
Abstract
The episodic nature of both epilepsy and psychiatric illnesses suggests that the brain switches between healthy and pathological states. The most obvious example of transitions between network states related to epilepsy is the manifestation of ictal events. In addition to seizures, there are more subtle changes in network communication within and between brain regions, which we propose may contribute to psychiatric illnesses associated with the epilepsies. This review will highlight evidence supporting aberrant network activity associated with epilepsy and the contribution to cognitive impairments and comorbid psychiatric illnesses. Further, we discuss potential mechanisms mediating the network dysfunction associated with comorbidities in epilepsy, including interneuron loss and hypothalamic–pituitary–adrenal axis dysfunction. Conceptually, it is necessary to think beyond ictal activity to appreciate the breadth of network dysfunction contributing to the spectrum of symptoms associated with epilepsy, including psychiatric comorbidities.
Psychiatric Illnesses in Epilepsy
Psychiatric illnesses are highly comorbid in epilepsy, being reported to occur in 25% to 50% of people with epilepsy, 1 a rate higher than the general population or associated with other chronic illnesses. 2 Comorbidities in epilepsy range from depression, anxiety, psychosis, and cognitive impairments, 3 which negatively impact the quality of life of patients. 4,5 Psychiatric comorbidities are more common in patients with poorly controlled seizures 6 and are associated with negative outcomes in people with epilepsy. 7 Interestingly, there appears to be a bidirectional relationship between psychiatric disorders and epilepsy, 8 -10 which has been proposed to involve a shared underlying pathological mechanism and may also involve a pathological process in which psychiatric illness predisposes networks to seizure activity or vice versa.
Psychiatric comorbidities can negatively affect the management of patients with epilepsy, leading to an increased risk of treatment-resistant epilepsy, adverse events associated with antiepileptic drug treatment, stress-triggered seizures, and premature death. 9,11 Thus, psychiatric and behavioral disorders must be properly included in the clinical spectrum of the epilepsies and may help predict outcomes in people with epilepsy. 9,11 The topic of psychiatric comorbidities in the epilepsies has already been comprehensively reviewed by experts in the field. 1 -3,8 -15 The goal of the current review is to provide a new perspective on the role of network dysfunction in contributing to psychiatric comorbidities in epilepsy and discussing network abnormalities associated with both psychiatric illnesses and epilepsy to begin illuminating potential mechanisms contributing to the comorbidity between these disorders.
Aberrant Network Activity and Psychiatric Comorbidities in Epilepsy
In some patients, there is a temporal relationship between ictal events and psychiatric comorbidities. 12 Psychiatric symptoms in epilepsy can manifest as interictal or peri-ictal phenomena and can also result as a side effect of treatment. 12 The temporal association of psychiatric illnesses with ictal activity is varied, as symptom manifestation is associated with the preictal, ictal, and/or the postictal period. The temporal association of psychiatric illnesses with ictal activity suggests a direct relationship between network activity and symptom presentation. However, this relationship is not well understood and is dismissed as a side effect of seizures, but this temporal association may tell us something about the mechanisms mediating the comorbidity between psychiatric illnesses and epilepsy.
Seizures are the most obvious manifestation of a disruption in network activity and are, rightfully, the focus of the majority of studies related to epilepsy. However, more subtle changes in network activity may manifest as psychiatric illnesses and involve dysfunction in similar neuronal networks. 6,16 Thus, network dysfunction may contribute to the shared underlying neurobiology between psychiatric illnesses and epilepsy. This is particularly relevant to temporal lobe epilepsy in which seizures involve brain regions implicated in mood. In fact, psychiatric comorbidities are more common in patients with temporal lobe epilepsy, 13 suggesting that dysfunction in networks implicated in mood may increase vulnerability to psychiatric comorbidities.
The hippocampal circuit receives information from the entorhinal cortex, which enters the hippocampus via the perforant path, synapsing onto dendrites of dentate granule cells. Granule cells, in turn, project to the CA3 via the mossy fiber pathway, and CA3 pyramidal cells project to the CA1 via Schaffer collaterals. CA1 projects back to the subiculum and entorhinal cortex, completing a recurrent circuit. 17 The hippocampal circuitry extends beyond this canonical trisynaptic circuit, 18 which is susceptible to runaway excitation and seizure generation. The hippocampus also plays a well-established role in cognitive function, learning and memory, and spatial navigation. 19 In fact, deficits in hippocampal function associated with epilepsy are proposed to contribute to cognitive impairments comorbid with epilepsy (Figure 1A). 20,21 For example, place cells, which are thought to provide a cognitive map, are unstable in epileptic mice, which is associated with interneuron dysfunction and altered oscillations in the hippocampus. 22,23 In addition, pathological high-frequency oscillations have been observed during interictal periods and negatively impact memory processes. 24 These data demonstrate that network abnormalities in the hippocampus not only contribute to seizure generation but also lead to impairments in hippocampal function critical for cognitive processes. 25
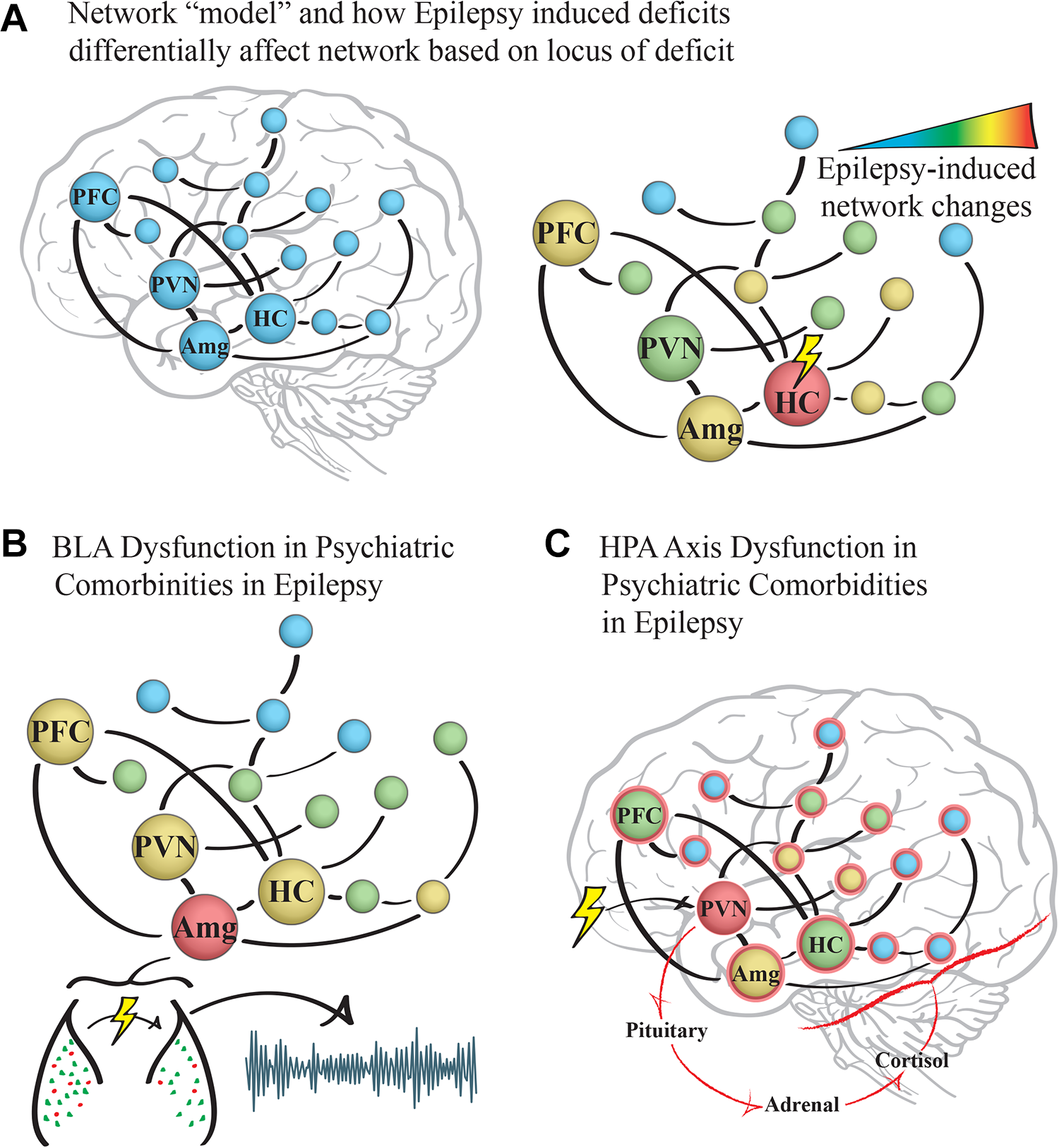
Proposed mechanisms of network dysfunction contributing to psychiatric comorbidities in epilepsy. A, Dysfunction in several brain regions, including the hippocampus (HC), amygdala (Amg), prefrontal cortex (PFC), and paraventricular nucleus of the hypothalamus (PVN), has been observed in association with psychiatric comorbidities in epilepsy. B, Interneuron loss in the amygdala may induce network dysfunction and impair emotional processing, leading to psychiatric comorbidities in epilepsy. C, Network dysfunction in the PVN may cause hypothalamic–pituitary–adrenal (HPA) axis dysfunction, leading to neuroendocrine abnormalities exerting widespread effects contributing to psychiatric comorbidities in epilepsy.
In addition to the role that the hippocampus plays in seizure generation and cognitive impairments associated with epilepsy, hippocampal abnormalities have also been correlated with the severity of depression in patients with temporal lobe epilepsy. 26 Although evidence supporting the relationship between mesial hippocampal sclerosis in epilepsy and comorbid depression has been inconsistent, it has been shown that mesial hippocampal sclerosis is associated with an increased lifetime risk of developing major depressive disorder. 27 Cognitive deficits, associated with hippocampal dysfunction, are also a common feature of the depressed state, and perturbations in cognitive networks have been implicated in comorbid depression and epilepsy. 6,28 Dynamics between the autobiographic memory network, which comprise the prefrontal cortex, cingulate cortex, hippocampus, retrosplenial cortices, precuneus, and parietal regions; and the cognitive control network, which includes the dorsolateral prefrontal cortex, cingulate cortex, mesial temporal lobe, and intraparietal sulcus, are disrupted in depression. 28 Interestingly, epilepsy has also been demonstrated to induce deficits in these networks, 29,30 which may contribute to the high comorbidity of depression and epilepsy as well as cognitive deficits associated with epilepsy.
Further, aberrant network activity in other brain regions has also been implicated in psychiatric comorbidities associated with epilepsy (Figure 1A). Patients with temporal lobe epilepsy, 31 including those presenting with comorbid depression, 32 exhibited decreased connectivity in the limbic-frontal network, consistent with the limbic-frontal network dysfunction hypothesis of depression. 33 People with epilepsy presenting with comorbid depression have also been shown to have hypometabolism in the frontal cortex. 34,35 Network abnormalities within discrete brain regions (microcircuit) can induce dysfunction in distributed networks (macrocircuit), both of which could potentially contribute to comorbid psychiatric illnesses and epilepsy.
We can combine our understanding of the function of specific brain regions and networks with abnormalities identified in association with epilepsy to extrapolate to the potential relevance to psychiatric comorbidities in epilepsy. For instance, the amygdala is known to play a critical role in emotional processing 36 and is therefore highly relevant to psychiatric disorders, particularly anxiety and depression. The amygdala is connected to brain regions involved in emotional processing, including the ventral tegmental area, dorsal and ventral striatum, bed nucleus of the stria terminalis, ventral hippocampus, medial prefrontal cortex, brain stem, and hypothalamus. In patients with temporal lobe epilepsy with amygdala enlargement, the incidence of comorbid depression and epilepsy is substantial (90%). 37 Functional connectivity emanating from the amygdala is altered in patients with temporal lobe epilepsy, which is correlated with psychiatric symptoms. 38 Another study demonstrated that amygdalar volume in people with epilepsy correlates with the core symptoms of dysphoric disorder in epilepsy, including emotional instability, dysphoria, irritability, and aggression, 39 and alteration in the structure of the amygdala has been observed in people with epilepsy and comorbid depression. 40 Although the role of the amygdala in psychiatric comorbidities in epilepsy has received very little attention, this topic was beautifully discussed previously by Kullmann and collectively the data point to a dysregulation in amygdalar function in epilepsy (Figure 1B). 41
These data begin to illuminate dysfunction in neural circuits involved in comorbid depression and epilepsy. However, despite the high incidence of comorbid anxiety and epilepsy, very few studies have focused on network-level changes associated with this comorbidity. Given the importance of the amygdala in the behavioral expression of fear and anxiety, 42 it is likely that these network changes may influence both comorbid anxiety and depression. The suggestion that subtle aberrations in network activity associated with epilepsy may contribute to psychiatric comorbidities may help explain the evidence that psychiatric comorbidities are associated with worse outcomes in epilepsy. 7 This conceptual framework may also explain why psychiatric comorbidities are more common in certain types of epilepsy, such as temporal lobe epilepsy. 13 Additional studies recognizing that psychiatric comorbidities are part of the clinical spectrum of the epilepsies are required to understand the network-level changes associated with the full range of psychiatric comorbidities and epilepsy.
Potential Mechanisms Mediating Aberrant Network Activity Related to Psychiatric Comorbidities in Epilepsy
Neuropsychiatric disorders are increasingly acknowledged to involve altered brain states, 43 and efforts are underway to understand how perturbations in distributed brain areas operating within large-scale networks contribute to psychiatric illnesses. It is interesting to note that similar networks have been implicated across psychiatric disorders. For example, imaging studies identify similar networks disrupted in anxiety and depression, including the prefrontal cortex, amygdala, and insula. 44 In fact, an integrated model of network dysfunction has been proposed to underlie psychopathology. 44 These findings lead us to speculate that network dysfunction in particular regions may lead to a range of psychiatric illnesses, and known risk factors may increase vulnerability through corruption of these networks. Consistent with this notion, there are also similar risk factors across psychiatric disorders. For example, previous adverse life events are a major risk factor for anxiety and depression and may contribute to psychiatric illnesses comorbid with epilepsy. 45 Beautiful studies in animal models have elucidated patterns in network communication between the prefrontal cortex, ventral striatum, amygdala, ventral tegmental area, and ventral hippocampus which predict the behavioral changes following chronic social defeat stress, potentially relevant to depression and the interaction between adverse life events (stress) and psychiatric illnesses. 46 Further, combined electroencephalogram and functional magnetic resonance imaging studies demonstrate abnormalities in these networks associated with seizures in patients with epilepsy. 47 The commonality between brain regions implicated across psychiatric illnesses and epilepsy suggest that impairments in these networks may increase vulnerability to both psychiatric disorders and epilepsy and may contribute to their comorbidity.
We are only beginning to understand the mechanisms controlling network activity within networks and communication between networks in the healthy brain, let alone under pathological conditions. Network activity generated within a network, such as oscillations, require interneurons to synchronize neuronal activity. 48 Interestingly, the number of interneurons in the hippocampus and amygdala are decreased both in patients with TLE and in experimental epilepsy models. 49,50 Thus, interneuron loss could contribute to network abnormalities within that specific network that could directly increase vulnerability to psychiatric illnesses (Figure 1B). For example, interneuron loss in the hippocampus has been proposed to impair oscillations in the hippocampus, contributing to a breakdown of spatial coding and cognitive impairments associated with epilepsy. 22,23 In addition, network communication between brain regions also relies on interneuron-driven network synchrony and oscillations, 51 which could become disrupted by interneuron loss in one region and radiate dysfunction throughout the distributed network. For example, interneuron loss in one region, such as the hippocampus or amygdala, could impair network communication with associated regions, such as the prefrontal cortex. Thus, a disruption in network activity in one region could have a ripple effect, impacting connected regions, which we propose may contribute to psychiatric comorbidities comorbid with epilepsy. It should be noted that numerous additional factors may contribute to network-level changes. Previous publications nicely reviewed potential mechanisms contributing to psychiatric comorbidities in epilepsy, including altered neurotransmitters (glutamate, GABA, and serotonin), hypothalamic–pituitary–adrenal (HPA) axis dysfunction, altered opioid signaling, structural changes, and inflammation. 14,15 It should be noted that these mechanisms are not mutually exclusive, and these potential mechanisms implicated in psychiatric comorbidities may also contribute to the network-level changes summarized in this review. For instance, HPA axis dysfunction is an attractive mechanism linking network abnormalities with psychiatric comorbidities and epilepsy given that hypercortisolism is a hallmark characteristic of depression and stress hormone levels are altered in people with epilepsy. 52 Furthermore, stress is a major risk factor for both epilepsy and depression. 52 In animal models, corticosterone levels are elevated in chronically epileptic mice exhibiting depression-like behaviors, 53 -55 and blunted activation of the HPA axis improves outcomes in epilepsy including decreased comorbid depression-like behaviors. 56 Neuroendocrine changes, such as elevated levels of stress hormones, have the ability to exert widespread impacts throughout the brain, particularly in limbic regions expressing high levels of mineralocorticoid and glucocorticoid receptors 57,58 including the hippocampus and amygdala. In fact, glucocorticoid signaling has been shown to increase neuronal excitability in the hippocampus, 57,58 which likely alters network activity and has the potential to negatively impact both epilepsy and psychiatric comorbidities. In this way, HPA axis dysfunction could exert widespread effects on networks implicated in mood, potentially altering network activity and contributing to psychiatric comorbidities in epilepsy. In addition, the paraventricular nucleus of the hypothalamus which governs the HPA axis and the physiological response to stress are regulated by the hippocampus and amygdala (Figure 1C). Therefore, there may be a bidirectional interaction in which network dysfunction could induce HPA axis abnormalities and vice versa. Additional studies are required to elucidate the mechanisms contributing to psychiatric comorbidities in epilepsy and appreciate the contribution of network dysfunction in the manifestation of these comorbidities.
Conclusions
Epilepsy is a network disorder characterized by remarkable changes in neuronal activity. Accumulating evidence also suggests that psychiatric disorders involve network-level changes in brain states. Emerging evidence suggests that network-level changes are associated with psychiatric illnesses in epilepsy. The majority of studies investigating network changes in epilepsy have focused on the generation of ictal activity. However, it is important to recognize that subtle, but potentially widespread, network dysfunction may also contribute to psychiatric comorbidities associated with epilepsy. Further studies are required to fully appreciate the role of network abnormalities in mediating the bidirectional relationship between psychiatric illnesses and epilepsy.
Highlights
Psychiatric illnesses are commonly comorbid with epilepsy.
Epilepsy is a network disorder.
Seizures are the most obvious manifestation of network dysfunction in epilepsy.
Network dysfunction may also contribute to psychiatric comorbidities in epilepsy.
The structure of the amygdala is disrupted in epilepsy, which may contribute to psychiatric comorbidities in epilepsy.
The HPA axis dysfunction may contribute to network disruption and negative outcomes in epilepsy.
Footnotes
Acknowledgments
We appreciate from the references cited the remarkable contributions of dedicated individuals to studying the comorbidity of psychiatric illnesses and epilepsy. Without the contributions of these pioneers, the importance of psychiatric comorbidities in epilepsy would have gone unappreciated. The citation limit prevented me from highlighting all those who have contributed to the field, but I would like to extend my thanks for raising awareness to this important issue.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.M. is a member of the Scientific Advisory Board for SAGE Therapeutics.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: J.M. is supported by R01NS105628, R01NS102937, R01AA026256, and a sponsored research agreement with SAGE Therapeutics.