
Abstract
Lawn ND, Pang EW, Lee J, Dunne JW. Epilepsia. 2023;64(10):2714-2724. doi:10.1111/epi.17712
Patients with a first-ever unprovoked seizure commonly have subsequent seizures and identifying predictors of recurrence has important management implications. Both prior brain insult and epileptiform abnormalities on electroencephalography (EEG) are established predictors of seizure recurrence. Some studies suggest that a first-ever seizure from sleep has a higher likelihood of recurrence. However, with relatively small numbers and inconsistent definitions, more data are required. Prospective cohort study of adults with first-ever unprovoked seizure seen by a hospital-based first seizure service between 2000 and 2015. Clinical features and outcomes of first-ever seizure from sleep and while awake were compared. First-ever unprovoked seizure occurred during sleep in 298 of 1312 patients (23%), in whom the 1-year cumulative risk of recurrence was 56.9% (95% confidence interval [CI] 51.3-62.6) compared to 44.2% (95% CI 41.1-47.3, p < .0001) for patients with first-ever seizure while awake. First-ever seizure from sleep was an independent predictor of seizure recurrence, with a hazard ratio [HR] of 1.44 (95% CI 1.23-1.69), similar to epileptiform abnormalities on EEG (HR 1.48, 95% CI 1.24-1.76) and remote symptomatic etiology (HR 1.47, 95% CI 1.27-1.71). HR for recurrence in patients without either epileptiform abnormalities or remote symptomatic etiology was 1.97 (95% CI 1.60-2.44) for a sleep seizure compared to an awake seizure. For first seizure from sleep, 76% of second seizures also arose from sleep (p < .0001), with 65% of third seizures (p < .0001) also from sleep. Seizures from sleep were less likely to be associated with injury other than orolingual trauma, both with the presenting seizure (9.4% vs 30.6%, p < .0001) and first recurrence (7.5% vs 16.3%, p = .001). First-ever unprovoked seizures from sleep are more likely to recur, independent of other risk factors, with recurrences also usually from sleep, and with a lower risk of seizure-related injury. These findings may inform treatment decisions and counseling after first-ever seizure.Objectives:
Methods:
Results:
Significance:
Commentary
Approximately 1 in 10 people worldwide have a first seizure in their lifetime. 1 First seizure patients make up a unique cohort that includes those with provoked seizures with a low risk of recurrence and patients with unprovoked seizures who are likely to go on to develop epilepsy. The first seizure can be a frightening, life-changing experience for the patients and their families. They would want to know their risk of recurrence since the likelihood of recurrence has profound psychosocial and financial implications. Besides, individual risk prognostication is critical in predicting patient outcomes and guiding treatment decisions.
The practical clinical definition of epilepsy proposed in the 2014 International League Against Epilepsy official report includes patients with a single unprovoked seizure if the risk of recurrence is at least 60% over the following 10 years. 2 This definition has brought up the question as to whether some risk factors for seizure recurrence after a first seizure are strong enough to allow for the diagnosis of epilepsy. The 2015 American Academy of Neurology (AAN) guideline identified 4 clinical factors with the highest risk of recurrence: remote symptomatic seizures (Level A), epileptiform abnormalities (Level A), a significant brain imaging abnormality (Level B), and a nocturnal seizure (Level B). 3 However, the decision to diagnose epilepsy or initiate anti-seizure medication (ASM) therapy following a single unprovoked seizure can be complex since it can be affected by several factors beyond these risk factors (Figure 1). 4
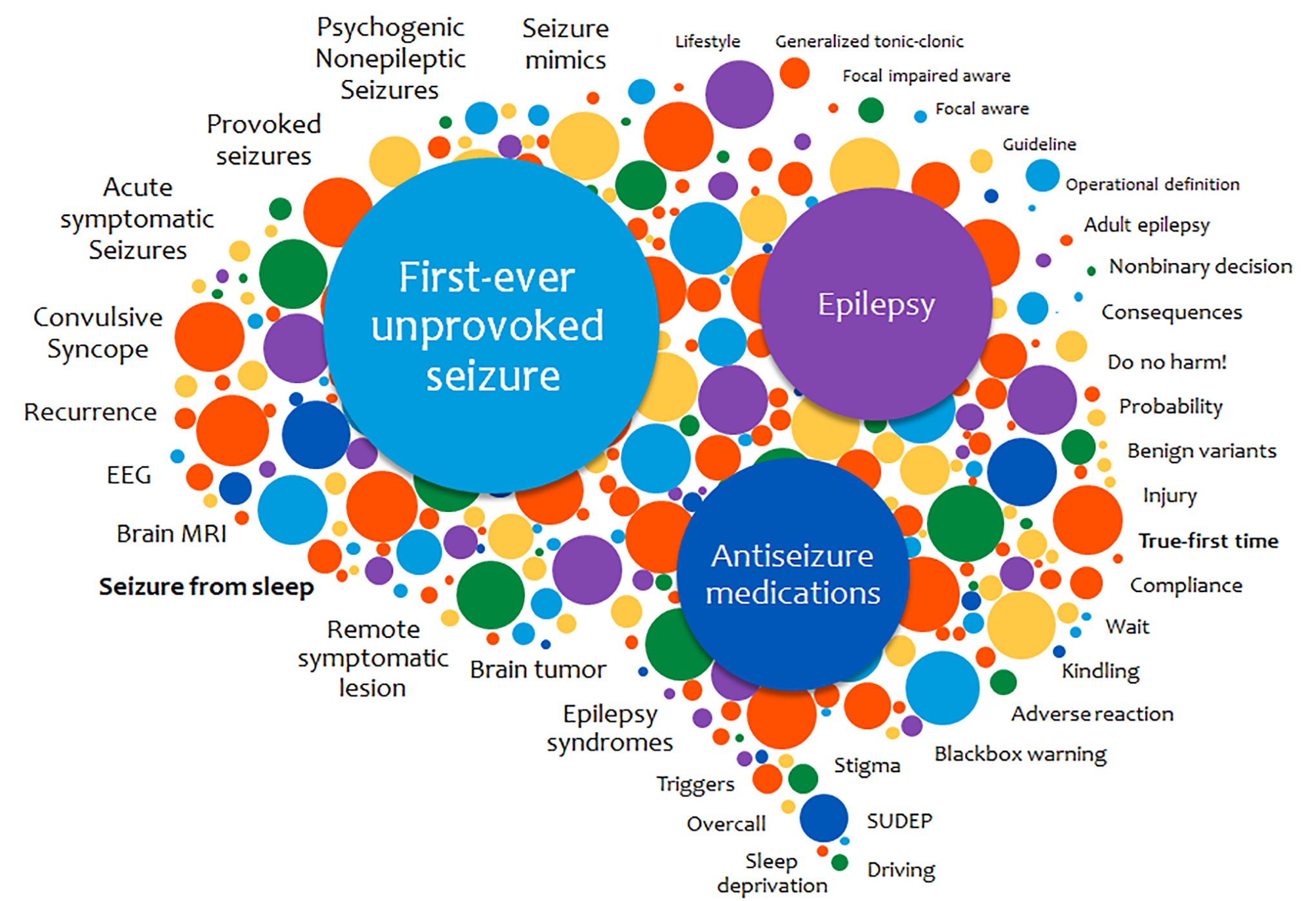
Factors potentially impacting decisions in patients with first-ever unprovoked seizure. Modified and used with permission from Feyissa and Cascino 4 with permission of Elsevier, all rights reserved. EEG indicates electroencephalogram; MRI, magnetic resonance imaging; SUDEP, sudden unexpected death in epilepsy.
The AAN guideline recommendation regarding sleep as a risk factor for recurrence comes from 2 prior older studies. These studies looked at nocturnal seizures, defined as seizures occurring between midnight and 9
Of 1312 adults, almost a quarter (298) had a first seizure from sleep. Seizures from sleep were a strong predictor of recurrence with a hazard ratio of 1.44, on par with epileptiform abnormalities and remote symptomatic etiology. Compared to those who had seizures from wakefulness, this population had a higher rate of recurrence, with a 1-year risk of 57% and a 10-year risk of 77.5%. Of those who had a recurrence, the majority had their second (76%) and third seizure (65%) also from sleep. The seizure from the sleep group was less likely to have seizure-related injury other than orolingual trauma, both with the first seizure and the first recurrence. Besides, the 1-year mortality was slightly lower at 1-year in the sleep seizure group, but not subsequently, and there was no difference in the rate of sudden unexpected death in epilepsy. Interestingly, immediate ASM treatment was commenced in about a quarter of patients for both seizures from sleep and awake groups with a similar rate of recurrence (72% vs 78%).
The current study’s findings have several practical implications. First, the study provides strong evidence for the first-ever unprovoked seizure from sleep as a predictor for seizure recurrence, with a larger sample size and longer follow-up than previously. This information allows us to confidently counsel our patients that with the first seizure from sleep, there is a much higher chance of seizure recurrence (i.e., epilepsy) regardless of the presence of other risk factors. However, we must balance the increased risk of recurrence with the knowledge that the second and third seizures, if they occur, will also most likely occur in sleep and are associated with a lower risk of seizure-related injury.
Second, the association between sleep state and recurrence risk suggests that seizures in sleep may differ from those during wakefulness and be more likely to recur. The finding that the sleep state at the time of the first seizure was correlated with the sleep state at the time of recurrence may relate to enhanced cortical network synchrony during non-rapid eye-movement (NREM) sleep or changes in neurotransmitters during sleep. 8 Indeed, it is well-known that interictal spikes are most frequent in N3 sleep, while sleep-related seizures most frequently arise from N1 or N2 NREM sleep stages. 8
Third, for those with the first seizure from sleep, it is crucial to determine the risk of awake seizures during activities such as working with heavy machinery and driving. In the first-ever seizure from sleep, the monthly risk of recurrent awake seizure decreased consistently below 1.7% (20% per annum), typically used as an arbitrarily accepted risk for private motor vehicles in some countries, 9 only after 5 months had passed. This suggests a cautious requirement of a seizure-free period of at least 6 months before returning to driving after the first-ever seizure from asleep.
Finally, despite the immediate initiation of ASM therapy in about a quarter of the study cohort, the majority of the treated patients still had seizure recurrence. Those with the first seizure from sleep were at a lower risk of having an injury from recurrences, and recurrences were more likely to occur from sleep. These observations support considering a conservative approach before initiating ASM therapy in patients after their first-ever seizure, 4 even so for those with their first seizure from sleep.
The study suffers from the typical limitations of all first seizure studies. The reported first seizure event may not be truly the first-ever seizure. Indeed, a substantial proportion of individuals with a “first” bilateral tonic–clonic seizure report prior seizures. 10 This is true more so for patients with the first seizure from sleep because there may be delays in diagnosis or misdiagnosis as parasomnias. Second, the median time from the first seizure to review in the study was 41 days. This may have influenced the identification of early seizure recurrence. Curiously, the study did not examine the role of obstructive sleep apnea in patients with seizures predominantly arising from sleep. Significantly, the study did not answer whether and how the established 4 risk factors for recurrence can be tallied when and if they co-occur in an individual patient to determine the aggregate risk for recurrence.
Despite its limitations, the present study has demonstrated that first-ever unprovoked seizures from sleep in adults are more likely to recur, independent of other risk factors, with recurrences also usually from sleep and a lower risk of seizure-related injury. While the observed association between sleep state and recurrence risk underscores the role of sleep in modulating cerebral activity, more studies are needed to elucidate the precise relationship between sleep state and recurrence risk. Such studies will provide insights into the pathophysiology of the first-ever unprovoked seizure and the mechanisms that underlie the transition into epilepsy, ultimately improving our ability to provide a concrete management plan to calm our patients’ fear. In the meantime, the decision to diagnose epilepsy or initiate ASM therapy immediately following a first-ever unprovoked seizure, awake or sleep, needs to be individualized.