
Abstract
GBD Epilepsy Collaborators. Lancet Public Health. 202;10(3):e203-e227. doi: 10.1016/S2468-2667(24)00302-5 Background: Epilepsy is one of the most common serious neurological disorders and affects individuals of all ages across the globe. The aim of this study is to provide estimates of the epilepsy burden on the global, regional, and national levels for 1990-2021. Methods: Using well established Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) methodology, we quantified the prevalence of active idiopathic (epilepsy of genetic or unknown origin) and secondary epilepsy (epilepsy due to an underlying abnormality of the brain structure or chemistry), as well as incidence, death, and disability-adjusted life-years (DALYs) by age, sex, and location (globally, 21 GBD regions and seven super-regions, World Bank country income levels, Socio-demographic Index [SDI], and 204 countries) and their trends from 1990 to 2021. Vital registrations and verbal autopsies provided information about deaths, and data on the prevalence and severity of epilepsy, largely came from population representative surveys. All estimates were calculated with 95% uncertainty intervals (UIs). Findings: In 2021, there were 51.7 million (95% UI 44.9–58.9) people with epilepsy (idiopathic and secondary combined) globally, with an age-standardized prevalence of 658 per 100 000 (569–748). Idiopathic epilepsy had an age-standardized prevalence of 307 per 100 000 (235–389) globally, with 24.2 million (18.5–30.7) prevalent cases, and secondary epilepsy had a global age-standardized prevalence of 350 per 100 000 (322–380). In 2021, 0.7% of the population had active epilepsy (0.3% attributed to idiopathic epilepsy and 0.4% to secondary epilepsy), and the age-standardized global prevalence of epilepsy from idiopathic and secondary epilepsy combined increased from 1990 to 2021 by 10.8% (1.1–21.3), mainly due to corresponding changes in secondary epilepsy. However, age-standardized death and DALY rates of idiopathic epilepsy reduced from 1990 to 2021 (decline of 15.8% [8.8–22.8] and 14.5% [4.2–24.2], respectively). There were three-fold to four-fold geographical differences in the burden of active idiopathic epilepsy, with the bulk of the burden residing in low-income to middle-income countries: 82.1% (81.1–83.4) of incident, 80.4% prevalent (79.7–82.7), 84.7% (83.7–85.1) fatal epilepsy, and 87.9% (86.2–89.2) epilepsy DALYs. Interpretation: Although the global trends in idiopathic epilepsy deaths and DALY rates have improved in the preceding decades, in 2021 there were almost 52 million people with active epilepsy (24 million from idiopathic epilepsy and 28 million from secondary epilepsy), with the bulk of the burden (>80%) residing in low-income to middle-income countries. Better treatment and prevention of epilepsy are required, along with further research on risk factors of idiopathic epilepsy, good-quality long-term epilepsy surveillance studies, and exploration of the possible effect of stigma and cultural differences in seeking medical attention for epilepsy. Funding: Bill and Melinda Gates Foundation.
Commentary
Epilepsy is a chronic neurologic disorder that spares no socioeconomic or geographic demographic. The long-standing stigma surrounding the diagnosis contributes to significant underreporting, obscuring the true occurrence of the disease. As a result, epidemiological studies in epilepsy are both essential and uniquely challenging. They play a critical role in identifying at-risk populations, informing prevention strategies, shaping public health policies, and addressing disparities in care and outcomes.
The Global Burden of Diseases is the largest, detailed scientific collaborative effort led by the Institute for Health Metrics and Evaluation to quantify temporal health trends for different diseases. 1 Using data compiled from global surveys, censuses, administrative registries, and cohort studies, they periodically generate measures of disease frequency, morbidity, and disability statistics. The unique advantages of this publication are: (1) They are periodically updated using a standardized and systematic approach, enabling comparisons over time and across different diseases. (2) They represent a global collaboration involving hundreds of scientists from diverse regions and settings, reflecting the wide spectrum of epilepsy environments. (3) They incorporate data from multiple sources, including negotiated access to governmental datasets, making them the most comprehensive and reliable source of epilepsy-related health metrics.
The highlighted paper is the second in a series revisiting three decades of global epilepsy data. The first publication, released in 2019, analyzed trends from 1990 to 2016. 2 This updated study builds upon its predecessor by providing more granular estimates—specifically distinguishing the prevalence of secondary epilepsy, rather than treating epilepsy as a single, undifferentiated entity. This distinction is important, as the underlying mechanisms differ significantly: idiopathic epilepsy is often genetic or inherited, while secondary epilepsy results from identifiable neurologic insults such as infections, perinatal injuries, or stroke and may be more amenable to prevention or targeted public health interventions. Table 1 summarizes the differences between the results published in the Global Burden of Disease Studies of 2019 and 2025. Notably, the study periods overlap, and the patient cohorts are not mutually exclusive; rather, one is a subset of the other.
The Differences Between the Global Burden of Disease Study Published in 2019 and 2025.
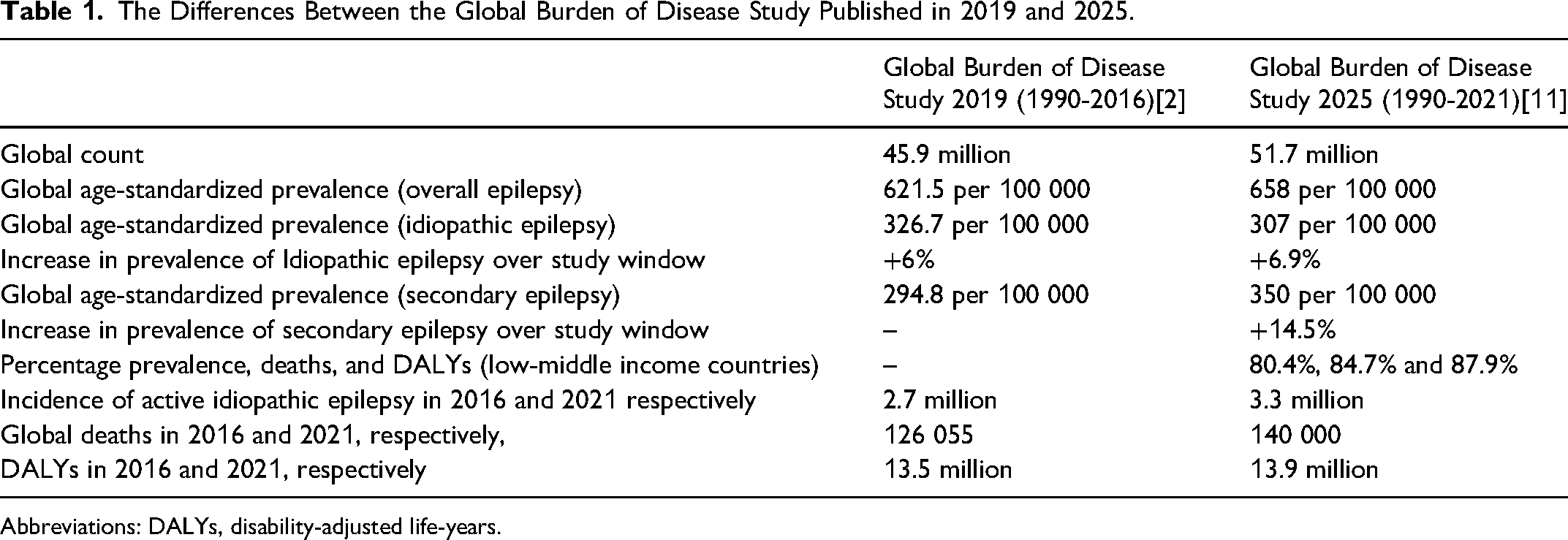
Abbreviations: DALYs, disability-adjusted life-years.
These findings bring several important insights to the surface. Of the 51.7 million people living with active epilepsy worldwide, a striking 83.7% are in low- and middle-income countries (LMICs)—a pattern that has been consistently reported across studies. This is partly because LMICs make up about 80%–85% of the world's population. But in reality, the burden in LMICs is likely underestimated due to underdiagnosis, lack of access to care, and incomplete national datasets. In fact, some countries have not even conducted a national census in decades—Lebanon (1932), Afghanistan (1979), Uzbekistan (1989), and DR Congo (1984).3,4 Furthermore, many of these regions struggle with limited healthcare infrastructure, meaning a majority of people with epilepsy may not be receiving the care they need. Unsurprisingly, this is reflected in disproportionately high rates of epilepsy-related mortality (85%) and disability (87%) in the data.
One of the more interesting points raised in the study is that secondary epilepsy seems to be driving most of the cases in LMICs. This is accurately explained by the authors as being due to increased exposure to perinatal insults, zoonotic, and other infections. To address this preventable burden, improving access to prenatal and neonatal care, expanding vaccination and deworming programs, and implementing injury prevention measures—particularly in rural and underserved areas—should be prioritized as key strategies in epilepsy prevention. Conversely, idiopathic epilepsy remains independent of income level raising the possibility of a racial or genetic predisposition at play, though no clear patterns emerge from the study's geographic heatmaps.
Another perplexing observation is the relatively high prevalence of idiopathic epilepsy in older adults. While this would be expected in secondary epilepsy, the genetic epilepsies usually present earlier in life, and some even remit with age. Grouping idiopathic and cryptogenic epilepsy may account for this finding, particularly in settings with limited neuroimaging, where small strokes or subtle cortical changes may be missed, resulting in the misclassification of secondary epilepsy as idiopathic.
One of the main limitations introduced by pooling data from diverse sources is a selection bias, as data disproportionately come from high-income countries, with sparse representation from rural and remote regions. For instance, in the United States, the CDC relies on telephone surveys to estimate epilepsy prevalence: (1) whether a person has ever been diagnosed with epilepsy, (2) whether they are on antiseizure medication, and (3) whether they had a seizure in the past year. Individuals with milder, untreated, or undiagnosed epilepsy—especially in rural areas—may be missed, leading to underestimation.
Additionally, this publication adheres to the 1985 ILAE classification of epilepsy. However, major revisions were introduced in 2010 and again in 2017, driven by advances in neuroimaging and genetics that have significantly deepened our understanding of epilepsy.5–7 The decision to use the older classification in this study was likely made to ensure consistency with the previous 2019 report and because the updated classification may not be widely adopted in many regions—particularly where access to advanced diagnostic tools remains limited. Adding to the complexity, the International Classification of Diseases codes used by many national health systems are not aligned with the most recent ILAE framework. 8 Since much of the data in global registries depends on these outdated codes, discrepancies are inevitable. Moreover, epilepsy classification by physicians is only accurate about 70%-80% of the time, with considerable variation across and within countries.9,10 Together, these limitations introduce heterogeneity and potential classification bias, which may impact the accuracy of the study's findings.
Ultimately, this is a critical epidemiological study that advances our understanding of epilepsy's global burden. Despite limitations, it offers essential data to guide public health policy, especially in underserved regions. Policymakers can leverage these insights to prioritize prevention, improve care, and allocate resources more equitably. Continued efforts to enhance data quality and classification will be key to refining future strategies.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.