
Abstract
This brief review summarizes presentations and discussion from the Health Disparities Special Interest Group held in December 2024 at the American Epilepsy Society Annual Meeting. The session addressed known health disparities in pediatric and adult epilepsy at a national and global level. The goal of the session was not just to present the known inequities, but to also propose ideas and work together toward improving healthcare for all. Invited speakers work directly with at-risk communities in the United States and abroad and shared their experiences on how we can do better. This piece is intended to provide a brief overview of the talks given by the invited speakers and to put it all together with the goal of achieving better epilepsy care for all by working together.
Introduction
There are well documented health inequities in epilepsy care for many minoritized communities across the United States and globally. External factors such as socioeconomic status, insurance status, immigration, legal status, language barriers, geographical location, and education level are only some of the barriers our patients face on a day-to-day basis. Nonvariable factors, such as race and ethnicity, also play a big role in health status and outcomes for the patients we care for. These disparities are present in both adult and pediatric populations, although less studied in the latter. There is an urgent need to not just recognize these gaps, but to advocate for our patients and determine how best to achieve equity. At a global level, as we continue to learn about lack of access and resources, we also need to get creative and learn how others have attempted to help shape better health outcomes for all. These disparities not only hinder individual health outcomes but also perpetuate cycles of poverty and marginalization.
The Health Disparities Special Interest Group at the 2024 American Epilepsy Society Annual Meeting convened to address these urgent challenges. The session aimed to go beyond acknowledging inequities by fostering dialogue and proposing actionable strategies to advance equitable epilepsy care for all. This review summarizes the insights shared by speakers with direct experience working with at-risk communities and explores potential solutions to ensure that no patient is left behind.
National Impact
Disparities are defined as preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations. 1 Data from the Center for Disease Control showed that patients with epilepsy in general, may take less medication than prescribed to save money, struggle to pay medical bills and report delaying care because of inadequate transportation. 2 Children with epilepsy have significantly higher odds of living in lower income households and they may not be receiving appropriate or adequate healthcare.
The North American Commission of the International League Against Epilepsy reported that there is substantial evidence that North America minorities with epilepsy may be receiving lower levels of care than the nonminority population. 3 Looking at specific populations, US data has demonstrated that Black patients and individuals with public insurance receive epilepsy surgical procedures at lower rates compared with other patients with drug-resistant epilepsy. 4 Studies have shown that Blacks and Hispanics with epilepsy are less likely to have access to specialized epilepsy care 5 and there is evidence that patients who have access to Epilepsy Centers, receive higher quality care than patients who have their epilepsy care elsewhere. This implies that just offering health insurance is not enough to decrease the treatment gap.
Although there is limited data in the literature, there is enough collective experience to state that healthcare inequalities involving immigrant children and adults with epilepsy—especially those that are undocumented in the United States—are underrecognized. A vast majority of undocumented immigrants are uninsured, which contributes to significant delays or inadequacies in their care. Only a small number of states offer Medicaid coverage, regardless of immigration status for children, but the numbers are even smaller for adults (11 and 3 states, respectively). 6 Therefore, access to care for these patients is often limited to situations of high acuity. Moreover, clinicians taking care of these patients face challenges in ordering basic electrodiagnostic and radiological tests necessary for a timely, accurate, and specific diagnosis of epilepsy. Families report concerns regarding affordability of antiseizure and rescue medications, lack of adequate transportation to access healthcare services and difficulty in navigating the healthcare and school systems for their loved ones with chronic needs. Performing specialized procedures for patients with drug-resistant epilepsy, for a presurgical work-up for example, can be highly cumbersome, if not impossible.
The 2020 Census results demonstrate an evolving population in the United States. Regarding race and ethnicity, the non-Hispanic White group was the most prevalent population in the United States with 57.8% of the population. However, this number decreased from 63.7% in the 2010 Census. The second most prevalent group was the Hispanic/Latino population with 18.7% of the population. 7 The Pew Research Center projected that the Hispanic or Latino population will triple to 128 million by 2050 and be expected to make up 29% of the population. 8 As the population continues to grow and become more diverse, there has been an increase in diversity of languages spoken at home. The 2019 American Community Survey shows that Spanish is the most common non-English language spoken in the United States. 9 As the patient population continues to evolve, medical providers need to consider the patient's preferred language when providing care. Language concordant care is defined as an encounter where the patient and healthcare provider speak the same non-English language (or shared native language). This does not include interpreting services. Language discordant care, on the contrary, is an encounter where patient and health care provider speak different languages. 10 There are multiple benefits to language concordant care such as improving patient outcomes, increasing patient satisfaction, lowering healthcare costs and decreasing medical errors. 11 A study looked at language discordant care in patients with Limited English Proficiency and found that these patients were less likely to receive health education, more likely to report receiving worse interpersonal care and to give providers lower ratings. When an interpreter was used, the only outcome showing improvement was health education. Therefore, even with the aid of interpreters patients still perceived that they received substandard care from providers. 12 Specifically focusing on pediatric epilepsy, a recent paper published in 2019 found significant disparities in Hispanic children. The study found that Hispanic children had reduced likelihood of seizure control with lower probability of remission when compared to non-Hispanic children. 13 In addition, a systematic review published recently found that patients who underwent epilepsy surgical evaluation were most often White and had private insurance. They also found there were differences in time to referral and surgery rates with an increased time to referral and lower rates of surgery for those who identified as Hispanic and/or non-White. 14
Geographical location can also play a big role in health inequities affecting patients living with epilepsy. Specialized centers are usually located in capital cities or large urban centers, while rural areas tend to be underserved. As far as other minority groups, there is evidence of substantial ethnic and racial disparities in obtaining appropriate diagnosis with Native Americans, Native Hawaiians, Pacific Islanders, and Alaskan Natives. 15
National Solutions
The American Epilepsy Society recognizes disparities in epilepsy care. Therefore, it is important to find potential solutions to minimize national disparities. The first step is to understand the factors driving these disparities. Therefore, it is necessary to produce research that includes multiple variables—not only race and ethnicity, but disparities due to gender preference, English proficiency, among others.
The National Institute of Neurological Disorders and Stroke has proposed a useful framework for studying determinants of inequities in neurological disease. This framework emphasizes the various levels and scale of causation and includes the structural and intermediate social determinants of health, with the goal to develop research programs and policies that are long term, impactful, and sustainable. 16
Similar multivariable frameworks address health equity in people living with epilepsy and include sociocultural, structural healthcare, and physiological factors. 17 A comparable model to analyze disparities in epilepsy surgery incorporated multiple factors, such as access to care, fear of treatment, trust/communication problems, education, and social support. 18
Not surprisingly, disparities in epilepsy are complex and multifactorial. They are usually driven by political and social factors that produce an uneven distribution of resources. Multidimensional frameworks can improve our knowledge about root causes of disparities. However, no single intervention can solve all problems, and potential solutions need to be addressed at different levels.
Large academic centers should develop community programs, especially in rural areas, and improve communication between public health practitioners and epilepsy providers or social workers to address gaps in access. Academic centers could support more rural communities with no access to tertiary centers via telehealth modalities. Epilepsy centers should also minimize the economic burden of patients living in rural zones with availability of program coordinators. Virtual platforms should also be utilized for education to primary providers, families, and community leaders.
As an example of what academic centers can do, due to recognized health disparities in pediatric epilepsy in the Hispanic population, Ann & Robert H. Lurie Children's Hospital of Chicago (LCH) created a comprehensive Spanish Epilepsy Clinic. LCH is located in the very diverse city of Chicago and recent demographics show that 47% of patients identify as Hispanic/Latino. In addition, in recent years there has been an increase in the Hispanic/Latino population with the large groups of migrants coming to the city. It is estimated that more than 51 000 migrants have arrived in Chicago since August 2022. 19 Therefore, this data demonstrates that Chicago has a large group of patients that would benefit from language concordant care. The Spanish Epilepsy Clinic was created in October 2023 for patients with epilepsy who identify Spanish as their preferred language. The goals of the clinic are to provide more culturally sensitive care, improve quality of care and patient education, enhance patient experience and satisfaction and increase physician trust. All members of the clinic are fluent in Spanish. As of December 2024, 83 pediatric patients had been seen, ages ranging from 7 months to 22 years old. 47% of patients had at least 1 social influencer of health identified in the medical record, which highlights the importance and value of having a language concordant Social Worker be part of such specialized clinics for vulnerable populations. The hope is to continue to gather data to further assess the impact of the clinic in patient's health and quality of life and analyze how these interventions can reduce financial costs by building trust and improving health literacy within the communities.
At a government level, it is imperative that the policy makers, healthcare managers as well as the treating physicians remain cognizant of this sensitive sociopoliticomedical topic to generate potential solutions. Expanded health insurance regardless of legal status in the United States, more affordable insurance options, and training providers on cultural competency should all be addressed to facilitate care of more vulnerable children.
At an individual level we need to eliminate personal biases or implicit/explicit racism and understand our patients’ needs and sociocultural factors to overcome disparities. Finally, it is important to recognize that disparities are pervasive and tend to persist and as epilepsy providers, we have the responsibility to provide the best possible care.
Global Impact
Epilepsy is recognized as one of the most common neurological conditions across the world, impacting over 50 million people globally. However, around 80% of people with epilepsy live in low resourced countries (LRC). 20 Therefore, it is estimated that about 75% of these individuals living with epilepsy do not have access to critical antiseizure medication and/or the treatment required to manage their condition, resulting in significant disparities to epilepsy care in LRC. 20 The World Health Organization (2019) report emphasized the need to prioritize actions that will address the burden of epilepsy. 21 One of the gaps identified is the chronic lack of knowledge and clinical expertise required by healthcare practitioners to accurately assess, treat and provide necessary interventions for people living with epilepsy in LRC. 21
Barriers to epilepsy treatment include perceived cultural and superstitious causes; including spread of myths that epilepsy is caused by spirits or the consequence of a wrong action like infidelity to one's spouse. 22 Unfortunately, these misconceptions abound and impact negatively in the care people with epilepsy received in LRC.
In 2020 the World Health Organization adopted the Intersectoral Global Action Plan (IGAP) on epilepsy and other neurological conditions. The International Bureau for Epilepsy and the International League Against Epilepsy jointly advocated for a meaningful action plan. IGAP is now what is known as the 90-80-70 goal to improve epilepsy care globally 23 (Table 1).
Goals to Improve Epilepsy Care Globally. 23
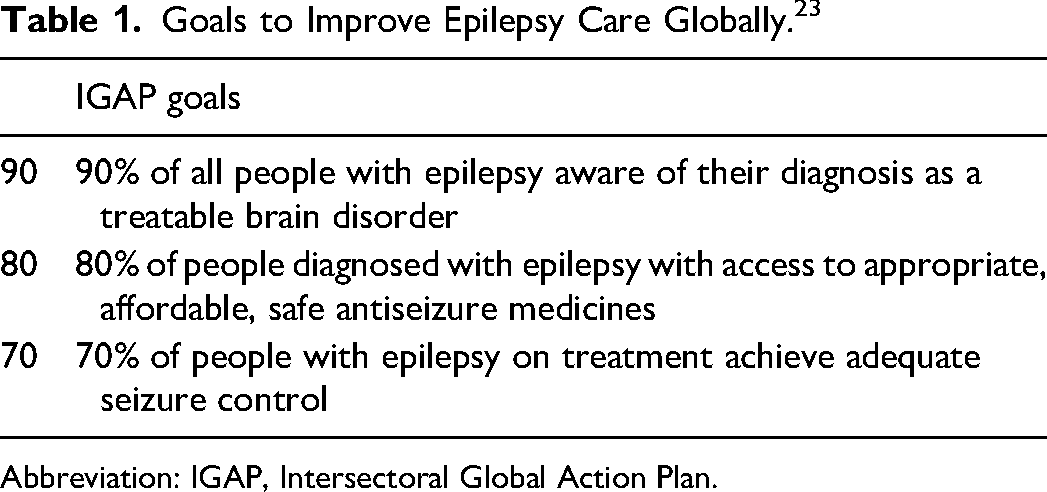
Abbreviation: IGAP, Intersectoral Global Action Plan.
To address disparities and improve care delivery for people with epilepsy in LRC, it is important that healthcare professionals have the knowledge, skills and experience required to assess, diagnose, treat and manage epilepsy appropriately. One of the major barriers to education of healthcare professionals in LRC is financial barriers; most clinicians cannot afford to pay for specialist training to increase their knowledge and skills in epilepsy care. 24
Global Solutions
In 2021, Pretola Global Health started a free virtual annual training for clinicians in LRC, the Epilepsy Assessment and Management Course (EAMC). This training covers 19 topics over a period of 3 months. Teaching sessions were delivered virtually by epilepsy specialists including neurologists, epilepsy specialist nurses, neuropsychologists, neuropsychiatrists and people with lived experiences. Participants registered for the training at no financial costs to them.
Over a period of 3 years, there's been a significant increase in the demand and registration of healthcare professionals for the training. The first edition of the EAMC was held in 2021 with 54 clinicians from 12 countries. In 2024, there were 720 clinicians from 55 countries and 5 continents that attended the fifth edition of the training. This significant increase reflects the need and desire to learn and improve epilepsy care delivery. Feedback received from participants was positive and indicated an increase in awareness, knowledge, and skills to support people with epilepsy in their clinics and communities.
These efforts should be replicated in more areas and could be applied to rural communities in the United States as well if we combined forces and worked together.
Conclusion
Health disparities in epilepsy care remain a global challenge, affecting minoritized communities in the United States and individuals in low-resource countries disproportionately. Factors such as socioeconomic status, immigration status, language barriers, and geographical location, among others, contribute significantly to these inequities. Addressing these challenges requires a multifaceted approach at individual, institutional, and governmental levels.
Nationally, efforts to reduce disparities must include frameworks that address social determinants of health, improve access to specialized care, and expand culturally and linguistically appropriate services. Programs like the Spanish Epilepsy Clinic in Chicago demonstrate how targeted interventions can provide more equitable care, build trust, and improve outcomes for underserved populations.
Globally, initiatives like the Epilepsy Assessment and Management Course (EAMC) highlight the importance of education and collaboration in reducing the epilepsy treatment gap. These programs underscore the value of empowering healthcare professionals with the necessary skills and resources to provide effective care, even in resource-limited settings.
Ultimately, achieving equity in epilepsy care will require sustained commitment from all stakeholders. By fostering collaboration among providers nationally and globally, advocating for systemic changes, and leveraging innovative solutions, we can move closer to the goal of high-quality, accessible epilepsy care for all individuals.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.