
Abstract
van Coevorden-Hameete MH, de Bruijn MAAM, de Graaff E, et al. Brain. 2019;142(6):1631-1643. doi:10.1093/brain/awz094. PMID: 31009048. In this study, we report the clinical features of 32 patients with γ-aminobutyric acid B receptor (GABABR) antibodies, identify additional autoantibodies in patients with anti-GABABR encephalitis that mark the presence of an underlying small-cell lung carcinoma and optimize laboratory methods for the detection of GABABR antibodies. Patients (n = 3225) were tested for the presence of GABABR antibodies using cell-based assay, immunohistochemistry, and live hippocampal neurons. Clinical data were obtained retrospectively. Potassium channel tetramerization domain-containing (KCTD)16 antibodies were identified by immunoprecipitation, mass spectrometry analysis and cell-based assays. Potassium channel tetramerization domain containing 16 antibodies were identified in 23 of 32 patients with anti-GABABR encephalitis, and in 1 of 26 patients with small-cell lung carcinoma and Hu antibodies, but not in 329 healthy patients and disease controls. Of the anti-GABABR encephalitis patients who were screened sufficiently, 18 (95%) of 19 patients with KCTD16 antibodies had a tumor versus 3 (33%) of 9 anti-GABABR encephalitis patients without KCTD16 antibodies (P = .001). In most cases, this was a small-cell lung carcinoma. Patients had cognitive or behavioral changes (97%) and prominent seizures (90%). Thirteen (42%) patients developed a refractory status epilepticus with intensive care unit admittance. Strikingly, 4 of 32 patients had a rapidly progressive dementia. The addition of KCTD16 to the GABABR cell-based assay improved sensitivity of the in-house fixed cell-based assay, without loss of specificity. Twenty-two of 26 patients improved (partially) to immunotherapy or chemotherapy. Anti-GABABR encephalitis is a limbic encephalitis with prominent, severe seizures, but patients can also present with rapidly progressive dementia. The co-occurrence of KCTD16 antibodies points toward a paraneoplastic origin. The addition of KCTD16 improves the sensitivity of the cell-based assay.
Commentary
Since its seminal description in the 1960s, 1 the spectrum of limbic encephalitis (LE) has considerably expanded. So has our understanding of its causes, with the establishment of a link with cancer and the identification of onconenural antibodies in the 1990s, followed by the identification of sporadic autoimmune cases and of antibodies to neuronal surface antigens in the 2000s. There are currently more than a dozen antibodies associated with idiopathic and paraneoplastic LE (Table 1). The γ-aminobutyric acid B receptor (GABABR) antibody is a relatively recent addition to this expanding list. With around 150 cases reported prior to this series 2 –11 (Table 2), this entity is rare—approximately 20 times less frequent than the anti-NMDAR syndrome, 2 for instance—although it is likely underdiagnosed.
List of Antibodies Linked With Limbic Encephalitis, With Their Specific Clinical Features and Association With Neoplasms.
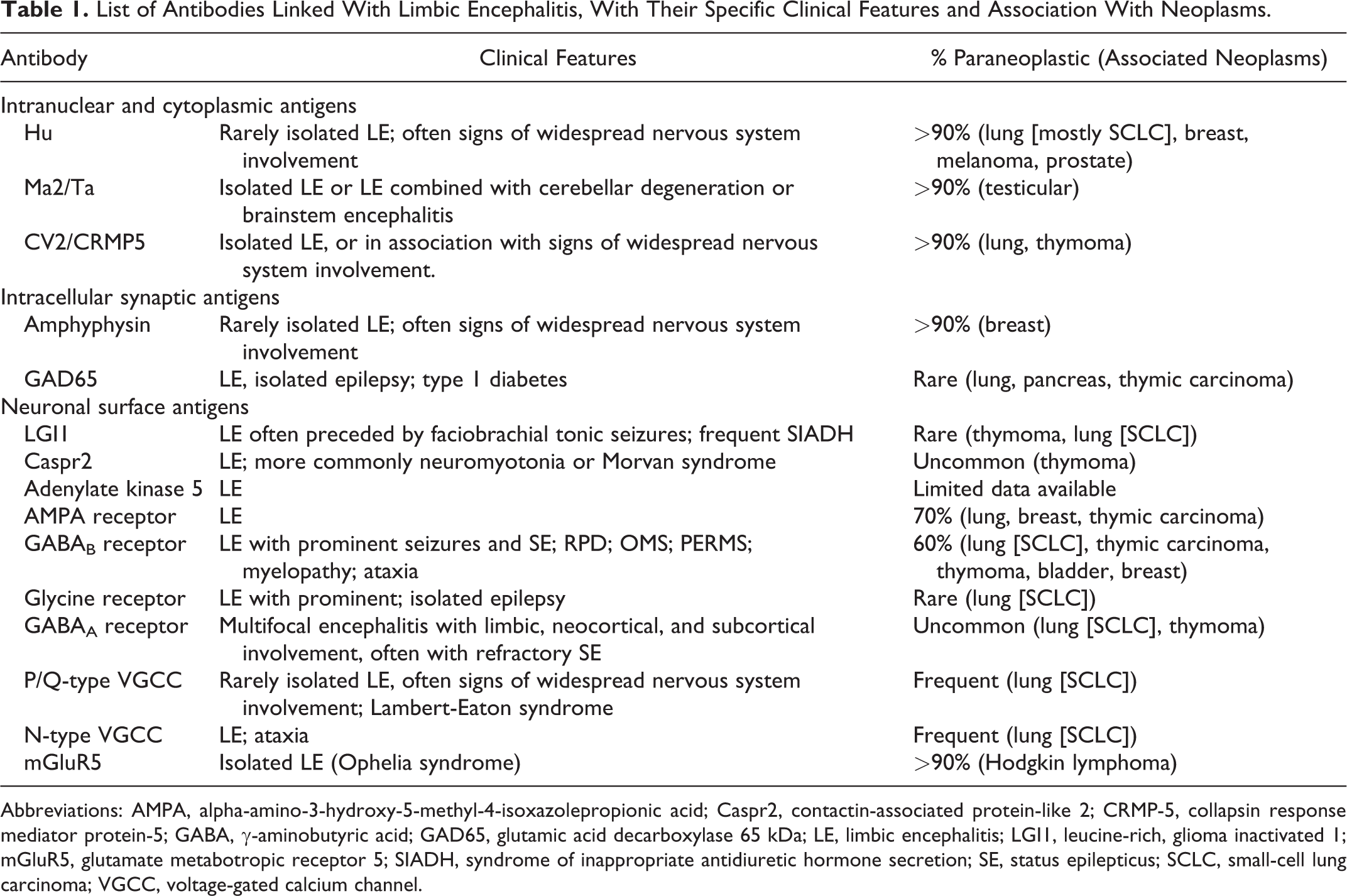
Abbreviations: AMPA, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; Caspr2, contactin-associated protein-like 2; CRMP-5, collapsin response mediator protein-5; GABA, γ-aminobutyric acid; GAD65, glutamic acid decarboxylase 65 kDa; LE, limbic encephalitis; LGI1, leucine-rich, glioma inactivated 1; mGluR5, glutamate metabotropic receptor 5; SIADH, syndrome of inappropriate antidiuretic hormone secretion; SE, status epilepticus; SCLC, small-cell lung carcinoma; VGCC, voltage-gated calcium channel.
Summary of Clinical and Paraclinical Findings in Cases of GABABR Antibody-Associated Limbic Encephalitis Reported in Large (N > 5) Case Series.
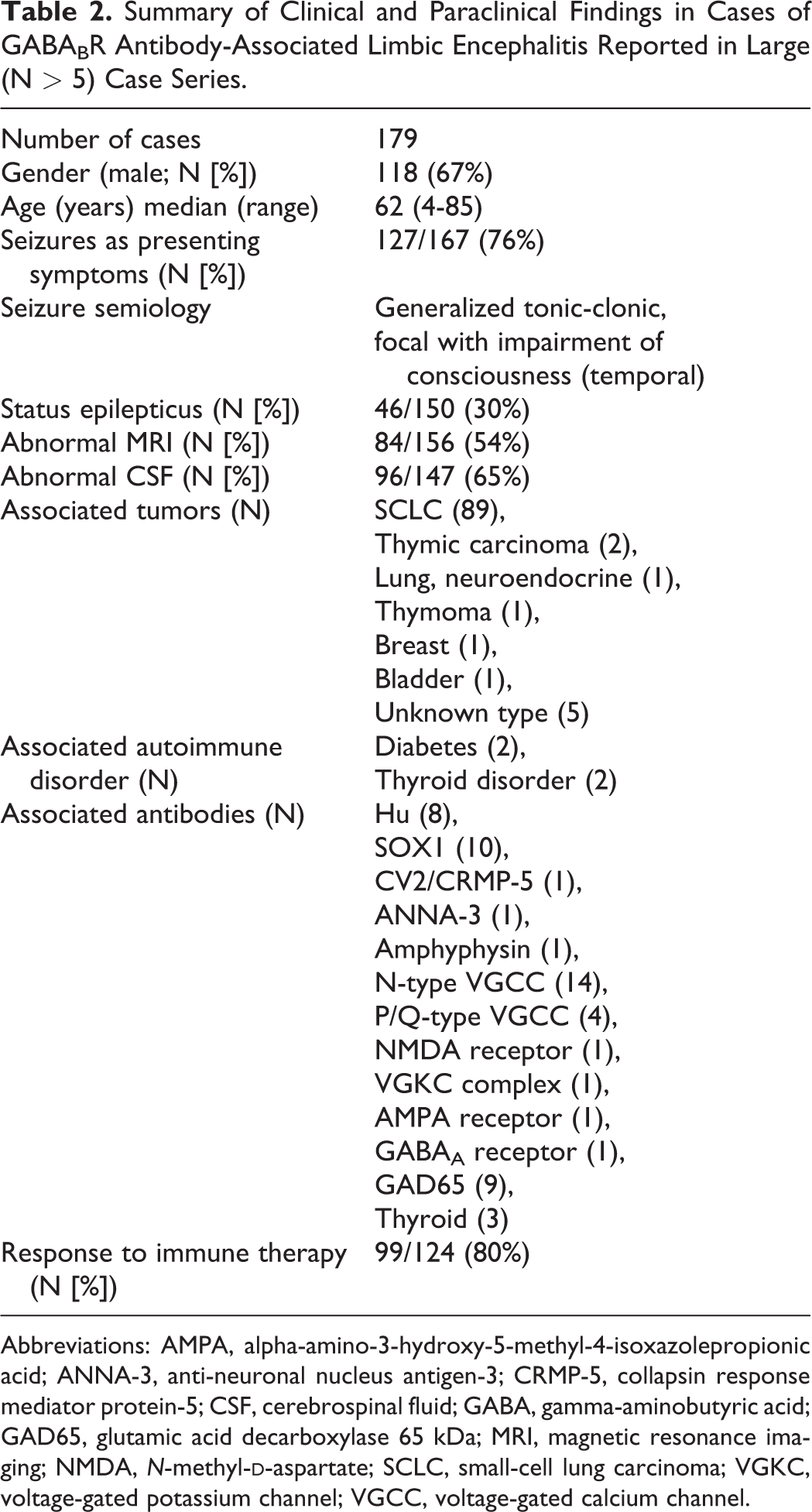
Abbreviations: AMPA, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; ANNA-3, anti-neuronal nucleus antigen-3; CRMP-5, collapsin response mediator protein-5; CSF, cerebrospinal fluid; GABA, gamma-aminobutyric acid; GAD65, glutamic acid decarboxylase 65 kDa; MRI, magnetic resonance imaging; NMDA, N-methyl-
In this study, the authors report the clinical features of a new series of 32 patients diagnosed at a national reference center. They also describe a novel antibody targeted at the potassium channel tetramerization domain-containing protein 16 (KCTD16) in a subgroup of these patients, especially paraneoplastic cases.
Most (27/32) of these new patients with a GABABR antibody presented with LE, and seizures occurred in all. Seizures were the first clinical manifestation in 17 patients and evolved to refractory status epilepticus in 13. The most frequent seizure semiology was generalized or bilateralized tonic–clonic, although some patients also had focal seizures with impairment of consciousness, with brain magnetic resonance imaging and electroencephalography pointing toward unilateral or bilateral mesial temporal lobe foci. Four patients presented with rapidly progressive dementia, which mimicked the clinical and biological presentation of Creutzfeldt-Jakob disease, including the elevation of 14-3-3 and τ protein levels in the cerebrospinal fluid (CSF). Whether or not subclinical seizures might have contributed to the rapid cognitive decline was not systematically investigated. One patient had subacute cerebellar ataxia. This report thus further confirms that LE with prominent ictal manifestations is the most typical clinical presentation of GABABR antibodies. It also underscores that the range of uncommon clinical manifestations associated with the antibody extends beyond LE. In addition to rapidly progressive dementia and subacute cerebellar ataxia, cases of opsoclonus–myoclonus syndrome, progressive encephalopathy with rigidity and myoclonus, and brainstem encephalitis were previously reported. 3 –5 Importantly, the response to immune and oncological therapies was observed in 22 of 26 treated patients, with seizure control being achieved faster than cognitive improvement. Eighteen patients achieved a good outcome with a score ≤2 on the modified Rankin scale (mRS), although no patient became asymptomatic (mRS of 0). This indicates that most patients had residual cognitive dysfunction, at least during the duration of the follow-up period.
Systematic cancer screening with whole-body fluorodeoxyglucose-positron emission tomography (FDG-PET) led to the identification of an underlying cancer in 21 cases, most frequently small-cell lung carcinoma (SCLC), confirming prior reports of a paraneoplastic etiology in 60% of cases (Table 2). This obviously indicates that thorough screening for an occult neoplasm is mandatory these cases.
Current expert guidelines for SCLC screening recommend performing chest computed tomography (CT), followed by FDG-PET if the CT is negative, or integrated FDG-PET/CT every 6 months for 4 years. 12 Although intensive repeated screening is certainly warranted for cases with a high risk of occult neoplasm, such as those with antibodies targeted at intranuclear or cytoplasmic antigens (Hu, Ma2/Ta, etc), it might not be cost-effective in patients with a lower risk, such as most of those with neuronal surface antibodies (LGI1, Caspr2, etc). In fact, inappropriate screening might even become a source of unnecessary exposure to radiation and produce anxiety in these patients. In these cases, additional information that can help assess more accurately the probability of a paraneoplastic etiology and the need for intensive screening would be welcome. And this is where the major novelty of this study lies. The authors identified a new antibody directed at KCTD16. This protein belongs to a family of intracellular proteins that bind to the GABABR and contribute to the downstream inhibitory signaling of the receptor. A KCTD16 antibody was found in 23 of 32 patients with GABABR antibody. Most importantly, its presence was associated with a much higher risk of an underlying neoplasm (17/23 vs 3/9). The authors also identified onconeural antibodies in 2 of the KCTD16-negative paraneoplastic cases (one Hu and one voltage-gated calcium channel [VGCC]) and in 6 of the KCTD16-positive paraneoplastic cases (including Hu, SOX1, Ri, and VGCC). In previous series, other antibodies (CV2/CRMP-5, amphyphysin) had been shown to co-occur in a few patients with GABABR antibodies. 2 –6 Thus, the presence or absence of additional antibodies, such as KCDT16, Hu, SOX1, or VGCC, in addition to GABABR antibody, has important clinical implications, as it does modify the likelihood of an underlying cancer and might help guide clinical management. As a side note, the presence of a tumor and of KCTD16 antibody was associated with higher GABABR antibody titers in the CSF and a more severe clinical course. This association between the presence of an underlying tumor, a higher antibody titer and a more severe clinical picture, is reminiscent of the anti-NMDAR syndrome.
The authors also provide important information regarding the sensitivity and specificity of different methods used for antibody detection and identification. Immunostaining of sections of cerebral issue and of live neurons had a sensitivity close to 100% on both CSF and serum. These methods however do not allow the identification of specific antibodies and are used for screening. Specific detection of GABABR antibodies using both commercially available and in house cell-based assays showed a similarly suboptimal (84%-97%) sensitivity. For the practicing clinician, the key point to remember is that commercially available methods lack sensitivity for the detection of known antibodies, including GABABR, and are unable to identify antibodies that are yet to be discovered. A negative result does not exclude the diagnosis of autoimmune encephalitis and should prompt further investigations, with the help of a research lab, if possible. Perfect sensitivity was indeed achieved using an in-house tailored cell-based assay combining multiple antigens (GABABR and KCTD16).
Altogether, this study further underscores the clinical and immunological complexity of LE. It also provides exciting new leads on how to better tease out idiopathic and paraneoplastic cases, and ultimately improve patient care. Hopefully, this observation will be replicated in larger studies and similar findings will emerge in cases of LE associated with other antibodies that portend a comparable or even lower overall risk of paraneoplastic etiology, such as Caspr2 or LGI1.