
Abstract
Numerous factors including social determinants of health, knowledge gaps, economic challenges, workforce limitations, and health system deficiencies are associated with significant disparities in access to health care services and health outcomes for people with epilepsy (PWE). The American Epilepsy Society (AES) and the International League Against Epilepsy—North America (ILAE-NA) established a joint task force to explore and develop recommendations to address health care disparities experienced by PWE. The task force gathered foundational knowledge through meetings, public and patient organization comments and discussions to develop consensus recommendations. We enumerate the recommendations and discuss the rationale behind them to reduce disparities in epilepsy care through comprehensive research, inclusive clinical practices, robust advocacy, and targeted educational initiatives. While our recommendations are focused on the United States, we acknowledge that similar barriers and limitations exist for PWE globally and that these also need to be addressed within their local domains and with attention to unique factors therewithin.
Introduction
Significant disparities in access to optimal health care services and health outcomes exist for people with epilepsy (PWE) across rural disadvantaged communities and historically marginalized populations in multiple domains of health care delivery, including diagnosis, treatment, and management.1–3 Members of these populations face systemic barriers that prevent them from accessing and receiving equitable care. 4 Disparities are influenced by numerous social determinants of health (SDOH), knowledge gaps, economic challenges, workforce limitations, and health system deficiencies. For patients with refractory epilepsies as well as rare and complex epilepsies, these challenges are magnified, resulting in additional disparities from difficulty accessing high-quality, specialized care.5,6
Disease-specific stigma plays a key role in perpetuating disparities as PWE experience severe health and health care disparities, compared to the general population. The literature on epilepsy disparities is extensive, including systematic and narrative reviews,2,7,8 and continues to evolve alongside broader health equity literature.
Addressing health disparities for PWE requires focused, analytical, and deliberate strategies to evaluate root causes (e.g., SDOH and other structural factors) and implement solutions to promote sustainable, transformational change so that all PWE can achieve optimal health.
The American Epilepsy Society (AES) and the International League Against Epilepsy—North America (ILAE-NA) established a joint task force to explore and develop recommendations to address health care disparities experienced by PWE. Task force members were included based on their clinical, research, educational, and other experience in addressing epilepsy disparities and improving access to care in the United States.
This document, produced by the members of the AES and ILAE-NA task force, aims to highlight common disparities in epilepsy care and provides recommendations for improving access to care through advancements in research, clinical care, advocacy, and education.
Task Force Process and Methodology
The task force was convened in October 2023 and met bi-weekly through September 2024 to identify foundational knowledge necessary to develop recommendations. Over this period, each bi-weekly session focused on disparities in one aspect of epilepsy care and/or research. Subject matter experts were identified by task force members and invited to provide short presentations and discussions on a topic related to disparities (Appendix A). Topics included epilepsy self-management, outcomes from Project ECHO® (Extension for Community Healthcare Outcomes), Common Data Elements, the work of the Epilepsy Foundation, and epilepsy disparities in historically marginalized and minoritized populations. At least 10 task force participants attended each session. At the end of each session, the task force discussed possible steps for improving access in the session's focus area. Task force leaders consolidated and categorized proposed action steps, leading to two cycles of feedback, discussion, and refinement that ultimately led to this report.
The first draft of the recommendations was made available for public comment on the AES website for 30 days in October 2024. Notification of the public comment period was sent via email to the AES member database email list and direct solicitation of the community perspective was solicited through the Epilepsy Leadership Council (ELC). Twenty-five individuals and organizations submitted comments. Each comment was discussed among the task force and considered as the recommendations were revised.
Results
We outline common barriers to equitable epilepsy care, acknowledging that additional challenges may exist beyond those identified here.
Knowledge Gaps
There is insufficient research into effective and sustainable methods for addressing known disparities in epilepsy care. To date, PWE have had limited opportunities for involvement in identifying crucial barriers to their care and co-developing solutions. Co-produced directives, research, and programmatic efforts are essential for reducing these barriers to improve outcomes and enhance the well-being of our patient communities. 9 Involving and elevating the voices of PWE—and their caregivers—is vital to improving basic health literacy and self-management techniques, setting optimal care goals and creating measurable outcomes that reflect the needs and priorities of PWE.
Social Factors
Historically and socially marginalized populations often face exclusion from the health care system. The unique strengths and perspectives of these populations are rarely incorporated into research, education, or clinical care models. Many health care providers lack adequate training to address the needs of underserved populations, in addition to epilepsy-specific challenges such as care partner burden and social stigma. 10 Women may face care barriers related to reproductive health. Lack of paid family and medical leave restricts access to epilepsy care. Epilepsy affects multiple aspects of life, including driving status, employment opportunities, food security, social activity, and the well-being of friends and family. Even insured patients may not receive advanced epilepsy treatments such as surgery or neuromodulation, particularly if they lack the support networks required for the safety and success of such interventions.
Language
PWE with non-English language preferences often encounter communication barriers that hinder trust and cultural understanding with their providers. 11 Beyond language barriers, health literacy and inaccessibility of educational materials further impact care and outcomes. 12
Cultural and Spiritual Diversity
Cultural and spiritual norms influence patients’ perspectives on health and health care and can influence their understanding and interpretation of medical information.13,14 Specifically related to epilepsy, cultural and religious beliefs may be intertwined with stigma. 15
Immigration Status
Many immigrants with epilepsy in the United States face unique challenges in accessing care, including lack of insurance, language barriers, or fear of deportation for documented and undocumented individuals. These challenges may discourage them from seeking essential health services.16,17
Digital Divide
While telehealth offers significant potential solutions for improving access to epilepsy care for some PWE, 18 disparities in digital literacy and internet connectivity limit its effectiveness for many individuals, particularly those in rural, low-income, or otherwise underserved communities.19,20
Economics
Economic insecurity, inadequate insurance coverage, and employment challenges significantly impact PWE and their caregivers.10,21 Caregiving responsibilities often restrict caregivers’ job opportunities, leading to loss of potential income. Insurance barriers and financial insecurity further contribute to medical debt and reduced access to care.
Geography
Geographic barriers, such as the need to travel for care, affect nearly all PWE but are particularly relevant for PWE residing in rural areas, where access to specialized epilepsy centers and neurologists is limited. Most Level 4 comprehensive epilepsy centers are in metropolitan areas. 3
Workforce
The United States lacks an adequate workforce of professionals trained to care for PWE. 22 This includes advanced practice providers, EEG technologists, community health workers, nurses, pharmacists, psychologists, neuropsychologists, and physicians (including specialists such as pediatric epileptologists and geneticists). Workforce shortages and their detrimental effects are especially acute in areas with higher poverty rates, rural areas, and/or less favorable payer mixes. 23 Furthermore, the neurology workforce does not reflect the demographics of the population it serves. 24 Systemic biases in clinical care settings remain largely unaddressed.
Prolonged Wait Times
Excessive wait times to see a provider are common and disproportionately affect PWE with limited insurance and those from marginalized populations.1,25 Delays in care can lead to inappropriate or insufficient treatment, which can exacerbate mistrust in health care providers and increase epilepsy-related morbidity and mortality.25,26
Recommendations
Guided by the informational sessions and responses from the public comment period, the task force developed actionable recommendations to address epilepsy health care disparities through research, clinical care, advocacy, and education.
Research Recommendations
AES should develop a grant mechanism to support research on solving known disparities caused by social determinants of health (SDOH).
Funding agencies should broaden the collection of SDOH data beyond age, gender, race, and ethnicity within epilepsy common data elements.
All epilepsy clinical research grant applications funded by public or private institutions should include a plan to engage, recruit, and retain historically marginalized populations to optimize the study's representativeness.
In line with the National Academies of Sciences, Engineering, and Medicine's recommendations, 26 journal editors should require information on the representativeness of study populations for journal submissions.
Funders, research institutes, and individual researchers should prioritize efforts to adopt patient-centered approaches to epilepsy research, actively integrating the voice and lived experiences/expertise of PWE and caregivers in all stages of the research process.
The committee discussed the rationale for these recommendations, summarized below.
A new grant mechanism: At this writing, AES offers one grant mechanism designed to encourage research on addressing health disparities. The Sergievsky Award for Epilepsy Health Equity and Diversity is available for early career investigators, including those who self-identify as members of underrepresented populations; the award encourages research on SDOH but is open to other topics. Establishing a specific grant mechanism that supports efforts to solve the known disparities based on SDOH may attract more investigators whose research focuses on SDOH and public health in epilepsy, encourage current researchers to focus on SDOH, and foster collaboration between epilepsy researchers and researchers outside of epilepsy who have SDOH expertise. Partnerships with advocacy groups and/or foundations to co-sponsor such awards may provide access to additional funds.
SDOH data collection: The task force acknowledges that SDOH can vary across populations, such as children and local vulnerable populations. Researchers can use ICD-10-CM SDOH Z-codes to harness EMR data for clinical research and tracking epilepsy care outcomes. While Z-codes may offer researchers additional information to understand and eventually ameliorate the negative impacts of SDOH, their collection must be thoughtfully and systematically integrated into health care delivery services across the nation to glean accurate, representative data. Additionally, the task force recognizes that Z-codes may not capture all SDOH and recommends encouraging researchers to identify and include other measures (e.g., disability status) in their research.
Representativeness of study participants: Representativeness refers to the extent to which the participants in a clinical study are similar to the broader population the research aims to represent. It is essential to ensure that the results of epilepsy clinical research can be applied to the appropriate and, ideally, broadest possible population and that those potential interventions are safe and effective for all individuals. The National Academies of Sciences, Engineering, and Medicine has provided recommendations to improve representativeness of clinical studies. 26 Moreover, the requirements set by scientific journals to ensure the representativeness of trials could help advance this effort. Promoting research reporting guidelines for publications involving health equity among historically marginalized and minoritized populations may help prevent the continued legacy of health research from ignoring and/or exploiting these groups.
Patient-centered approaches: Engagement of the patient community, including parents and caregivers as appropriate, and patient advocacy groups in research design, implementation, analysis, and results dissemination is critical. In addition, priorities for epilepsy research outcomes can vary significantly among patient groups and individuals. The Patient-Centered Research Outcomes Institute (PCORI) has provided recommendations for partnerships in research (https://www.pcori.org/engagement-research/engagement-resources). To address these diverse needs, an intentionally inclusive approach to conducting research and disseminating outcomes is essential and may involve expanding research efforts beyond academic institutions to include rural and community-based settings.
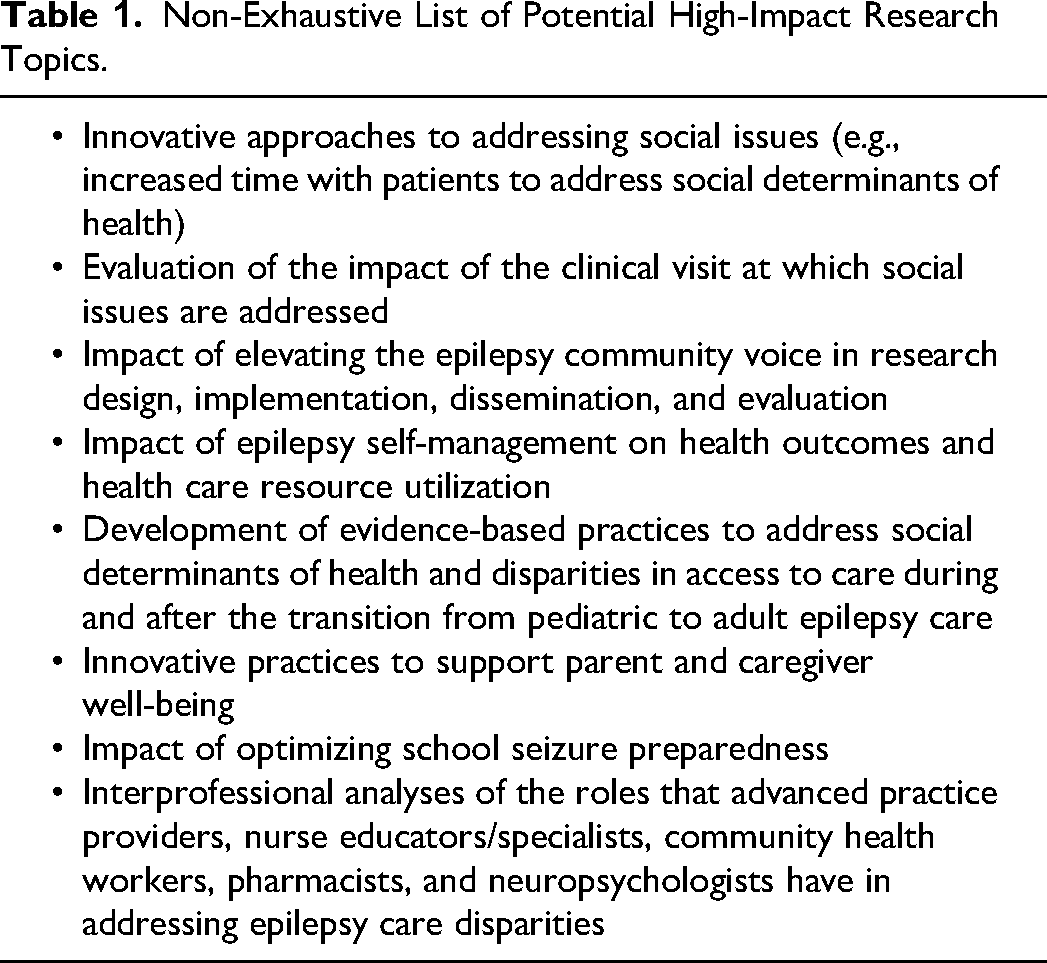
The task force considered many areas of epilepsy research that can reduce disparities, which are displayed in Table 1.
Non-Exhaustive List of Potential High-Impact Research Topics.
Clinical Care Recommendations
The task force recommends expanding the epilepsy workforce by including nurse specialists, educators, community health workers, pharmacists, mental health clinicians, and neuropsychologists as core members of epilepsy care teams and developing practice recommendations for the integration of services of pharmacist and community health workers.
Adopt a structured framework for integrating mental health services into epilepsy care, ensuring a holistic approach to patient management.
Develop adequate support at epilepsy centers for appropriate medical care beyond neurology for mental health and other subspecialty services (e.g., orthopedic, cardiology, gastroenterology, physical medicine and rehabilitation, etc.) for individuals with epilepsy and other complex conditions and comorbidities, including intellectual and developmental disabilities.
Expand care models to include telehealth and digital tools for epilepsy management.
AES should provide expertise for the existing Rare Epilepsy ECHO® and Epilepsy Specialist ECHO® Hubs and expand to a national ECHO® program for neurologists focused on refractory and rare epilepsies.
Form an AES workgroup to develop practice recommendations for widely available epilepsy self-management programs.
Adopt ICD-10-CM Z-codes for SDOH screening.
Improve support for PWE's pediatric and adult care transitions, especially for patients from minoritized populations.
Develop accessible programs for populations with non-English language preferences, focusing on areas with the most significant impact, to promote the linguistic aspect of culturally competent epilepsy care.
Promote diversity in epilepsy care teams by ensuring epilepsy centers recruit, train, and retain a diverse workforce.
Form a work group to develop trackable metrics of epilepsy disparities.
Below we detail the rationale for our clinical recommendations:
Interdisciplinary epilepsy care teams: expanded workforce. A holistic approach to patient management can improve patient outcomes and enhance care delivery, and optimize the team's ability to address barriers, including medication access. AES and its partners can advocate to include a variety of health professions, including nurse specialists, nurse educators, community health workers, pharmacists, mental health professionals, child life specialists, and neuropsychologists as core members of epilepsy care teams. While nurse specialists, pharmacists, some mental health professionals, and neuropsychologists are recognized by insurers for some services, not all are covered.
Comorbidities and integration of mental health services. The burden of comorbidities—medical, psychiatric, and cognitive—in PWE is high. 27 Comprehensive epilepsy centers should engage with other professionals to ensure adequate medical care beyond neurology and mental health for PWE who have other complex conditions, including intellectual and developmental disabilities. In appropriate clinical settings, health care providers should consider integrating more mental health clinicians into clinical epilepsy care. The task force acknowledges that barriers such as insurance coverage, requirements to prioritize clinical space utilization for higher revenue-generating services, and workforce shortages (including and beyond physicians) currently challenge the feasibility of this recommendation. Nevertheless, a holistic approach to patient management can improve patient outcomes, enhance care delivery, and enhance the team's ability to address barriers, including medication access.
Telehealth and digital tools. Overcoming geographic barriers between PWE and epilepsy specialists and comprehensive epilepsy centers is imperative. The expansion of epilepsy care models to include telehealth and other digital solutions, such as email communication and seizure tracking tools, can enhance patient engagement and improve accessibility to care, especially for those who reside in rural areas of the United States.
Supporting epilepsy-themed ECHO® programs: The ECHO® model is an educational framework that is based on the medical education concept of learning from medical rounds. The virtual environment allows practitioners to connect and discuss a specific topic, including sharing support, feedback, and guidance while learning from specialists in a case-based environment. Supporting ECHO® programs that train primary care providers, general neurologists, and other health care professionals on rare and refractory epilepsies can provide valuable resources and support for delivering effective epilepsy care and increase access by having more knowledgeable providers.
Epilepsy self-management: The need for self-management in epilepsy is paramount because the monitoring and management of seizures, and treatment to control seizures, takes place in the home and community environment and is not isolated to a clinic or hospital. Epilepsy self-management programs have been identified by the Institute of Medicine as a mechanism for improving the lives of PWE. The Centers for Disease Control and Prevention's catalog of evidence-based epilepsy self-management programs, tested in 15 randomized controlled trials and showing patient benefit, are severely underutilized in current epilepsy care streams. For epilepsy self-management programs to be translated from science to service delivery, a national best practice standard of care recommendation that serves to increase the relevance and meaning to patients, providers and practices will be required. National frameworks for building capacity and achieving population-level health impact through the broad dissemination of self-management strategies exist for other chronic diseases (e.g., diabetes, asthma, cardiovascular disease). These frameworks serve as replicable models that can be adapted to enhance whole-person epilepsy care and improve health and quality of life outcomes. 28
Z-codes: Using ICD-10-CM SDOH Z codes during clinical care will help relate epilepsy care outcomes to the economic and social factors captured by these codes. Z-codes can also be useful in research to collect SDOH data. The task force recognizes that Z-codes do not capture all SDOH.
Transitions: As children with epilepsy age, their care will be transitioned from a pediatric epilepsy specialist to an adult epilepsy specialist or adult neurologist. Transition planning should be intentional and anticipate future aspects of the patient's care that will need to be addressed. 29 Supporting PWE, especially those from minoritized populations, in this transition is vital. Developing evidence-based approaches and clinical practice guidance on transition of care will be vital to these efforts.
Language accessibility: Individuals with non-English language preferences may face barriers accessing programs or services for epilepsy care. Offering written translations of resources and providing access to interpreter services, when available, can improve access and outcomes. These services are covered under the Healthcare Common Procedure Coding System under code T1013, allowing for coverage of real-time, spoken interpretive services per 15 minutes. Despite this coverage, health care systems face challenges in initial investment costs of contracting with interpretation vendors and cultivating the necessary structures that support successful implementation of interpreter services across the site, regardless of size.
Care team and educational content diversity: Efforts to increase workforce diversity in epilepsy care should include targeted recruitment, mentorship programs for members of underrepresented groups (including training and support for their mentors), and policies that foster inclusivity and equity in training and professional development. Patients are more likely to trust and seek care from providers who share or understand their cultural backgrounds.30–34 Recruiting diverse clinical team members—physicians, nurses, social workers, mental health professionals, psychologists, EEG technologists, and pharmacists—to better reflect patient demographics can improve patient engagement with epilepsy care. Additionally, training and professional development promoting cultural humility can improve health care providers’ ability to provide high-quality, inclusive care for patients outside their cultural background. 35
Trackable metrics: Unfortunately, metrics to track the efficacy of health equity interventions on epilepsy outcomes are lacking. Investing in the development of reliable and trackable metrics, including clinical outcomes, quality of life, and health care access, is essential to systematically address disparities and improve the lives of individuals with epilepsy in underserved populations.
Education Recommendations
Collaborate with partner organizations to identify and disseminate existing resources or develop and disseminate new resources related to unconscious bias training, comprehensive epilepsy education, awareness of socioeconomic disparities, premature death risks, and cultural competence and humility training.
Collaborate with partner organizations to promote inclusion in workforce discussions.
Collaborate with partner organizations that serve primary or secondary public, private, and charter school personnel to promote Seizure Safe School training, implementation of seizure action plans, and student education about epilepsy.
Collaborate with patient advocacy groups to promote educational initiatives and to disseminate reputable education and support resources for PWE.
AES educational sessions should support implementation science methodology, and best practices for community-engaged research (e.g., use of community-based participatory research methodology), and for engagement with patients and advocates across the research lifecycle.
Create educational programs designed for providers working with culturally diverse populations.
Here, we describe the rationale for the recommendations related to education.
Professional development through collaboration: Expanding professional development opportunities for current health care providers is a crucial step to enhance their capacity to support individuals with epilepsy and address disparities effectively. Collaboration among diverse professional organizations can generate resources, incorporating multiple perspectives to meet multifaceted learning needs. Vital educational activities include those that address unconscious bias, the importance of referring patients to epilepsy specialists and comprehensive epilepsy centers, identifying the socioeconomic challenges faced by epilepsy patients, the risks of premature death and awareness about Sudden Unexpected Death in Epilepsy, and cultural competence and humility.
Workforce expansion through inclusion and collaboration: Numerous health care professionals contribute to epilepsy care. Workforce development plans include recognizing these professionals and their contributions to safe and effective care for PWE. Both conceptual knowledge about cultural differences and lived experiences of their patients, and technical skills that enhance the quality of care for PWE can be taught. For example, providing EEG technologists with training on techniques that accommodate different hair textures and styles can improve EEG quality.
School personnel and safe schools: School staff should be provided with the knowledge and skills to properly recognize and respond to seizures. They should also have access to Seizure Action Plans to help guide appropriate responses. Organizations can collaborate to actively educate school staff and students on ensuring the safety of PWE by providing timely and appropriate seizure and first aid that can reduce potential harm during a seizure. This can, in turn, create a supportive learning environment where students with epilepsy feel comfortable and safe and can reach their full academic potential.
Further, policymakers can support Seizure Safe School legislation, mandating seizure recognition training for school personnel and ensuring students can carry their medications at school. Supporting initiatives such as the Seizure Awareness and Preparedness Act can provide grant funds for schools to develop programs that train school personnel on individualized epilepsy plans and individualized emergency seizure for students who have epilepsy or a seizure disorder.
Education and support resources for PWE: Stereotypes and misinformation about epilepsy are common, with many believing epilepsy is a mental illness, contagious, or caused by evil spirits, leading to stigma and discrimination against PWE. Collaboration among epilepsy organizations and patient advocacy groups can produce educational programs to combat these issues and increase epilepsy awareness. Further collaboration can provide health care providers with reputable education and support resources to disseminate to PWE.
Bereavement support services: Epilepsy is associated with a high rate of premature mortality. 36 Epilepsy-focused organizations can partner with other organizations and groups to provide bereavement support services for families affected by traumatic loss due to epilepsy. These resources should be developed to meet the health literacy needs of the target audience and disseminated to all PWE and their families, including newly diagnosed families, to ensure they know how to best advocate for effective epilepsy care.
Educational on community-based research: The promotion of best practices for community-engaged research, such as the community-based participatory research methodology, can improve engagement with patients and advocates across the research lifecycle. Educational activities such as the AES Annual Meeting Investigator Workshops focused on implementation science could motivate investigators to pursue research that addresses SDOH and improve the quality of grant applications and funded research.
Advocacy Recommendations
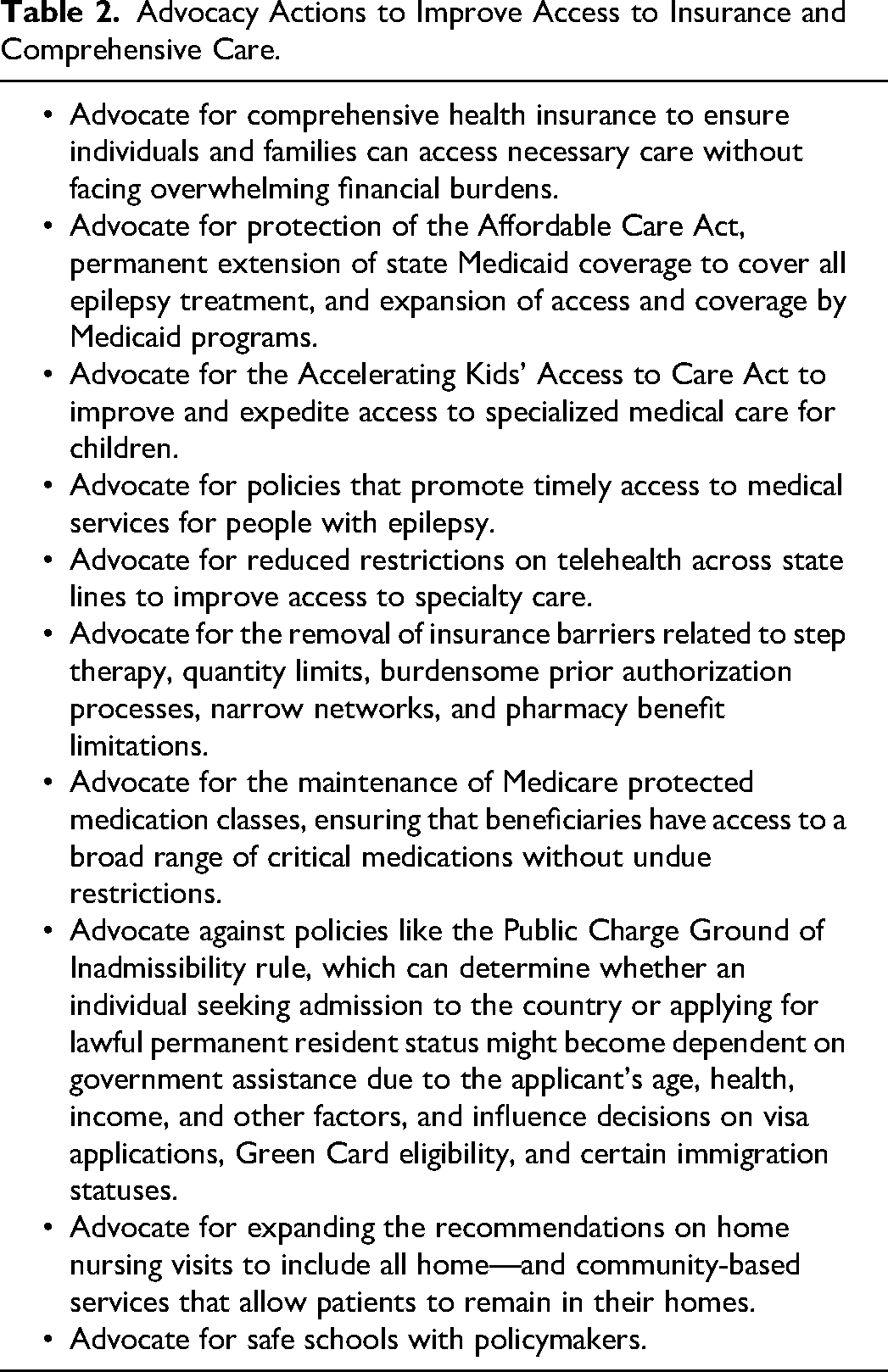
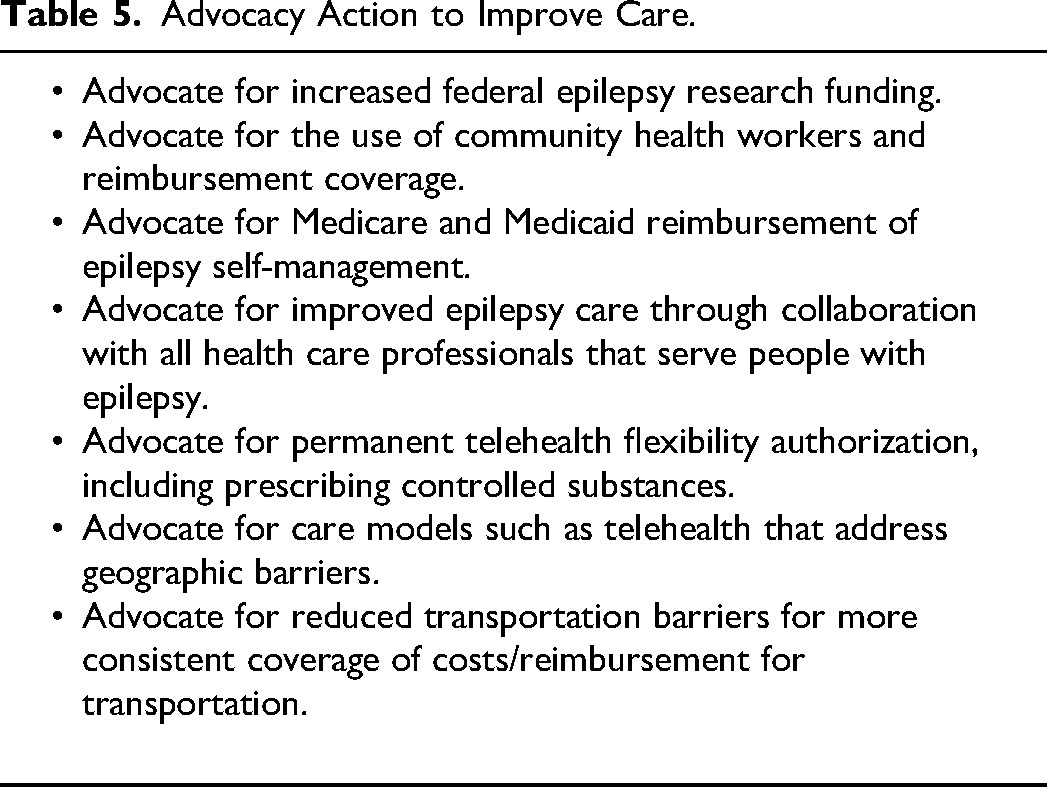
AES should develop sustainable advocacy engagement strategies, including a national action plan for epilepsy. The epilepsy community can implement the above-outlined recommendations regarding research, clinical care, and education through strong advocacy for resources. Developing a sustainable advocacy engagement strategy is the cornerstone to promoting long-term improvements in epilepsy outcomes. By maintaining a consistent and well-resourced advocacy approach, the community can foster environments where individuals with epilepsy live healthier and more empowered lives. The task force has identified four advocacy themes with potential strategies to improve patient outcomes. These are (a) improving access to insurance and comprehensive care, (b) improving data collection, (c) reducing the burden of epilepsy, and (d) improving care. Tables 2–5 list specific advocacy actions.
Advocacy Actions to Improve Access to Insurance and Comprehensive Care.
Advocacy Actions to Improve Data Collection.
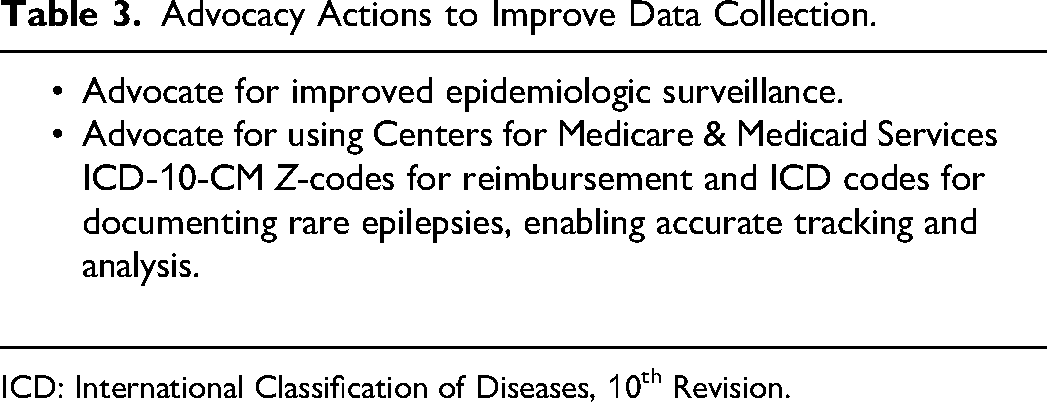
ICD: International Classification of Diseases, 10th Revision.
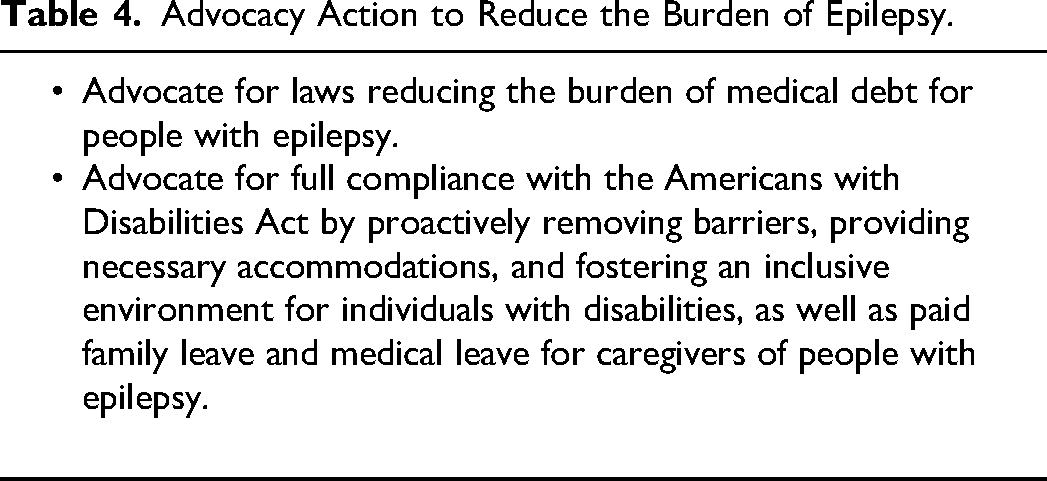
Advocacy Action to Reduce the Burden of Epilepsy.
Advocacy Action to Improve Care.
Conclusion
PWE have significant disparities in health outcomes and access to health care services. The work of this joint AES/ILAE-NA task force highlights prevalent disparities in epilepsy care. It provides recommendations for improving equitable access to high-quality care through research, clinical care, advocacy, and education advancements.
Footnotes
Acknowledgments
The authors would like to acknowledge the following professionals as subject matter experts who shared their time, expertise, and experiences throughout the information-gathering phase of the project: Bernice Martin Lee; Bruce Ovbiagele, MD, MSc, MAS, MBA, MLS; Patricia Osborne Shafer, RN, MN; Qian-Zhou JoJo Yang, MD.
Author Contributions
Jaideep Kapur—1, 3, 5, 6, 10, 11, 12, 13, 14
Dave Clarke—3, 5, 11, 13, 14
Mill Etienne—3, 5, 11, 13, 14
Camilo Gutierrez—3, 5, 11, 13, 14
Barbara C. Jobst—3, 5, 11, 13, 14
Emily Johnson—3, 5, 11, 13, 14
Sucheta Joshi—3, 5, 11, 13, 14
Elaine T. Kiriakopoulos—3, 5, 11, 13, 14
David M. Labiner—3, 5, 11, 13, 14
Fred A. Lado—3, 5, 11, 13, 14
Alain Lekoubou Looti—3, 5, 11, 13, 14
Daniel H. Lowenstein—3, 5, 11, 13, 14
Karen Parko—3, 5, 11, 13, 14
Ellen Riker—3, 5, 11, 13, 14
Renée A. Shellhaas—3, 5, 11, 13, 14
Joseph I. Sirven—3, 5, 11, 13, 14
Karen Skjei—3, 5, 11, 13, 14
John M. Stern—3, 5, 11, 13, 14
Timothy E. Welty—3, 5, 11, 13, 14
Adam B. Eickmeyer—3, 5, 7, 11, 12, 13, 14
Shawna L. Strickland—3, 5, 7, 11, 12, 13, 14
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Appendix A: AES/ILAE-NA Joint Task Force on Epilepsy Health Care Disparities Members
Task force co-chairs:
Jaideep Kapur, MD, PhD, FAES William H. Theodore, MD, FAES
Task force members:
Dave Clarke, MBBS, FAES Mill Etienne, MD, FAES Camilo Gutierrez, MD, FAES Barbara C. Jobst, MD, Dr Med, FAES Emily Johnson, MD, FAES Sucheta Joshi, MD, FAES Elaine T. Kiriakopoulos, MD, MPH, MSc David M. Labiner, MD, FAES Fred A. Lado, MD, PhD, FAES Alain Lekoubou Looti, MD, MS Daniel H. Lowenstein, MD Karen Parko, MD, FAES Annapurna Poduri, MD, MPH, FAES Ellen Riker, MHA Renée Shellhaas, MD, MS, FAES Joseph I. Sirven, MD, FAES Karen Skjei, MD, FAES John M. Stern, MD, MA, FAES Timothy E. Welty, PharmD, FAES Adam B. Eickmeyer, MPH Shawna L. Strickland, PhD, CAE, RRT, FAARC