
Abstract
Implantable devices for controlling medically intractable seizures nondestructively are rapidly advancing. These offer reversible, potentially, restorative options beyond traditional, surgical procedures, which rely, largely on resection or ablation of selected brain sites. Several lines of, investigation aimed at improving efficacy of these devices are discussed, ranging from identifying novel subcortical, white matter, or cell-type specific targets to engineering advances for adaptive techniques based- on continuous, dynamic system analysis.
Keywords
Treatments for pharmacoresistant epilepsy syndromes have largely focused on nonreversible surgical intervention, such as focal brain resection, ablation, or structural disconnection. The goal of reducing morbidity and creating nondestructive, reversible therapies has led to a series of implantable devices that deliver physiologically inspired electrical signals directly to the brain. 1 These have a history extending across decades, including stimulators targeting the cerebellum, left vagus nerve, and trigeminal nerve. These provide a much needed therapeutic alternative especially for patients facing a high risk of adverse cognitive effects from destructive therapy. The recent approvals of two new implantable devices, which have already become mainstays of epilepsy treatment, have helped to spur new progress in the field. These are the responsive neural stimulator (RNS; Neuropace Inc), which targets selected cortical or subcortical sites with tailored permanent electrode implants, and the Medtronic deep brain stimulation (DBS) device targeting the anterior nucleus of the thalamus (Medtronic Inc). As yet, however, the modest seizure-free rates achieved by these devices cannot match the benefits of traditional brain resection. Additionally, therapy optimization is a time-consuming process that may extend into periods of years, thus delaying clinical benefit. However, there is hope that these gaps may eventually close.
In a series of lectures presented at the Merritt-Putnam Symposium in the 2020 American Epilepsy Society Annual Meeting, three general investigative approaches to device efficacy were described: addressing network interactions inherent in focal epilepsies, identifying novel stimulation paradigms and targets, and expansion of device capabilities to permit dynamic adaptation in response to patient needs.
A Network Approach to Stimulation for Treating Focal Seizures
One approach is to devise a rational, systematic process for determining electrical stimulation parameters. Current strategies for generating DBS protocols utilized in both clinical and research applications have been largely empirical, in which a particular starting point for stimulation protocols is established ad hoc and then tweaked to improve efficacy. The parameter space for stimulation can be quite large: stimulation amplitude, duration, frequency, locations, and so on, can all be varied and used in unique combinations. Given this, such improvised modifications can be inefficient. In addition to complications associated with neuronal diversity and differing responses to stimulation parameters, we believe that there are at least two specific root causes for this state of affairs. First, stimulation protocols generally do not reflect the real-time dynamics of the brain’s electrical state. Although some attempts at modulating the time of stimulation are being employed to improve the responsiveness of stimulation, the stimulation paradigm itself is still largely predetermined. Second, there is increasing evidence that the neural network circuitry that contributes to epileptic seizures in many cases may extend well beyond the designated focal region 2 into other parts of the brain.
Dynamical analysis of endogenous neural coherence at multiple sites in the epileptic rat brain has been used to develop subject-specific DBS protocols that may lead to improved seizure control. A personalized form of DBS using dynamical biomarkers was used successfully to terminate seizures in a chronic rat model of temporal lobe epilepsy (TLE). 3 Periods of significant change in multisite coherence occurred coincident with the time of seizure onset, and a different but related dynamic was seen at natural seizure termination.4,5 Similar types of dynamics were also observed in depth recordings from patients with TLE. 6 These dynamics could significantly vary between rodent subjects but be stable in time over many months. When DBS was applied at the locations and frequencies where high synchronization occurred at the time of natural seizure termination for that specific animal, exogenous stimulation could abruptly terminate a seizure significantly faster than stimulation that was not tailored to the subject. 3 These and other results 7 provide a pathway of personalizing DBS application tailored for the specific ictal pathology of each patient.
Novel Stimulation Approaches
Low-frequency stimulation (LFS) has been underutilized in epilepsy research but has shown recent promising results. In animal models of limbic and neocortical seizures, LFS of a white matter tract connected with a seizure focus can reduce seizures. In a rat model of TLE, LFS of the dorsal hippocampal commissure at 1 Hz reduced seizures by 90% during the two weeks of stimulation. 8 Seizures continued to be reduced (57%) for two weeks after stimulation suggesting a significant carryover effect. In neocortical epilepsy induced by acute application of 4-aminopyridine in the rat somatosensory cortex, 20 Hz electrical stimulation of callosal fibers that are connected with that seizure focus was effective in reducing seizures. When compared with other neuromodulatory modalities including high-frequency stimulation of the focus or the anterior thalamic nucleus, callosal stimulation was significantly more efficacious in reducing seizures. 9
The above preclinical findings of fiber tract stimulation were translated into a proof-of-principle human trial. 10 In that short-term trial, which was conducted during invasive monitoring in the epilepsy monitoring unit, LFS (5 Hz) of the human dorsal hippocampal commissure reduced temporal lobe seizures by 90%. As this fiber tract is very close to the posterior arching fornices, the target was termed the fornico-dorso-commissural (FDC) tract. Subsequently, a year-long single-blinded study with implantable pulse generators was done in four individuals with bilateral TLE using chronic 5 Hz electrical stimulation of the FDC. Two subjects became seizure-free, and repeated neuropsychological testing revealed preserved memory.
Although the FDC appears to be a good stimulation target in TLE, the piriform cortex may be an attractive target for neuromodulation regardless of the location of the seizure focus. 11 The piriform cortex is a key structure for epileptogenicity related to chemical, electrical stimulation, kindling, and status epilepticus models in rodents and primates.12,13 It has a role in focal and generalized epilepsy networks 14 and bears some similarities to the hippocampus histologically. In the kainic acid model, a model of severe intractable seizures, LFS of the piriform cortex resulted in almost complete cessation of seizures. 15 In another study, the amplitudes of the evoked responses recorded in the contralateral hippocampus upon stimulation of the piriform cortex appeared to increase after acquisition of epileptogenicity. 16 This amplification may suggest facilitation of interhemispheric seizure propagation pathways which utilize the piriform cortex as a key hub.
Techniques for Basic Science Studies of Targeted Seizure Intervention
Interventions that are highly specific for site and cell type may increase stimulation efficacy while reducing unwanted side effects. Such studies currently require highly specific experimental techniques such as closed-loop, on-demand optogenetics. Studies utilizing on-demand optogenetics have shown that a highly specific intervention, for example, targeting only dentate gyrus granule cells near the seizure focus, 17 can be highly effective for controlling seizures.18,19 On-demand optogenetics can also be applied to areas remote from the site of injury or seizure focus,20,21 including the cerebellum.22-24 Experiments have revealed that excitation, but not inhibition, of the cerebellar fastigial nucleus is able to provide powerful inhibition of temporal lobe seizures, 25 illustrating a benefit of optogenetic-based approaches, and the relatively straightforward control over the direction of modulation they provide. Moreover, selective excitation of only excitatory neurons in the fastigial nucleus provides greater seizure control than an approach that lacks cell-type specificity and broadly excites fastigial neurons. 25 This highlights an important concept: specificity of intervention may not only be important for reducing side effects, it may also be a means to directly improve the efficacy of interventions.
Although the excellent specificity of on-demand optogenetics has several benefits over traditional approaches, it is not currently a clinical option for the epilepsies.19,20,26 Electrical stimulation, however, is. Electrical stimulation of the cerebellum has been previously examined, in both human clinical trials and in a large number of animal studies (reviewed in the study by Streng and Krook-Magnuson, 22 Fountas et al, 27 and Miller 28 ). However, these studies were all done “open loop,” where stimulation was not specifically timed to the seizure event. Additionally, stimulation parameters varied widely, often even within a single study. Therefore, it may be that robust, consistent, seizure inhibition may be possible, if the correct combination of stimulation parameters can be identified. Methods of tailoring closed-loop approaches, 29 such as Bayesian Optimization, may be means to determine which sets of electrical stimulation parameters can be effective, either for an individual or, potentially, for any given stimulation site. Optimization approaches may also help in the making the next generation of implantable systems more individualized and responsive to patients’ needs.
Next-Generation Implantable Systems
To improve the translation of current implantable system technology, several fundamental issues should be resolved. Most existing therapies do not take full advantage of the capability of bioelectronics to dynamically adjust stimulation parameters in response to the patient’s needs. 30 Many predicate algorithms rely on concepts from cardiac pacemakers, even while the underlying physiology is very different. The lack of device responsivity is compounded by the absence of objective, reliable outcome measures. 31 The absence of an immediate physiomarker, unlike the case with movement disorders, can make therapy optimization a long and tortuous process. 32 Although the effectiveness of DBS and RNS for epilepsy is established, it is still an intervention that requires invasive surgery, and fear of complications frightens many patients 33 ; clearly, there is a desire to lower the invasiveness of therapeutic systems. 34 Finally, like pharmaceuticals, the economic incentives of personalized medicine that bioelectronics might enable still needs alignment across health care stakeholders. 35
Including collaborative platforms as part of next-generation systems is a promising route to addressing the challenges and opportunities of bioelectronic medicines, when bridging basic science, advanced technology, and health care economics. 36 Bioelectronic platforms can create a self-reinforcing innovation framework—from designing bespoke, instrumented implantable platforms that enable novel clinical neuroscience, to applying these platforms and the resulting science to prototype new therapies—that can help catalyze new treatments for disease. For example, recent device advances include continuous streaming of brain sensing data that opens a new vista of adaptive therapy applications,37,38 including the application of a distributed brain co-processor providing an intuitive, bidirectional interface between the implanted device, patient, and physician in both canine and human drug-resistant epilepsy. Automated classifiers running on a handheld tablet computer and distributed cloud computing resource provide near-real-time assessment of behavioral state (awake and sleep), interictal epileptiform discharges, and seizures to guide adaptive electrical stimulation. 39 Devices that include recognition of circadian and multidien rhythms are also being explored in research settings 40 ; temporally aware devices provide a mechanism to apply chronotherapy in disease states such as epilepsy where rhythm-specific signatures are being identified with new sensing-enabled devices.41,42
Platform tools like this (Figure 1) are currently enabling new discovery models, aligned with the vision of global activities such as the NIH BRAIN initiative. 43 The breadth of studies reflects the diversity of challenges created by neurological disorders, but also the hope that bioelectronic platforms can help address them.
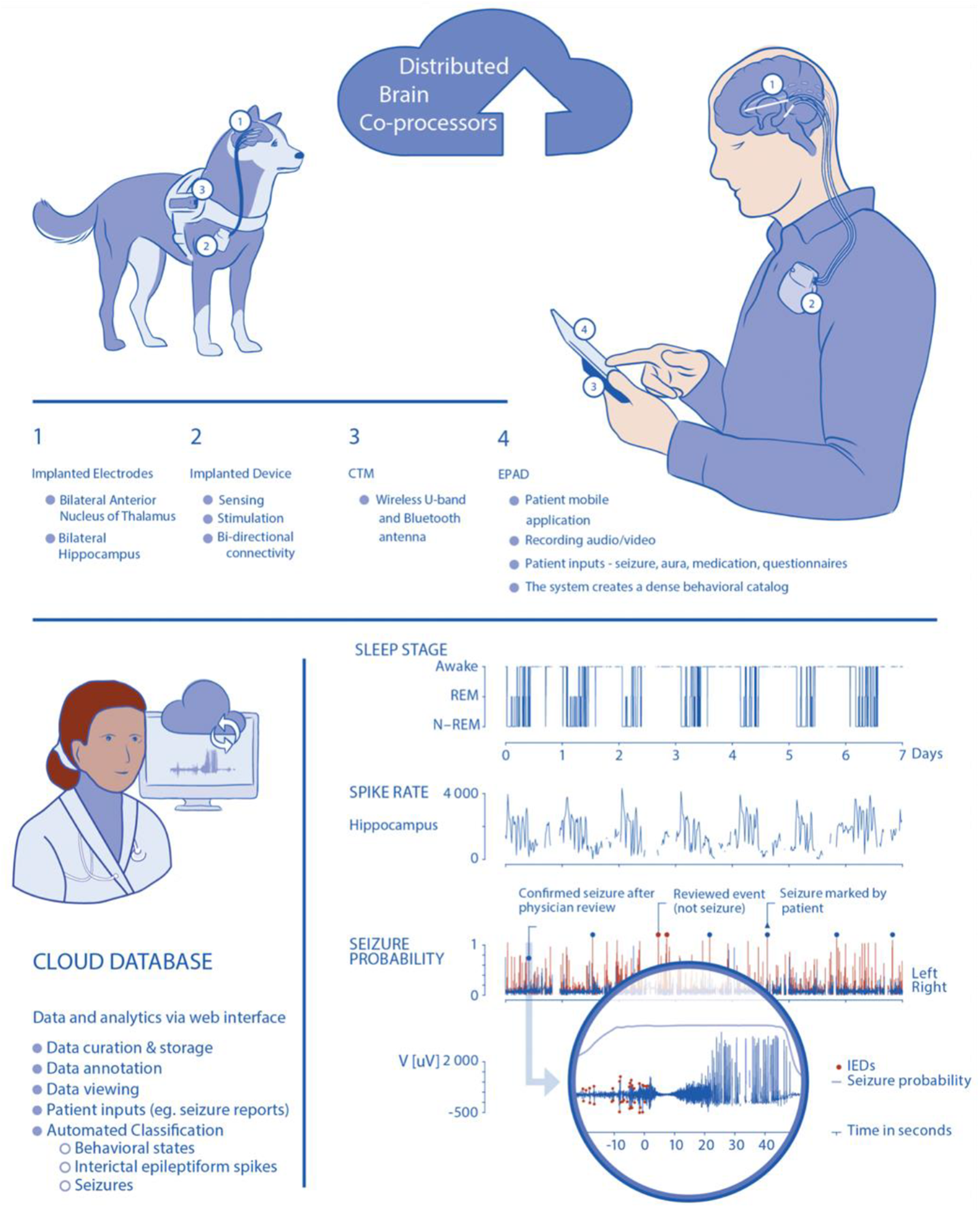
Brain co-processer for integrating implanted sensing and stimulation devices with off-the-body computing resources. The system enables continuous tracking of physiological data coupled with adaptive electrical stimulation. Top) Schematic for bidirectional data transmission between implanted brain sensing and stimulation device integrated with local handheld computer (Epilepsy Patient Assist Device) and cloud environment. The integrated system provides a platform for real-time, continuous, remote ambulatory monitoring physiological data such as brain behavioral state (wake, sleep, and seizures), biomarker (eg, interictal discharges) and behavior (patient inputs, actigraphy, mood, memory), as well as device data (eg, battery status and telemetry). Bottom left) The electrophysiology data are wirelessly telemetered off the implant and processed. Bottom right) Web-based Epilepsy Dashboard enables review of immediate and long-term data trends from the device (eg, battery, electrode impedances), electrophysiology data, and patient inputs. The physician can quickly review and either confirm or reject automatically detected and patient-reported events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Timothy Denison: MRC MC_UU_0003/3; Esther Krook-Magnuson: The Winston and Maxine Wallin Neuroscience Discovery Fund Award, NIH/NINDS R01-NS112518 and NIH R01-NS104071, and the University of Minnesota’s MnDRIVE (Minnesota’s Discovery, Research and Innovation Economy) initiative; David Mogul: NIH/NINDS R01 NS092760; Gregory Worrell: NIH Brain Initiative UH3-NS95495 and NIH/NINDS R01-NS09288203 (Worrell); Catherine Schevon: NIH/NINDS R01 NS084142 and R01 NS110669.