
Abstract
Tuberous sclerosis complex is a neurocutaneous syndrome caused by an autosomal dominant genetic disorder. This condition can lead to the expression of many vascular anomalies especially, in the pediatric population. Likewise, it has been linked with aortic aneurysm development. We report a case of a 12-year-old boy who presented a 97 × 70 mm Crawford type IV thoracoabdominal aortic aneurysm. Satisfactory open surgical repair was performed with an 18-mm multibranched dacron tube graft. Clinical and imaging findings revealed a de novo tuberous sclerosis diagnosis. The patient was discharged uneventfully during a 1-month follow-up.
Introduction
Tuberous sclerosis complex (TSC) is a neurocutaneous syndrome caused by an autosomal dominant genetic disorder. It is characterized by the classic triad of seizures, mental retardation, and facial angiofibroma development. Likewise, it has been linked with aortic aneurysm (AA) development in children.1,2 In those cases, the early surgical repair must be done to avoid the risk of rupture. Few cases of thoracoabdominal aortic aneurysms (TAAA) in the pediatric population with TSC have been described. We present the case of a 12-year-old boy who presented to the emergency department with a 97 × 70 mm symptomatic Crawford type IV TAAA. Satisfactory open surgical repair was performed with an 18-mm multibranched dacron tube graft. The patient was assessed by a multidisciplinary team based on clinical results and diagnostic images. At this point, the boy met all TSC criteria. A 1 month’s follow-up was uneventful, and symptoms resolved. This case and its final result demonstrate the need for meticulous surgical planning, multidisciplinary work, strict follow-up, and open surgical approach consideration. Written, informed consent for patient information and images to be published was provided by the legally authorized representative.
Case Presentation
A 12-year-old male was referred to the emergency department with breakthrough headaches, abdominal pain, and going through a hypertensive crisis. Upon admission, he came with an angiotomography report showing a TAAA from his referral institution. Physical examination revealed café au lait spots, hypomelanotic macules, and pulsating mass palpated at the epigastrium. His past medical history was significant for epilepsy without cognitive impairment. A new angiotomography showed a saccular TAAA compromising the superior mesenteric artery (SMA) and both renal arteries. Furthermore, it was associated with an eccentric thrombus and calcification of the aortic wall. (Figure 1) Thoracic and abdominal angiotomography. showing a saccular Crawford type IV TAAA with a maximum diameter of 9.7 cm.
The maximum anteroposterior diameter was about 97 × 70 mm with a total length of 57 mm. As an incidental finding, the image showed a hypervascular, peripheral solid focal lesion in the lower pole of the left kidney with a diameter of 28 mm. As well, revealed multiple low-density focal lesions in the kidneys cortex, vertebral body (L1), and iliac arteries. Given the high risk of rupture, urgent open surgical repair was performed. Prior detailed planning a handmade multibranched aortic graft was made. (Figure 2) The branches were anastomosed to a straight 18 mm dacron graft using a 16 × 8 mm dacron graft for the celiac trunk (CT) and SMA. For both renal arteries, a 12 × 6 mm graft was added. Handmade dacron graft with branches to the (a) right renal artery, (b) left renal artery, (c) celiac trunk, and (d) superior mesenteric artery.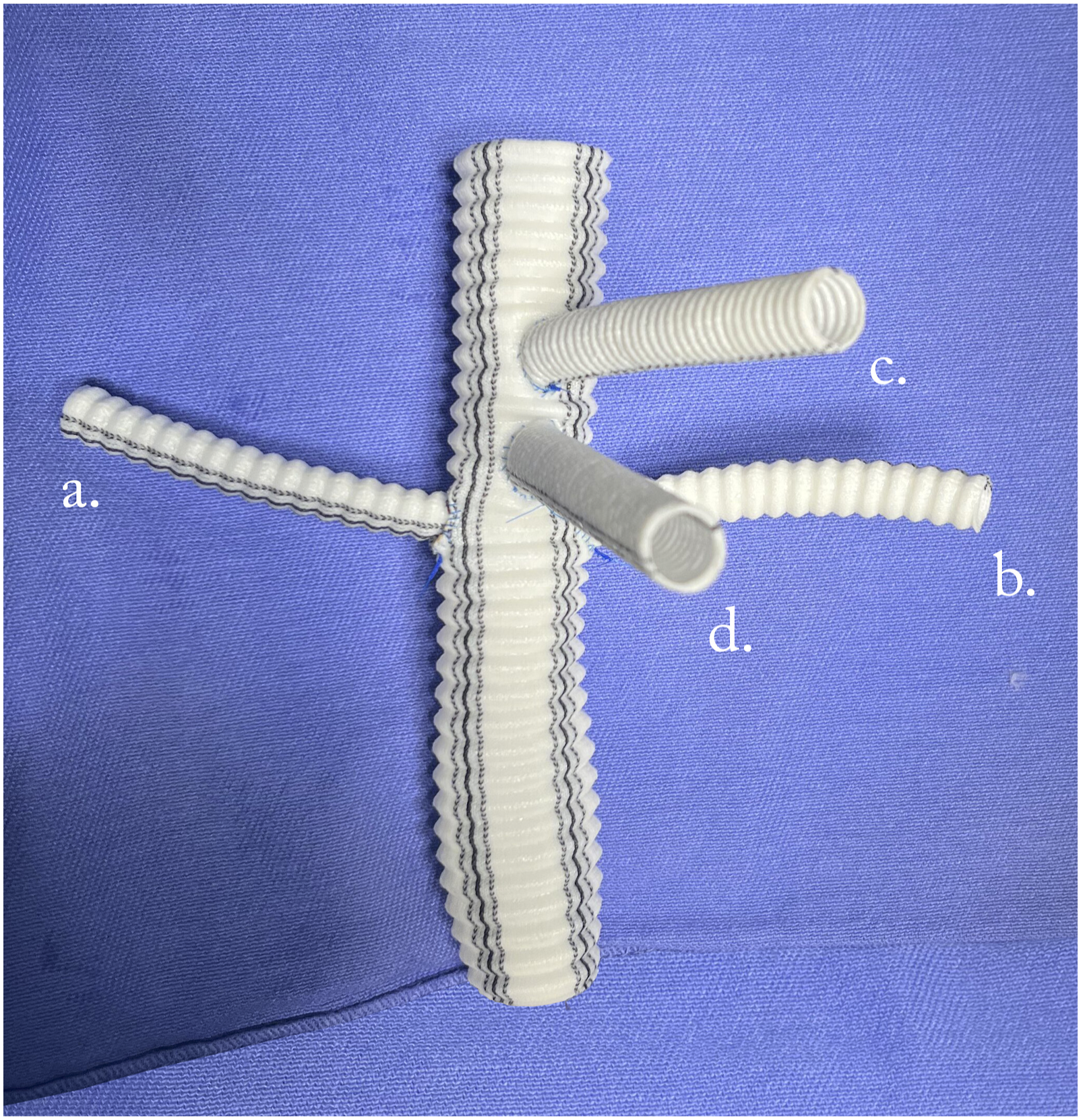
Under general anesthesia, a left thoracic-phrenic lumbotomy was performed and the aortic hiatus was identified and dissected. The abdominal aorta was dissected up to the infrarenal segment. CT, SMA, and renal arteries were dissected and repaired with vessel loops. Double proximal aortic clamping was performed and descending aorta was sectioned revealing Crawford IV thoracoabdominal aneurysm with a thrombus inside and calcified walls. (Figure 3.) The proximal segment of the terminal anastomosis was made with the pre-made 18 mm dacron graft. The CT, SMA, and renal arteries were divided and stumps were ligated. Thoracoabdominal aortic aneurysm exposure compromising CT, SMA, both renal arteries and inferior mesenteric artery.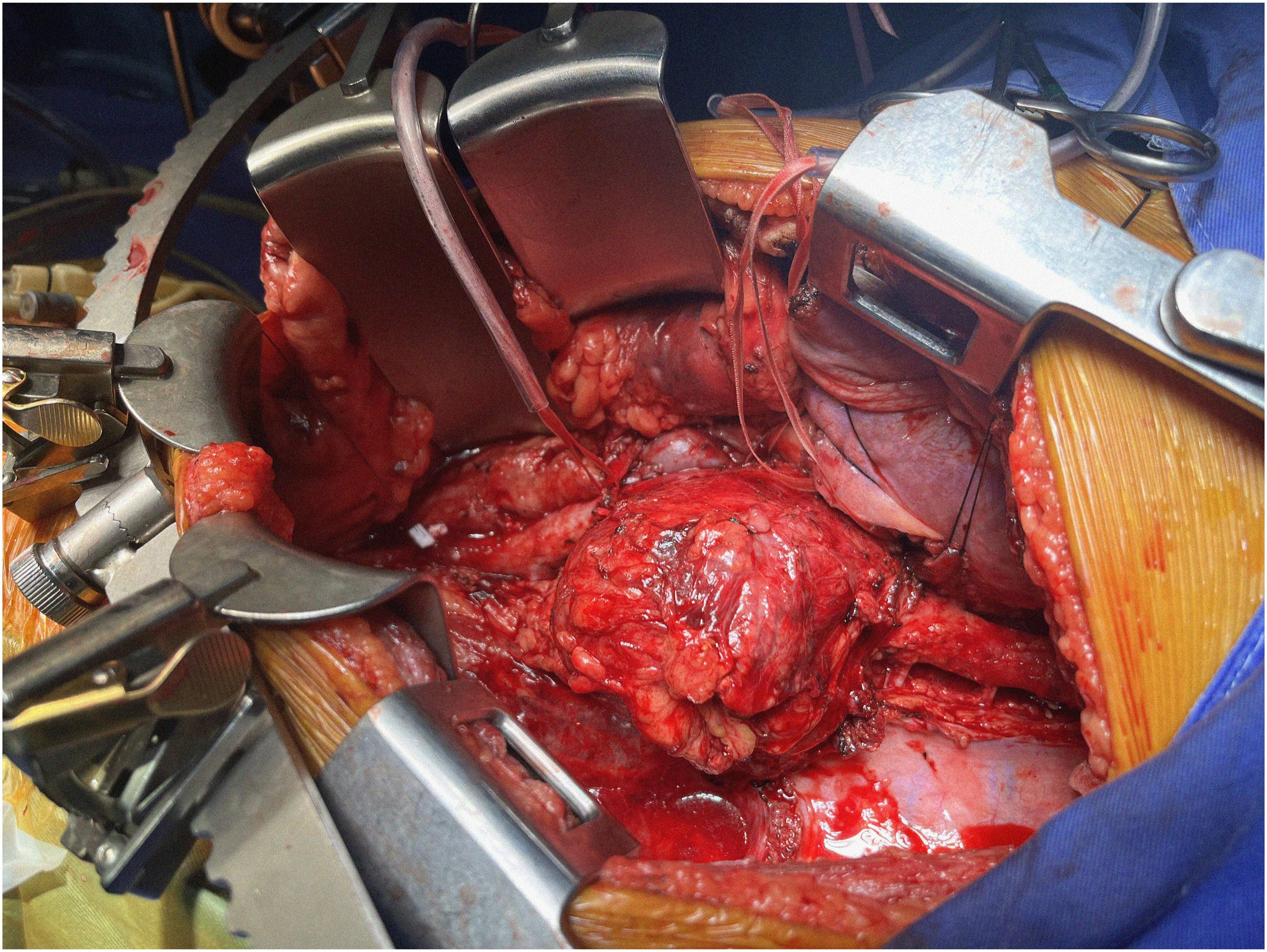
Each branch was anastomosed to the graft sequentially in an end-to-end fashion. The distal infrarenal aortic anastomosis was completed and distal body circulation was restored. Subsequently, AMS and CT end-to-end anastomosis were performed. The branches were unclamped to restore visceral perfusion. (Figure 4.) The patient was admitted to the pediatric intensive care unit. During the postoperative, TSC was suspected given the clinical and imaging findings. The clinical diagnosis was confirmed. Interdisciplinary care was crucial to identify the TAAA etiology. Multibranched graft fully anastomosed and declamped. (a) Proximal aortic, (b) celiac trunk and (c) superior mesenteric artery anastomosis. The renal vein keeps anterior to the graft.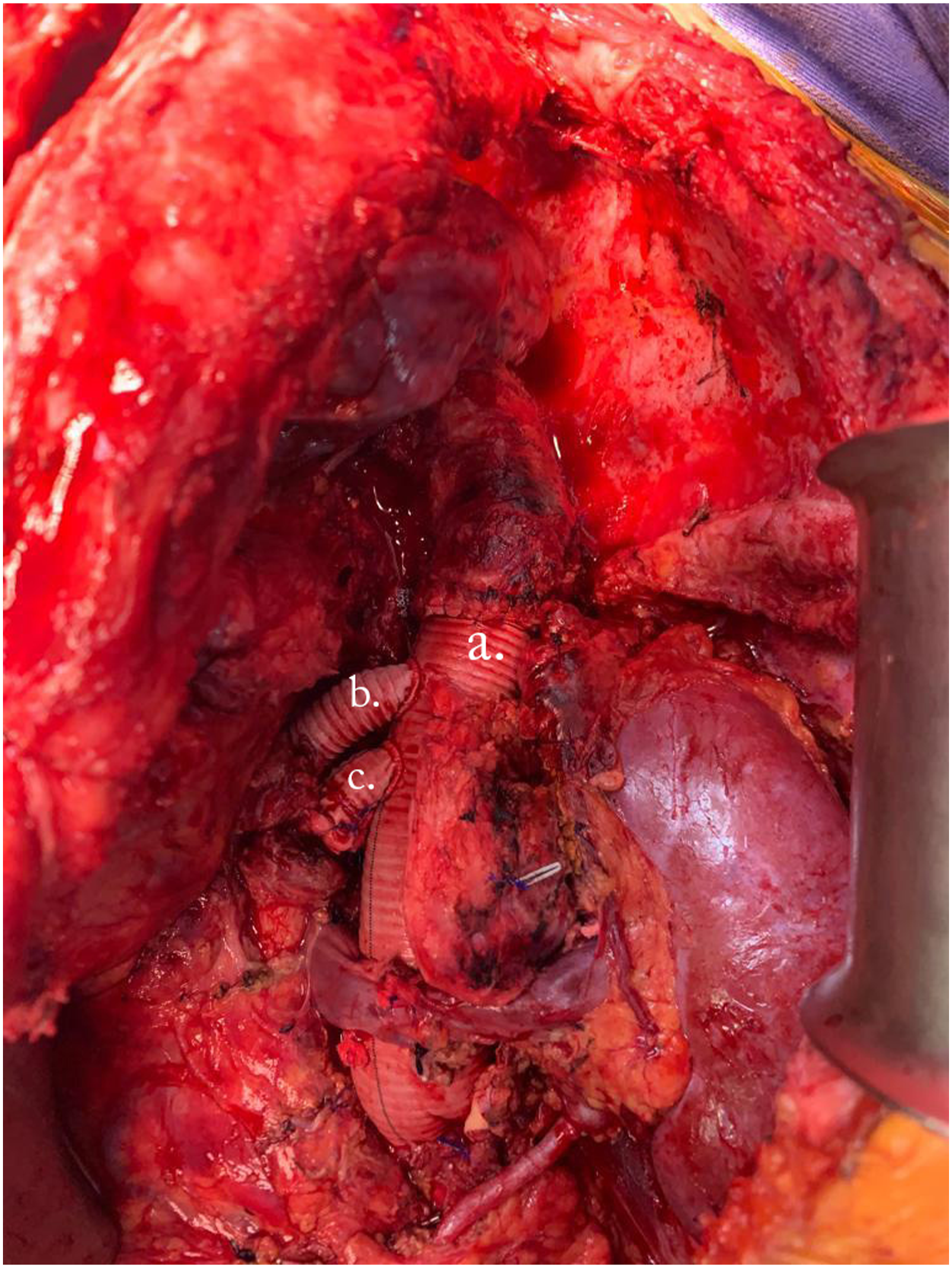
The diagnostic suspicion of tuberous sclerosis was given by the multisystemic findings such as renal angiomyolipomas, cortical tubers, giant cell astrocytoma, epilepsy, café au lait spots, hypomelanotic macules, and identified thoracoabdominal aneurysm. The histological revealed fibrosis, chronic inflammatory infiltrate, tunica media neovascularization, and loss of muscle fibers. At the 1-month follow-up, the patient was assessed uneventfully.
Discussion
TSC is an autosomal dominant disorder with multisystem involvement. It was initially described by Bourneville in 1880 as a triad characterized by seizures, mental retardation, and facial sebaceous adenoma. 3 It is caused by mutations in the tumor suppressor genes TSC1 and TSC2, which code for hamartin and tuberin proteins, respectively. This mutation produces a reduced inhibition of the complex (mTor) that promotes cell growth and proliferation. 2 The association between vascular abnormalities and cardiovascular involvement has been described in these patients.
Case Reports of Thoracoabdominal Aneurysms in Pediatric Patients With Tuberous Sclerosis.
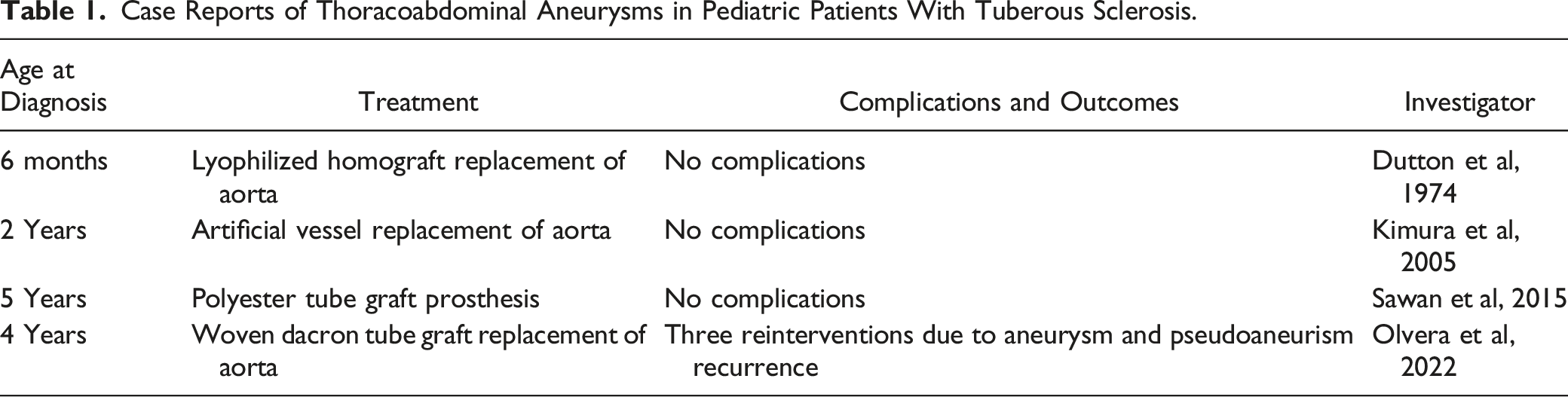
Most AA in patients with TSC occurs in the abdominal aorta and less frequently in the thoracic aorta. 10 The age of presentation is variable, however, Salerno et al showed that the age of presentation of AA was before 5 years of age, and mortality due to aneurysmal rupture was 29%.3,11 Currently, there is no consensus regarding treatment, however, surgery continues to be the best option according to each patient. 11 When a TSC related TAAA is present, surgery must be realized to avoid the risk of rupture. Frequently, this condition is diagnosed when a rupture of the aortic aneurysm is done. Early surgery correction allows better outcomes and decreases the risk of mortality.
The success of this case shows the importance of strict surgical planning and defining the preparation of the graft when all the necessary resources are not available. Multidisciplinary work allows for providing comprehensive care and is useful in the diagnosis of suspected TSC, due to the presence of vascular abnormalities and multisystem involvement. The open surgical approach may be considered for the correction of TAAA in pediatric patients if the resources exist and the surgical ability to perform it is possessed. Strict follow-up must be done in patients presenting with TAAA due to the risk of recurrence.
Supplemental Material
Supplemental Material - Open Emergency Repair of a Thoracoabdominal Aortic Aneurysm on a 12-Year-Old Boy With Tuberous Sclerosis
Supplemental Material for Open Emergency Repair of a Thoracoabdominal Aortic Aneurysm on a 12-Year-Old Boy With Tuberous Sclerosis by Julian M. Corso-Ramirez, Mariana Molina López, Paula Camila Flórez, Juan Guillermo Barrera-Carvajal, and Jaime Camacho Mackenzie in Vascular and Endovascular Surgery.
Footnotes
Acknowledgments
We would like to thank the staff of the vascular surgery service of the Fundación Cardio Infantil- LaCardio.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the ethics committee from Fundación Cardio infantil -LaCardio, Bogota, Colombia, under reference number CEIC – 0067 -2023.
Informed Consent
Written, informed consent for patient information and images to be published was provided by the legally authorized representative.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.