
Abstract
Tarrada A, Aron O, Vignal JP, Ertan D, Maillard L, Hingray C. Epilepsia. 2022;63(5):1130-1140. doi:10.1111/epi.17215. Anxiety disorders are a frequent psychiatric condition in patients with epilepsy. Anticipatory anxiety of seizures (AAS) is described as a daily persistent fear or excessive worry of having a seizure. AAS seems to be related to “subjective ictal anxiety” reported by patients. The current study aimed to assess the association between objective ictal features and the presence of AAS. Ninety-one patients with drug-resistant focal epilepsy underwent a standardized psychiatric assessment, specific for epilepsy, and presurgical long-term video-electroencephalography (EEG) or stereo-EEG (SEEG). We compared seizure semiology and epilepsy features of patients with AAS (n = 41) to those of patients without AAS (n = 50). We analyzed emotional and motor behavior ictal signs as well as ictal consciousness. We further assessed amygdala ictal involvement in seizures recorded with SEEG (n = 28). AAS was significantly associated with the presence of ictal emotional distress; negative emotional behavior (P < .01) and negative emotion were explicitly reported to the examiner during recording (P = .015), regardless of the ictal level of consciousness. Among the patients recorded with SEEG, we found a significant involvement of amygdala within the seizure onset zone (P < .01) for patients with AAS. Higher risk of developing AAS is associated with seizures expressing negative emotional symptoms, independently of ictal consciousness level. Persistent interictal fear of seizures might be viewed as the consequence of a reinforcement of the emotional networks secondary to amygdala involvement in seizures of temporal origin. Physicians should screen for AAS not only to assess the impact of epilepsy on daily life, but also as an interictal biomarker of ictal semiology and emotional network involvement at seizure onset.Objective:
Methods:
Results:
Significance:
Commentary
Psychiatric comorbidities are not only highly prevalent among people with epilepsy, but some psychiatric symptoms have a direct relationship to seizures and epilepsy itself. This direct relation between seizures and psychiatric symptoms is exemplified by peri-ictal psychiatric symptoms, which have a temporal relationship to seizures. 1 Pre-ictal symptoms precede seizures by up to 3 days and have variable duration; ictal symptoms are a brief, direct manifestation of seizure activity; and post-ictal symptoms begin after a seizure (usually hours to a few days after recovery from a seizure or cluster of seizures). Anxiety is arguably the most common type of psychiatric comorbidity among people with epilepsy and potentially the most complex, ranging from peri-ictal symptoms to epilepsy-specific anxieties to classical anxiety disorders described in the Diagnostic and Statistical Manual of Mental Disorders (DSM). The spectrum of peri-ictal and interictal anxieties in epilepsy is outlined in the recent framework proposed by Hingray and colleagues, 2 and summarized in Table 1. Anticipatory anxiety of seizures (AAS) is an epilepsy-specific anxiety concept stemming from the earlier concept of seizure fear. 3 AAS is characterized by excessive, anticipatory fear of having a seizure 2 and has been the topic of multiple recent investigations.
Major Categories of Peri-Ictal and Interictal Anxieties in Epilepsy.
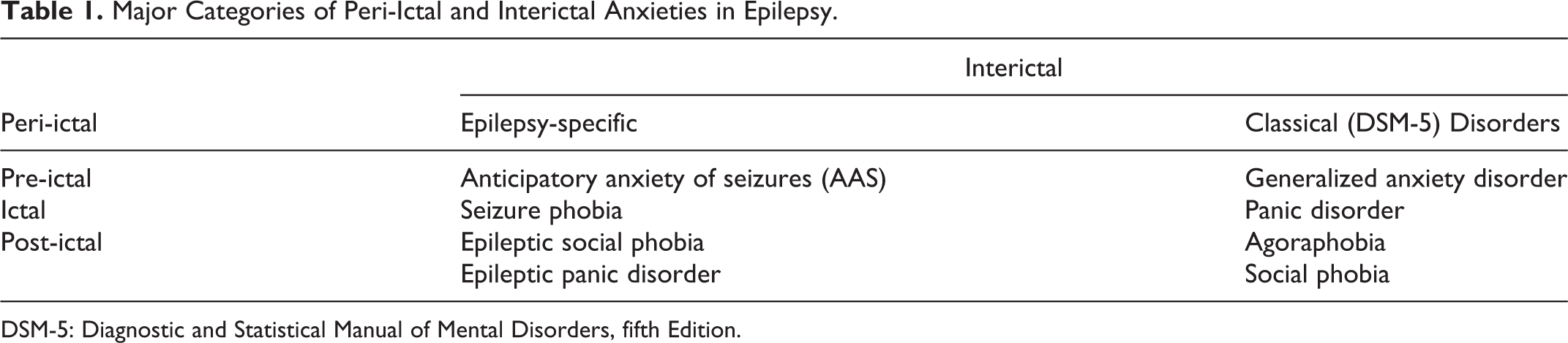
DSM-5: Diagnostic and Statistical Manual of Mental Disorders, fifth Edition.
Published research demonstrates a link between ictal anxiety and interictal psychopathology. Associations of anxiety symptoms with structural imaging abnormalities of mesial temporal structures including the amygdala have been documented. 4 -6 However, similar investigation of epilepsy-specific interictal anxieties including AAS is novel. Likewise, epilepsy-specific interictal anxieties have not been examined for association with seizure onset localization on intracranial EEG, and there is a paucity of literature overall examining interictal anxieties and intracranial EEG-based seizure onset localization.
In response, Tarrada and colleagues evaluate the relation between anticipatory anxiety of seizures and multiple dimensions of ictal phenomena: subjective ictal anxiety reported by participants retrospectively in the interictal period, objective ictal features observed on video, and location of seizure onset among 3 specific areas of interest investigated via stereo-EEG. 7 The findings build on the group’s prior work demonstrating an association between subjective experience of anxiety during seizures and AAS 8 to now demonstrate independent association of AAS with subjective ictal anxiety and objective negative emotional behavior on ictal video recording. Interictal generalized anxiety, measured by the Generalized Anxiety Disorder-7 (GAD-7), and shorter duration of epilepsy were also independently associated with presence of AAS. 7
Among 28 individuals who had stereo-EEG data available, considering the 3 regions of interest determined a priori (amydgala, insula, and orbitofrontal gyri), all 11 individuals with anticipatory anxiety of seizures had amygdala involvement in seizures, and 91% of these had seizure onset in the amygdala, compared to 41% in the non-AAS group. This finding was statistically significant, with a strong effect size. There were no statistically significant associations with regard to insula or orbitofrontal involvement, though only 11/28 participants with stereo-EEG data available had orbitofrontal electrode coverage. 7
While these findings are interesting and may suggest a role for anxiety symptoms as not only a comorbidity, but also a seizure localizing feature, this work is limited by the small, single center sample and bias in electrode sampling locations based on temporal lobe hypotheses for the seizure onset zone. Likewise, the assessment of AAS was done using a single question developed by the authors of this study, as there are currently no established diagnostic criteria for AAS. Although AAS is the most well-studied epilepsy-specific interictal anxiety, literature on this clinical concept remains limited to date, and further work is needed, including better development and testing of methods for identifying AAS.
Nevertheless, this work raises interesting questions about the spectrum of peri-ictal to interictal anxiety symptoms and documents a potential link between peri-ictal phenomena, epilepsy-specific anxieties, and more general interictal anxieties such as those captured by the commonly used screening instruments such as the GAD-7. While the mainstay of management for peri-ictal psychiatric symptoms (and in particular peri-ictal anxiety) is seizure control, typically management of interictal anxiety is similar to DSM anxiety disorder management in the general population. The results of the study by Tarrada and colleagues link anticipatory anxiety of seizures closely to ictal anxiety, raising potential questions about whether AAS and other epilepsy-specific interictal anxieties should have distinct management approaches from those used for the classical DSM-defined interictal anxiety disorders.
Future work should examine the relation between anticipatory anxiety of seizures and seizure-focused management approaches. It may be that some epilepsy-specific forms of interictal anxiety such as AAS respond to strategies focused on seizure management. Identifying whether an interictal anxiety is epilepsy-specific thus may be beneficial for effective management of these comorbidities. Recently developed epilepsy-specific anxiety screening tools, the Epilepsy Anxiety Survey Instrument (EASI) and its brief version, the brEASI, include items addressing epilepsy-specific anxieties 9 and may enhance anxiety characterization and management in epilepsy clinics. Further, individuals with ictal anxiety appear to be at risk for anticipatory anxiety of seizures and potentially should be screened specifically for AAS. Screening for AAS could be accomplished using the question employed in the Tarrada et al. study: “In your everyday life, are you afraid of having an epileptic seizure?” 7
Finally, the work by Tarrada et al. suggests that presence of AAS may have specific localizing value for seizure onset, further supporting the importance of identifying AAS in people with epilepsy, not only to treat a comorbidity, but to potentially benefit management of the epilepsy itself. This may be especially important among those with drug-resistant epilepsy, in which specific localization is essential for pursuing highly effective surgical epilepsy therapies. Other psychiatric symptom categories outside of anxiety may demonstrate similar value in localization, and work is underway, including a recent publication by Soncin and colleagues 10 demonstrating worse right temporal and orbitofrontal PET hypometabolism in individuals with interictal and peri-ictal post-traumatic stress symptoms, compared to those with temporal lobe epilepsy and no post-traumatic stress. Future research should further examine whether various epilepsy-specific psychiatric phenomena may have value for seizure focus localization on intracranial EEG, to expand on the work by Tarrada et al. and better clarify when psychiatric phenomena should be managed as inherent to the epilepsy, vs as a comorbidity.