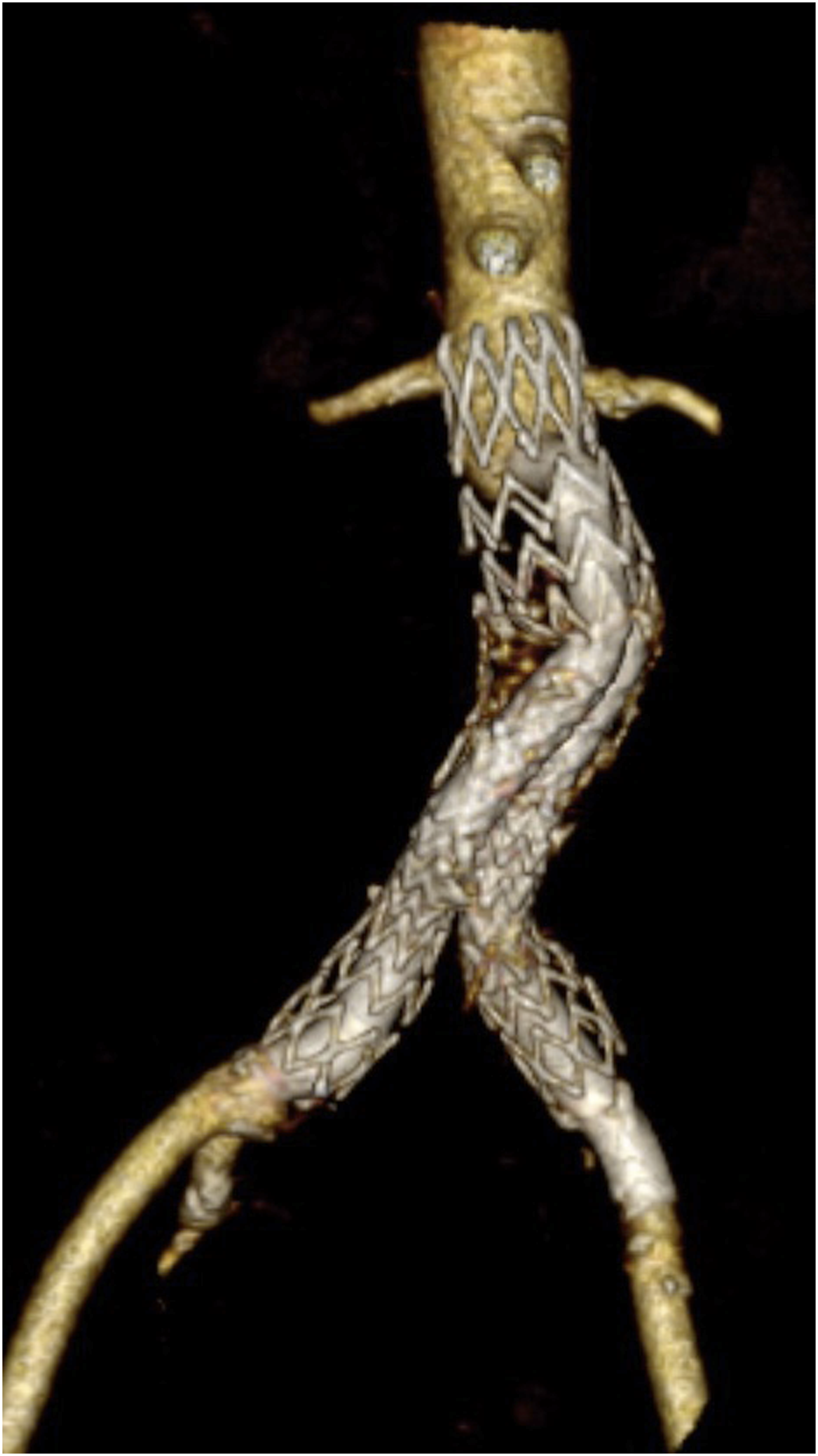
Discussion
EVAR has become the first line treatment in many patients with anatomically-suitable infrarenal abdominal aortic aneurysms. Limb occlusion shows incidence rates from 0% to 7%,2,3 causing a non-negligible number of reinterventions. However, this rate can be higher taking into account that asymptomatic occlusions may be missed. More specifically, bilateral occlusion is a rare complication with a reported incidence ranging from 0% to .6%.4,5 Limb occlusion manifests with acute ischemia (present in a third of patients in published series 3 ), rest pain, paresthesia, functional impairment, non-healing lesions or intermittent claudication. Some patients can remain asymptomatic, with a decreased femoral pulse as the sole finding. 11 These symptoms can appear both suddenly and insidiously.
Kinking is reported to be one of the main causes of limb occlusion, followed by extension into the external iliac artery. Coelho et al. report a graft kink rate as the underlying mechanism of 42.8% of all limb occlusions in their series (that include 55 articles and 27 509 patients). This study postulates that the predominant risk factors for limb occlusion are limb kinking, iliac tortuosity, extension into the external iliac artery, narrowing of the distal aorta, intra-graft mural thrombus, stent oversizing and the type of stent-graft. Aneurysm shrinkage has been related to limb distortions such as kinking, 7 although according to Fransen et al., late kinking appears closely associated with graft migration. 12 In the case we are reporting, kinking of both limbs can be appreciated in pre-reintervention images. (Figure 2)
It is known that old unsupported endografts and first-generation supported endografts were associated with higher rates of limb occlusion.7,13 The behavior of modern devices has also been studied. Limb grafts with Z-stents and unsupported gaps are more susceptible to kinking than helical configuration grafts. 14 On this matter, the multicenter study published by De Donato et al analyzed the long-term outcomes of low-profile endografts and reported similar results than traditional endografts, but Zenith LP® [Cook Medical, Bloomington, IN, USA] had significantly lower patency rates than Ovation® [Endologix Inc., Irvine, CA, USA] and Incraft® [Cordis, Bridgewater, NJ, USA] and was identified as an independent factor for limb-related events. These results can be explained by the Zenith LP® Z-stent design, which has been changed in the new Zenith Alpha® [Cook Medical, Bloomington, IN, USA]. 15
Additionally, the available data have shown that expanded polytetrafluoroethylene (ePTFE) grafts are less thrombogenic than polyester stent grafts. Also, small diameter limbs are described in the literature as a risk factor. 16 In this regard, Bogdanovic et al. described the endograft device type as an independent risk factor for limb occlusion; in their study, the Zenith Alpha® (Cook Medical, Bloomington, IN, USA) showed an increased risk (12.4%) of occlusion compared with the Excluder® endograft (W. L. Gore & Assoc., Flagstaff, AZ, USA) which reports a much lower occlusion rate (.7%). 17
The literature specifically addressing predisposing factors for bilateral limb occlusion as an independent entity is scarce. Moulakakis et al. published an analysis concluding that iliac artery angulation, calcification and endograft oversizing in the common iliac artery are the main mechanisms involved.10 Their group postulates that all three factors should be present in both iliac arteries to develop a bilateral limb occlusion. In our case, the preoperative CTA showed no remarkable iliac angulation or calcification. Only the right iliac limb (20 mm in diameter) was significantly oversized over the native common iliac artery (17 mm, 20,4%). No graft migration was observed in the follow-up CTA and the patient had a significant decrease of the sac diameter. We believe this sac shrinkage caused a bilateral limb distortion and kinking, facilitated by the specific Incraft® endograft (Cordis, Bridgewater, NJ, USA) configuration: the separation between the Z-stents and the narrow diameter of the gates (11 mm).
For a correct treatment of endograft limb occlusions, patient condition, severity of ischemia and surgeon preference should be taken into account in order to make a decision. There is a lack of evidence in literature for a management recommendation. Surgical thrombectomy in modular- designed grafts is not exempt of concerns regarding a potential graft damage or dislocation. Classically, the most common surgical option was an extra-anatomic revascularization with a femoro-femoral bypass for unilateral occlusions and an axillo-bifemoral bypass for bilateral limb occlusions. However extra-anatomic revascularization long-term patency has been put in question, therefore it should be reserved for patients with high surgical risk. Other open surgery options are an endograft explant with anatomic revascularization, or a thoraco-bifemoral bypass for patients with a hostile abdomen (obesity, multiple abdominal surgeries, colostomies, etc.). Endovascular treatment options include thrombus removal techniques with mechanical thrombectomy devices, as well as graft limb relining (percutaneous balloon angioplasty and stenting). Thrombolysis may be associated, since it allows patency restoration and identification of underlying limb stenosis. 7
In this case, the clinical onset of the right limb occlusion made us discard a mechanical thrombectomy and thrombolysis, choosing the relining with covered stents as our treatment strategy. Open control of both femoral bifurcations minimized the risk of embolization while the kissing stenting was taking place.
Conclusions
Bilateral limb occlusion is a rare post-EVAR complication with technically challenging treatment options. Aneurysm sac shrinkage can affect the endograft configuration, leading to limb distortion and occasionally to bilateral limb occlusion after EVAR. Special attention should be put on imaging follow-up to detect these complications before occlusion occurs. Further studies on bilateral limb occlusions are needed to confirm predictive factors and the optimal treatment strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Compliance with Ethical Standards
Our institution does not require ethical approval for reporting individual cases or case series. Written informed consent was obtained from the patient for the publication of this case report.