
Abstract
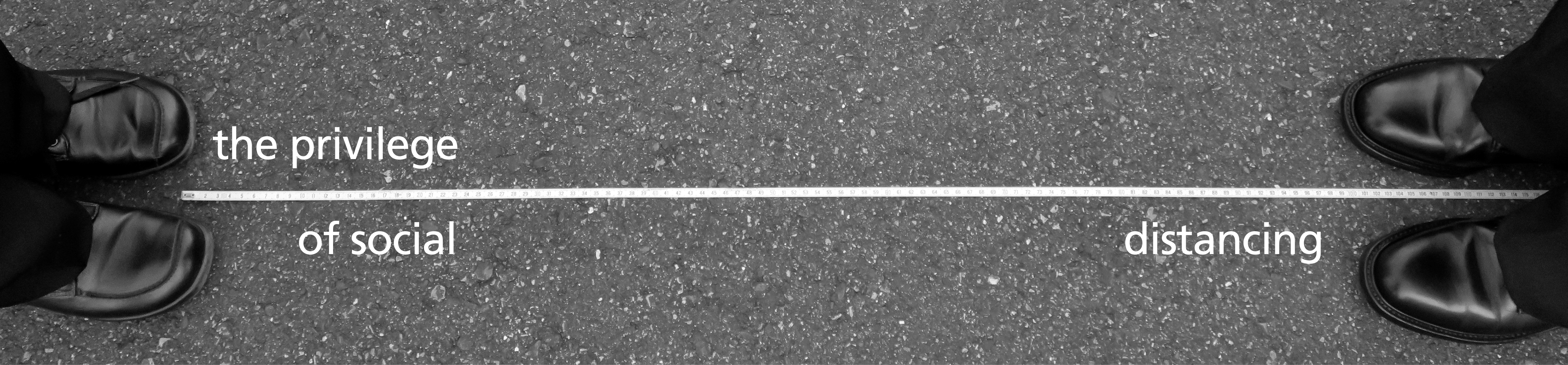
In the global pandemic, there is a group of people who are not socially distancing: the precariously employed, the workers who live paycheck to paycheck and lack the flexibility to stay home. In this article, readers are encouraged to consider the many social factors that can impede people from staying home.
Keywords
On camera in March, spring breakers in Miami discussed their decision to party despite the calls for “social distancing” or “measures taken to restrict when and where people can gather to stop or slow the spread of infectious diseases.” A young man concluded, “At the end of the day, I’m not going to let it stop me from partying.” Around the same time, another video made the social media rounds depicting people in a New York City apartment building yelling: “Flatten the curve, go home! Get the f*** inside!” at pedestrians walking below.
Perhaps because cases like that of the Miami Spring Breakers are the most visible, people admonish anyone who does not stay home as if they were all young partyers. However, what is lost in the stigmatization of all people who do not stay home is the class divide within this group of people.
There is another group of people who are not socially distancing: the precariously employed, that is to say, workers who live paycheck to paycheck and/or lack the flexibility to stay home. Historically, precarious employees have been people that the broader society already marginalized in other ways: women, immigrants, racialized groups, poor people, and those lacking access to education. To the precariously employed, staying home from work for health reasons has long been a decadent luxury. Undocumented immigrant workers, who have been formally excluded from the labor market and recently from federal pandemic support, are some of the most vulnerable workers amongst the precariously employed.
The experiences of this sub-group of precarious workers are at the center of this project. The case of undocumented immigrants does not, and is not meant to, encapsulate all of the different types of people who do precarious work in the United States. The precariously employed are a diverse and diversely marginalized sector of the workforce. However, since undocumented immigrants are formally marginalized from the mainstream labor market in the United States, this case is a well-suited one to investigate the experiences of precarious workers and the impact of precarity on health attitudes and behaviors.
In this article, I will delve into the literature on precarious employment and how its intersection with other marginalized identities restricts resources for precarious workers. I will then draw on 50 semi-structured interviews with some of the most vulnerable precarious workers in the United States: DACA and DACA-ineligible undocumented adults in order to illustrate that even before the COVID-19 pandemic, there was already a sense of unattainable decadence surrounding healthcare and that migrants turned to a “healthcare as self-care” narrative when deciding how to allot scarce health resources. I conclude by summarizing the structural reasons that make it near impossible for precarious workers to socially distance: the kind of work they do, their lack of resources, and constricted access to healthcare, and discuss how social compliance tools (like stigma) that could work on the Miami Spring Breakers will not only not succeed in keeping precarious workers home but may negatively impact the already limited healthcare access of this group.
Marginalization and Precarious Work
In the 2000’s, social scientists called attention to the expansion of precarious work, or work that employers touted as flexible, but workers found inconsistent and poorly compensated. In the same breath scholars also called attention to the tendency of marginalized people to perform precarious work. In The Precariat: The New Dangerous Class Guy Standing expanded the concept of the precariously employed into a global phenomenon with an emerging global worker class dubbed “the precariat”. He drew attention to the fact that precarious work was a global trend, and how even across different national and cultural contexts, this type of “bad” work was the purview of marginalized people. The connection between the marginalized and precarious employment seems robust to not only different national contexts but also changes over time. In The Temp Economy, From Kelly Girls to Permatemps in Postwar America Erin Hatton drew on the case of temporary “temp” workers to illustrate how even as the kinds of temporary work changed over time the bulk of the people relegated to these under-compensated positions were still marginalized people.
The propensity of marginalized people to hold precarious employment means that not only are precarious workers likely already experiencing intersecting disadvantage, but they are trapped in positions that worsen it. The cumulative disadvantage of precarious employment negatively impacts other sectors of the lives of workers. In their study on hospitality workers, Bohle, Quinlan, Kennedy, and Williamson confirmed the usual disadvantages of precarious work including workers reporting having little control over their work schedule and earning less than permanent hospitality workers, but they also found that these disadvantages hurt their family life and negatively impacted their health. A study drawing on the Canadian Survey of Labor and Income Dynamics by Heather Scott-Marshall and Emile Tompa also found that the stress that came from precarious work conditions hurt worker health.
In the United States, a country with a notoriously scarce social safety net, precarious workers not only have less income, but also less access to benefits that Americans usually get from their employers like healthcare. Furthermore, the connection between precarious work and poor health as well as poor health access holds up in research across the globe.
College students at a beach party during spring break.
Christopher Kuszajewski via Pixabay

Kim, Kim, Park and Kawachi explored the link between precarious employment and health in Korea. The researchers used propensity score methods on the Korea Labor and Income Panel Survey to test whether people who held precarious jobs reported worse health than people like them that held stable employment. The researchers found a negative link between reported health and precarious employment, but also found that a lot of the initial relationship could be attributed to the fact that vulnerable people were more likely to hold precarious employment in the first place. Scholars Cranford, Vosko, and Zukewich in Canada also found that precarious work was gendered and racialized. In other words, marginalized people are more likely to do precarious work than non-marginalized people, not just in the United States, but all over the world. Thus, when social scientists set out to investigate precarious employment and its impacts, they are by extension, also researching the impacts of race, gender, migration status, poverty, and the intersections of these.
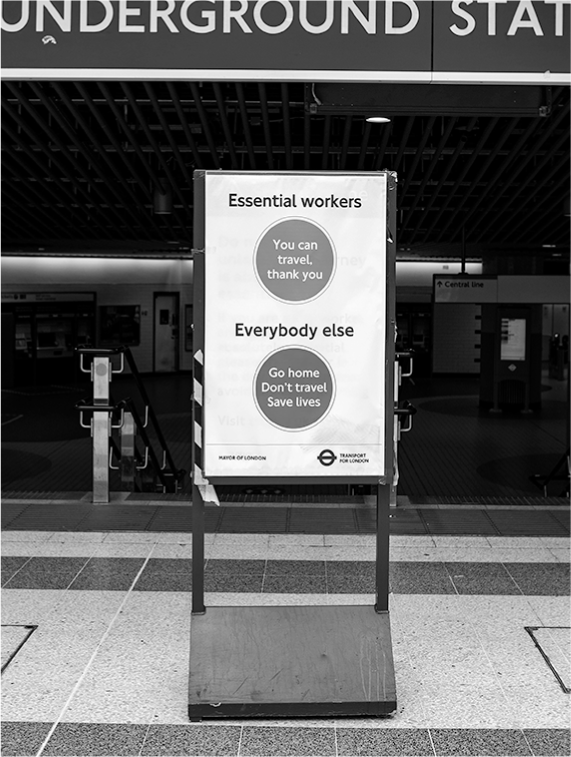
A sign at an underground rail station demonstrates that, for some, the safety of social distancing isn’t an option.
Ben Garratt on Unsplash
The Healthcare as Self-Care Narrative
During the COVID-19 pandemic, the cumulative disadvantage of precarious employment has worsened. Relief programs like the Pandemic Additional Compensation (PAC) payment and Pandemic Unemployment Assistance (PUA) that have provided limited support to Americans have excluded undocumented workers altogether, rendering them some of the most vulnerable amongst the precariously employed.
There has been plenty of literature documenting the difficulty that DACA and undocumented immigrants have accessing physical and mental healthcare. In their focus group study with DACA eligible immigrants Raymond-Flesch, Siemons, Pourat, Jacobs, and Brindis found that young undocumented immigrants had a hard time accessing health services, especially mental health help. Gonzales, Suarez-Orozco, and Dedio-Sanguineti came to a similar conclusion regarding the special difficulty undocumented migrants had in accessing mental health resources. This is particularly worrisome considering the robust literature showing that undocumented migrants incur what Schapiro, Kools, and Weiss referred to as “migration traumas” on their journeys.
In my work with Stanford’s Immigration Policy Lab, myself and Dr. Tomás Jiménez managed an interview study with 50 undocumented and DACA recipient immigrants in the communities of some of the most precariously employed in the United States. The lack of access to health services in the lives of our respondents was not shocking. What was unsettling was that the respondents saw using health services as a decadent thing to do while living in a home where money was always tight. Iris, the young mother of a little girl, summarized the sentiment of the other respondents saying, “We’re not used to going to the doctor… Hispanic people usually don’t go. It’s like a luxury for some people, right”. Even though Iris did not go to the doctor and seemed to see it as a luxury, she didn’t approach her daughter’s health this way. In fact, she took her daughter to the doctor and dentist regularly. When she was asked if there was anything that would stop her from taking her daughter to the doctor Iris answered: “No…I don’t care having the bill at home and having to pay for it. If it was necessary, then we kind of have to, right?”
Health was a resource that had to be budgeted and could only be granted to children, the elderly, or the gravely ill. One of the interviewees, Lalo, a middle-aged man struggling to cope with his diabetes put it succinctly: “You realize you can’t afford your own disease… I don’t want to spend money. They say, ‘Why don’t you? We’re talking about your health.’ Well, yes but am I just going to spend money on something that doesn’t have a solution?” Lalo weighed spending money on his diabetes against spending money on his children, the eldest of whom was also chronically ill, and decided on the latter. He dealt with his son’s health with a sensitivity he did not exhibit towards his own: “if Eduardo Jr. has a fever, we run to the doctor. We can’t wait for the fever to drop. If the fever appears, we run.”
Things that are broadly considered essential to maintaining health like administering insulin, resting after chemotherapy, or getting a dental check-up were discussed as if they were massages or aromatherapy. Adela, a young woman who supported her mother, who had survived several ovarian cancer relapses, referred to going to the dentist and financing her braces as a personal decadence: “I always wanted braces but finally, I was like this is my moment of treating myself, of actually getting braces.” She also discussed how she used to engage in traditional self-care activities like using facemasks and pleasure reading but had taken on more work in order to afford a different luxury: a sick day for her mother. Adela described the moment she could give her mother this luxury: “But once I got…three private jobs…! was like, ‘No, mom. Stay home. It’s fine, it’s fine.’ I saw it in her eyes. She knew she could stay home. And that was me stepping up in order for her to have a real sick day.”
The interviews also illustrated how undocumented children de-prioritized their health as they grew-up. Adriana, a woman in her late 20’s, recalled how she started noticing that dealing with her health was a negative externality on her mother’s life: “I only remember getting sick once in middle school… I was so scared, because she [my mom] had to get off work and she took the bus.because I had a fever and I was throwing up… I knew what a hassle it would be for my mom to come… Because most people, you call their parents and they’re like, ‘Yeah. I’ll be there in an hour’. But I knew, in my head, I’m like, ‘How is she gonna…? There’s just no way… I went to school in a different city.”
Fernando, a young man who was also in his 20’s, articulated how he too experienced this transition: “I used to get checked up once a year, and my teeth got checked up every six months… However, health-wise, I have not gotten checked up since high school… For me, I don’t go to the doctor until I’m bad. I don’t want to be a burden to my parents.” Fernando outlined how as he transitioned from being a teenager into being a young adult his healthcare usage dwindled from consistent to only when he was “bad” so as not to burden his family.
Undocumented immigrant workers are some of the most vulnerable members of our labor market and society. This photo was taken at a March 1, 2018, protest in support of undocumented immigrants and against the xenophobic policies and attack on the Deferred Action for Childhood Arrivals (DACA) program enacted during the Trump-Pence administration.
The Working Families Party via Flickr

While the narratives of Iris, Lalo, and Adela illustrate how undocumented immigrant caretakers prioritize and allocate precious healthcare resources, the reflections of Adriana and Fernando show how as immigrant children grow older and more cognizant, they begin to move out of the category of people for whom healthcare is a need (children, elderly, gravely ill) and towards seeing their own healthcare as self-indulgent. This narrative is useful when you live in constant economic precarity. It allows migrants to allot scarce health resources to those who are most likely to need them, but it also casts the healthcare utilization of others as superfluous. Respondents made plain that even before the pandemic, the precariously employed had to be strategic, and thus exclusive, in their healthcare usage. In other words, the scarcity of resources that precarious workers, and undocumented workers in particular, experience has long had negative consequences on their health.
Conclusion
The stories of my respondents illustrate the ways in which they think about their health and that of their families as well as the healthcare as self-care narrative that some of the most vulnerable precarious workers in the United States employ to allot limited health resources. They also distill the structural reasons that keep precarious workers on the street. By virtue of the type of work they do, they lack: the ability to work from home, the economic resources to subsist without continuous work, and access to healthcare. By virtue of the scarce American safety net, precarious workers lack the economic support to stay home from work and, in the case of undocumented workers, are institutionally excluded from healthcare. As long as these three needs are not addressed, it will be virtually impossible for precarious workers to shelter-in-place.
If we return to the case of the NYC people yelling at pedestrians from their apartment window, we see that social pressure can be a powerful tool when it is directed towards people who have the viable option of staying home. Stigmatizing the precariously employed, however, will likely not keep them home because it will not tackle the main factors that force them out in the first place: the type of employment they have, their income, or their access to healthcare. Social stigma will not keep precarious workers home, but that is not to say it will not have any effect on them. Stigma has very real consequences on the stigmatized. It can impact whether people who cannot afford to socially distance themselves actually end up seeking medical attention and whether they feel they will not be blamed for contracting a disease.
Marginalized people are some of the hardest hit by the COVID-19 pandemic. According to COVID Racial Tracker data racial and ethnic trends are emerging with Latinx and Black people being disproportionately likely to become infected and Black Americans being twice as likely to die of COVID-19. Stigmatizing those exposed to COVID-19 can worsen the virus’s impact and further isolate Latinx and Black communities.
The United States’ lack of social and economic support for workers and the poor specifically, has long had negative health consequences. It is simply during public health crises that the negative health effects of widespread economic precarity are on display not just in how they impact the health of the precariously employed themselves but the health of the entire country.