
Abstract
Trial registration: ClinicalTrials.gov NCT03385577
Keywords
Introduction
The American Cancer Society (ACS) estimates that in 2024 approximately 116 930 new individuals will be diagnosed with gynecologic cancer in the United States (US). About 156,430 new cases of gastrointestinal cancers and 118 270 new lung and bronchus cancers are anticipated among US women in the same year. 1 Distress is a prevalent quality of life (QoL) concern in cancer and a salient unmet need among women with gynecologic,2 -4 gastrointestinal,5,6 and thoracic malignancies.7,8 This is particularly true in socially and/or economically marginalized cancer patients who bear a disproportionate burden in QoL and cancer outcomes. Relative to their non-Hispanic White counterparts or patients with greater socioeconomic resources, women of color and/or lower socioeconomic status (SES) with gynecologic malignancies experience more aggressive disease, higher comorbidity burden, poorer access and provider adherence to comprehensive treatment, and poorer prognosis and survival.9,10 Similar patterns are observed in women with gastrointestinal 5 and thoracic cancers. 11
Psychologically oriented yoga interventions—that is, interventions predicated on the philosophical, practical intersections among psychotherapeutic skill modalities and the practice of yoga—are safe 12 and effective in reducing depression, anxiety, and overall distress among women with cancer.12 -14 Mind-body interventions also reduce fear of cancer recurrence (FCR).15,16 FCR is an anticipatory distress regarding possible cancer return/progression and is a common unmet QoL need in cancer. 17 The extant literature characterizes FCR as independent of prognosis and estimated survival and prevalent across time throughout remission, with detrimental impacts on physical, mental, and social health-related QoL in many cancers. 18 Recent findings demonstrate particularly prevalent FCR among patients with gynecologic,19,20 as well as gastrointestinal and thoracic, 21 cancers. While manifest in heterogeneous clinical presentations, emerging evidence accentuates the potential role of psychoeducational, cognitive-behavioral, mindfulness-based, and general supportive care interventions in mitigating distress and impairment related to FCR. 18 Thus, there is growing evidence that psychological yoga interventions may reduce distress in women with cancer.
Distress-reduction intervention research has primarily focused on breast cancer and early stage disease.12,14,22 However, psychological distress is a critical need in gynecologic, gastrointestinal, and thoracic cancers, in which cancer QoL remains understudied,2,5,7,23 -25 especially among such patients with advanced stage disease and significant distress related to FCR.19,20,26,27 While several studies have investigated yoga to reduce distress among women with gynecologic28,29 and other non-breast cancers 30 this literature remains limited even though such interventions may have high potential to improve distress. Published studies lack participant diversity and have not investigated inequities in intervention efficacy.12,22 This is notable, given racial, ethnic, and socioeconomic disparities in incidence, exposure to risk factors, medical and psychological comorbidity burden, access and provider adherence to optimal treatment guidelines, prognosis, and survival outcomes in gynecologic cancers.9,10 Similar disparities are observed among women with gastrointestinal 5 and thoracic cancers, 11 who represent additional understudied populations with unmet quality of life needs. 31
The primary aim of the present Phase IIa proof-of-concept study 32 was to evaluate the plausibility of an integrated group yoga and psychotherapy intervention in mitigating distress in gynecologic cancers, 33 with expansion to women with gastrointestinal and thoracic cancers. The intervention was designed to integrate 1000-year-old Eastern yogic philosophies 34 with psychotherapeutic skills as a distress management intervention for women with common non-breast cancers. Psychotherapeutic skills were drawn from core elements of Cognitive Behavioral Therapy (CBT), 35 Acceptance and Commitment Therapy (ACT), 36 and Dialectical Behavior Therapy (DBT) 37 as applied to cancer distress. Demographics and cancer site were examined as predictors of distress and distress change.
Methods
Participants
Participants were women with newly diagnosed gynecologic, gastrointestinal, or thoracic cancers enrolled from a large, academic health science center in the Southeast United States into a single-arm Phase IIa clinical trial 33 (ClinicalTrials.gov NCT03385577). Inclusion criteria were (a) new or recurrent gynecologic, gastrointestinal, or thoracic cancer within the past year; (b) 18-90 years of age; and (c) English fluency. Exclusion criteria included: (a) current, severe, and uncontrolled psychopathology (eg, bipolar disorders, psychotic disorders) or (b) neurocognitive disorder that could impair safe participation; (c) Karnofksy score less than 60, indicating performance status requiring considerable assistance from others and medical attention 38 ; (d) pregnancy or attempting to become pregnant; and (e) participation in at least once weekly yoga classes for at least 6 months within the past 5 years. All study procedures were approved by the University of Florida Institutional Review Board-01 (UF IRB-01; IRB201700079, 12/21/2017).
Procedures
Recruitment
Active recruitment to the study occurred from February 2018 to May 2021. Potentially eligible women were approached following their oncology visit. Fully eligible women were enrolled and added to a group intervention waitlist for their cancer diagnosis following completion of written informed consent procedures. Rolling cohorts of 2 to 6 women were then formed for group participation. Details regarding patient-centered, culturally sensitive recruitment procedures to promote sample diversity, equity, and inclusion are provided in Hanvey et al. 39
Measures
Participants completed a psychosocial assessment immediately prior to the first session and repeated the assessment immediately after the final session, with virtual participants completing their respective assessments sent via mail as closely as possible to their first and final sessions, respectively. Demographics were assessed with the MacArthur Sociodemographic Questionnaire, a 16-item measure examining race, ethnicity, and socioeconomic status (SES) indicators, including education, income, employment, insurance status, household structure, and perceived SES. 40 FCR was measured with the Fear of Cancer Recurrence Inventory (FCRI), which is a 42-item measure assessing FCR among individuals with cancer, with seven main subscales: Triggers, Severity, Psychological Distress, Coping, Functioning, Insight, and Reassurance. 41 The National Comprehensive Cancer Network (NCCN) Distress Thermometer (DT) was used to assess cancer-related distress. 42 The Beck et al Depression Inventory-Second Edition (BDI-II), a 21-item measure, was used to assess depressive symptomatology. The first 10 items assess affective symptoms of depression, and its final 11 items evaluate somatic symptoms of depression. 43 The State-Trait Anxiety Inventory (STAI), a 40-item measure, evaluated state (in the moment) anxiety and trait (general) anxiety.
Intervention
The intervention was a 10-week, in-person, manualized, group program entitled, Stilling the Waters of Uncertainty: A Yoga Program for Women with Cancer, divided into 5 modules: (1) Getting Started, (2) Cultivating a Mindful Attitude, (3) Self-Care and Compassion, (4) Finding Peace and Acceptance, and (5) the Power of the Present Moment. 33 Each session employed a combination of breathing and relaxation techniques, mindfulness meditation, psychotherapy skills, and gentle yoga, with the collective aim of optimizing physical and mental quality of life among participants. Yoga postures (referred to as asana in Sanskrit) and breathing exercises (referred to as pranayama) were selected for simplicity, safety, and relevance to the medical needs of the participants. The intervention author was a doctoral candidate in clinical health psychology at the time of intervention development with extensive experience working with cancer patients. She also previously completed a 200-hour general yoga teacher certification through a Yoga Alliance Registered Yoga School in 2011 as well as the Yoga for Cancer (“y4c”) teacher training program focused on yoga instruction in oncology settings. She was trained in a primarily vinyasa yoga tradition and the manualized program thus heavily emphasizes linking of movement and breath to improve stress management and health-related quality of life through the mind-body connection. Psychotherapy skills integrated into the curriculum included relevant psychoeducation, progressive muscle relaxation, cognitive restructuring, nonjudgmental awareness, acceptance, present moment contact, loving-kindness, values identification, and wise mind. Specific components of the integrated curriculum are detailed in Table 1.
Integrated Psychological Yoga Intervention Curriculum.*

“✔” indicates key source from which conceptual or practical material was derived, with recognition of significant intersection between psychotherapeutic and yogic philosophies presented in contemporary times via different language and frameworks.
Sessions were conducted once per week, for 60 to 90 minutes each session. Practice between sessions was monitored via verbal report during group sharing at the start of each session. Each session was conducted by 1 of 4 certified yoga instructors—one of whom was a Multiple Principal Investigator and intervention developer of the present study. Furthermore, this MPI contributed to the selection process of the additional yoga instructors to ensure basic training requirements and clinical appropriateness for working with cancer patients in a clinical setting. The other 3 instructors were certified by a 1000-hour Yoga Alliance Program (E-RYT) with Level 2 Zen certification, a 500-hour Jivamukti Yoga program in 2005 (E-RYT), and a 200-hour program in 2017 (RYT), respectively. All postures were considered minimal risk, with most poses completed from a seated, lying down, or basic standing position with no advanced movement. Participants were heavily encouraged and shown how to modify, prop, or support all yoga postures as needed for safety and comfort. No advanced balance or inversion poses were included. Uniformity of intervention was supervised across live and virtual modalities by staff designated to monitor quality assurance with the manualized protocol as foundation to affirm instructor and participant adherence. Participants received a program manual and instructors received manualized instructions to ensure flexible but consistent yoga instruction across teachers and cohorts. Due to COVID-19 prohibitions against in-person research, sessions were moved from in-person to a virtual format (n = 25) beginning in approximately March of 2020. For virtual participants, the physical address of their location, phone number, and an emergency contact number were collected to ensure safety support during potential adverse events. Virtual participants completed intervention exercises with audiovisual functions activated, so that their participation could be closely monitored and verbally modified as needed by the certified instructor. Participants were compensated $10 for each completed session.
Statistical Analysis
Mixed linear models (MLM) using maximum likelihood estimation were conducted with IBM Statistical Package for the Social Sciences (SPSS) Version 25.0 to evaluate the degree to which (1) distress indicator scores changed from pre- to post-intervention and (unconditional growth model [UGM]) (2) mean distress indicator scores and changes in distress indicator scores were predicted by the fixed effects of age, minority status, SES, and cancer site (conditional growth models). Random effects of linear time were tested, but ultimately eliminated, from the UGMs due to Hessian errors.
BDI-II depression scores were deconstructed into 3 outcome variables: total, affective, and somatic score. Age-adjusted standardized scores for state and trait anxiety were derived from the STAI. NCCN DT scores were deconstructed into 2 outcomes, one in continuous raw form and the other dichotomized by clinical relevance (≥4 = clinically relevant distress). 42 FCR was deconstructed into 8 continuous outcome variables (total score plus seven component scales). Age was dichotomized at 60 years old. Minority status was dichotomized between non-Hispanic White women and women of color (eg, Black/African American, Hispanic/Latina). SES was measured as a continuous composite variable comprised of education, employment, and income. 44 Cancer site/diagnosis was dichotomized into gynecologic cancer (“1”) or thoracic or gastrointestinal cancer (“0”). To aid in visual interpretation of potential interactions, SES was trichotomized by standard deviation relative to the mean.
Model building began with the unconditional means model (UMM) followed by the UGM. Significant UGMs were followed by conditional growth modeling (CGMs), which evaluated interactions between the fixed effect of occasion and minority status, SES, age, and diagnosis. Model fit was evaluated using the negative 2 Log Likelihood statistic (−2LL) and associated chi-square analyses to assess the presence of significant improvement.
Results
Participant Characteristics
Of the 125 participants who were enrolled, 50.4% (n = 63) were younger than 60 years old (M = 58.55, SD = 10.81). Approximately 26% (n = 32) were women of color, including 17 Black women (13.6%), 10 Hispanic/Latina White women (8%), 2 Asian American/Pacific Islander women (1.6%), 2 American Indian/Alaska Native women (1.6%), and 1 Hispanic/Latina woman of unknown race (0.08%). The remaining 74.4% were characterized as non-Hispanic White. Most participants were diagnosed with gynecologic cancers (n = 87, 69.6%); 16.0% (n = 20) were diagnosed with thoracic cancers and 14.4% with gastrointestinal cancers (n = 18). No significant differences were observed between participants enrolled during live intervention administration and their virtual intervention counterparts across dichotomized race (P = .571), ethnicity (P = .241), minority status (P = .838), or age (P = .858). The mean composite SES score was 3.98 (SD = 1.53, n = 46). Table 2 presents demographic characteristics of the enrolled sample.
Sample Demographic, Socioeconomic, and Diagnostic Characteristics.

Abbreviations: M, mean; SD, standard deviation; SES, socioeconomic status.
Fifty-one participants were included in analysis, with 71 participants lost to follow-up, withdrawn, or deceased between enrollment and provision of baseline. Of these participants, 23.5% were women of color (n = 12). Three additional participants who started the intervention did not provide baseline or follow-up assessment data and thus were excluded from analysis. These details are summarized in the study CONSORT Diagram (Figure 1). Table 3 presents the mean distress measure scores from pre- to post-intervention. No adverse events deemed serious, unanticipated, and related to study procedures were documented throughout study participation. Three minor adverse events that could not be definitively rendered unrelated to study procedures were documented; however, these events were deemed non-serious and expected (ie, mild dizziness, muscle soreness). Live participant adherence to intervention was visually monitored by the certified yoga instructor and at least 1 supervising staff member to ensure both (1) instructor adherence to the manualized curriculum and (2) participant adherence to instructor prompts.

CONSORT diagram.
Distress Measure Scores from Pre- to Post-Intervention (N = 41 Unless Otherwise Noted).

N = 40.
Proof-of-Concept: Change in Distress Across Intervention
Fear of cancer recurrence
Total Fcr
The UGM for total FCR score revealed no significant change across the sample from pre- to post-intervention (P = .424), with minimal improvement in model fit when incorporating occasion into the unconditional means model (χ2 = 0.649, P = .420). Thus, no conditional models examining demographic, socioeconomic, or diagnostic effects on change in symptoms over time were pursued for total FCR score.
FCR subscales
The UGM for the FCR Psychological Distress subscale revealed a trend towards average decline across the sample from pre- to post-intervention (b = −1.05, P = .073), with a trend towards model fit improvement when adding occasion to the UMM (χ2 = 3.295, P = .069) (Table 4, Model 2). CGMs evaluating main effects of minority status (Table 4, Model 3a), age (Table 4, Model 3c), and diagnostic group (Table 4, Model 3d) and their respective interactions with occasion revealed no significant demographic or socioeconomic differences in overall FCR Psychological Distress or change across the intervention. However, a CGM evaluating the main effect of SES and its interaction with occasion revealed that higher SES participants experienced significantly greater decline in FCR Psychological Distress relative to their lower SES counterparts (b = −0.744, P = .050) (Table 4, Model 3c). These effects were strengthened controlling for the effects of diagnostic group (b = −0.813, P = .034), with this final model demonstrating significant improvement relative to the UGM (χ2 = 67.893, P < .001; Table 4, Model 4; Figure 2).
Summary of Models for Psychological Distress Subscale related to FCR.

Abbreviations: MS, racial and/or ethnic minority status; SES, socioeconomic status; Dx, diagnosis; LT, linear time (occasion); AIC, Akaike information criterion; BIC, Bayesian information criterion; eta-squared, r-squared, additional variance explained relative to prior model in sequence; Model 1, UMM; Model 2, UGM; Model 3, CGM with demographic or socioeconomic predictor, demographic or socioeconomic predictor × occasion; Model 4, CGM with demographic or socioeconomic predictor, Dx, demographic or socioeconomic predictor × occasion.
Random effects of occasion not evaluated due to presence of only 2 occasions and associated Hessian error.
CGMs incorporating fixed effects of racial and/or ethnic minority status and its interaction with LT.
CGMs incorporating fixed effects of SES and its interaction with LT.
CGMs incorporating fixed effects of age and its interaction with LT.
CGMs incorporating fixed effects of Dx and its interaction with LT.
P ≤ .01. **P ≤ .05. *P ≤ .10.

Interaction between occasion and SES in predicting psychological distress related to FCR.
UGMs for the remainder of FCR subscales, including Triggers, Severity, Coping, Functioning, Insight, and Reassurance, revealed no significant change in FCR symptoms across the sample from pre- to post-intervention (ps > 0.050), with no significant model improvement observed incorporating occasion into any of their respective models (ps > 0.050). Thus, no conditional models examining demographic, socioeconomic, or diagnostic effects on change in symptoms over time were pursued for any other FCR subscales.
Cancer-related distress
The UGM for cancer-related distress score revealed no significant change across the sample from pre- to post-intervention (P = .380), with minimal improvement in model fit when incorporating occasion into the UMM (χ2 = 0.783, P = .376). Thus, no conditional models examining demographic, socioeconomic, or diagnostic effects on change in cancer-related distress from pre- to post-intervention were pursued (not shown).
Depressive symptoms
Total depressive symptoms
A significant average decrease of 2.1 units was observed in total depressive symptoms from pre- to post-intervention (b = −2.06, P = .012), with significant model improvement incorporating occasion into the UMM (χ2 = 6.318, P = .012) (Total Depressive Symptoms, Table 5, Model 2). A CGM evaluating the interaction between occasion and SES revealed an association between higher SES and greater reductions in depressive symptoms across the intervention when controlling for diagnostic group (b = −1.06, P = .049), with significant model improvement observed relative to the UGM for total depressive symptoms (χ2 = 66.332, P < .001) (Total Depressive Symptoms, Table 5, Model 4; Figure 3).
Summary of Models for Depressive Symptoms.

Abbreviations: Exp., Exploratory; MS, racial and/or ethnic minority status; SES, socioeconomic status; Dx, diagnosis; LT, linear time (occasion); AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; eta-squared, r-squared, additional variance explained relative to prior model in sequence.
Model 1 = UMM; Model 2 = UGM; Model 3 = CGM with Demographic or Socioeconomic Predictor, Demographic or Socioeconomic Predictor*Occasion; Model 4 = CGM with Demographic or Socioeconomic Predictor, Dx, Demographic or Socioeconomic Predictor*Occasion; Model 5 = CGM with 3-way interaction between MS, SES, and LT.
CGMs incorporating fixed effects of racial and/or ethnic minority status and its interaction with LT.
CGMs incorporating fixed effects of SES and its interaction with LT.
CGMs incorporating fixed effects of age and its interaction with LT.
CGMs incorporating fixed effects of Dx and its interaction with LT.
P < .01. **P < .05. *P < .10.
Random effects of occasion not evaluated due to presence of only two occasions and associated Hessian error.

Interaction between occasion and SES in predicting total depressive symptoms.
CGMs independently evaluating interactions between occasion and demographic characteristics revealed no significant differences in total depressive symptom change over time by age (Total Depressive Symptoms, Table 5, Model 3c) or by minoritized status (Model 3a); ps > 0.050). However, the CGM incorporating age revealed a trend such that individuals 60 years of age and older had lower average total depressive symptoms than their younger counterparts (b = −4.56, P = .057) (Total Depressive Symptoms, Table 5, Model 3c).
Affective depressive symptoms
The UGM for affective depressive symptoms reflected no significant change across the sample from pre- to post-intervention (P = .528) (Affective Depressive Symptoms, Table 5, Model 2). However, due to the significant decline observed in total depressive symptoms across the sample, a CGM evaluating the interaction between occasion and SES was explored. This model revealed an interaction between occasion and SES, such that higher SES was associated with greater reductions in affective symptoms (b = −0.76, P = .006) (Affective Depressive Symptoms, Table 5, Model 3b, Figure 4). These effects remained when controlling for diagnostic group (b = −0.78, P = .005), with significant model improvement observed relative to the unconditional growth model (χ2 = 58.659, P < .001) (Affective Depressive Symptoms, Table 3, Model 4).

Interaction between occasion and SES in predicting affective depressive symptoms.
Somatic depressive symptoms
A significant average decrease of 1.8 units was observed in somatic depressive symptoms across the sample from pre- to post-intervention (b = −1.79, P = .002), with significant model improvement observed relative to the UMM (χ2 = 9.769, P = .002) (Somatic Depressive Symptoms, Table 5, Model 2). A CGM evaluating the interaction between occasion and minority status revealed significant moderation of this occasion effect, such that women of color experienced greater reductions in somatic depressive symptoms than their non-Hispanic White counterparts (b = −2.71, P = .031), approaching significant model improvement relative to the UGM (χ2 = 4.858, P = .088) (Somatic Depressive Symptoms, Table 5, Model 3a). This interaction was strengthened when controlling for diagnostic group (Figure 5), revealing another significant interaction between minority status and diagnostic group. While non-Hispanic White women and women of color exhibited similar somatic depressive symptoms among patients with gynecologic cancers, women of color with gastrointestinal or thoracic cancers demonstrated higher somatic symptoms than their non-Hispanic White counterparts (b = 9.00, P = .017) (Somatic Depression Symptoms, Table 5, Model 4). In the CGM incorporating both interactions, significant improvement in model fit relative to the UGM was observed (χ2 = 10.634, P = .031).
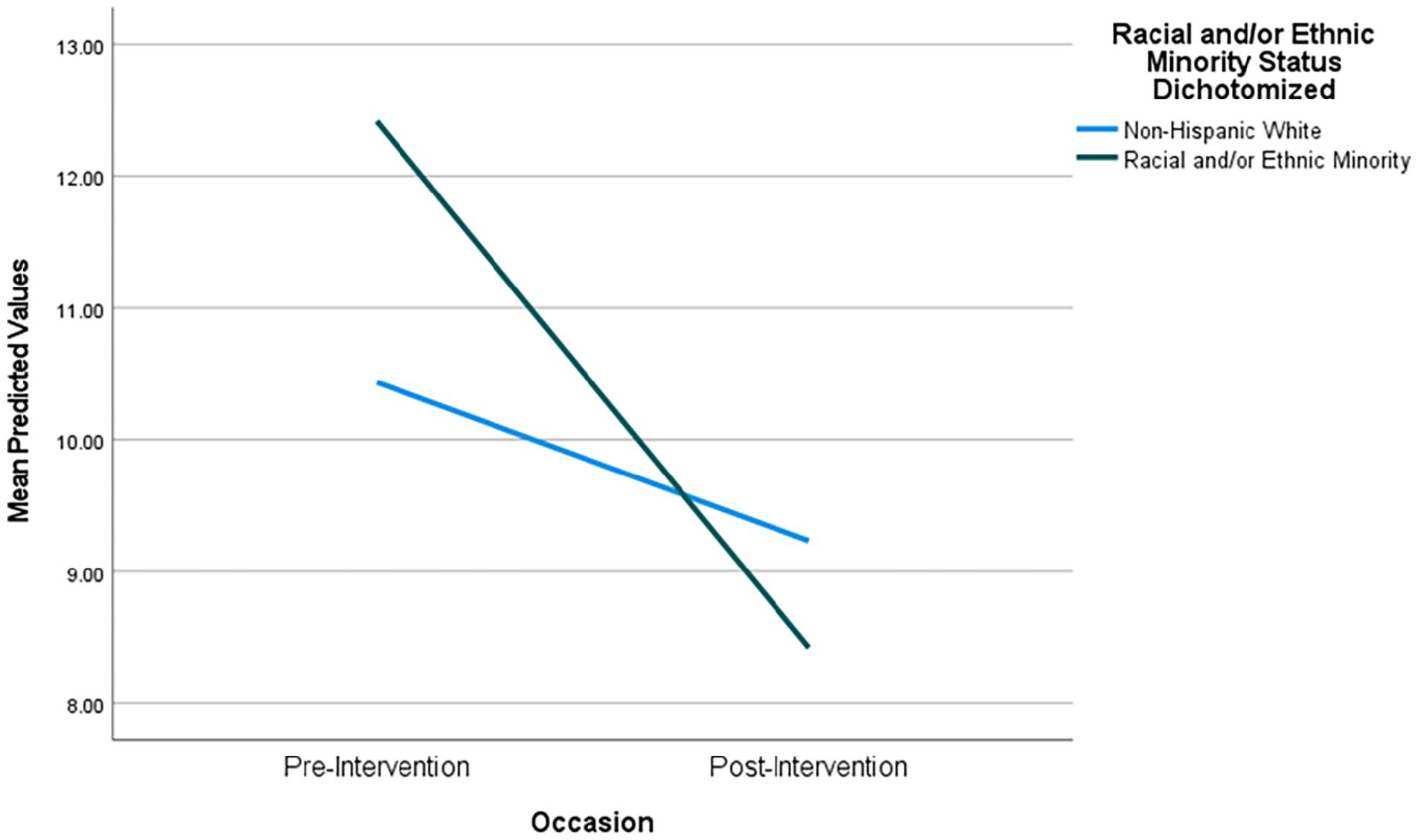
Interaction between occasion and minority status in predicting somatic depressive symptoms.
No significant interaction was observed in the CGM evaluating potential moderating SES effects on occasion in predicting change in somatic depressive symptoms from pre- to post-intervention (P = .483) (Somatic Depressive Symptoms, Table 5, Model 3b). However, this model exhibited significant model improvement relative to the UGM (χ2 = 10.694 P = .030). Due to this improvement and significant moderation by minority status, an integrative CGM was developed assessing the tri-faceted interaction between occasion, minority status, and SES in predicting somatic depressive symptoms. The integrated model rendered this interaction significant (b = 1.73, P = .026) and demonstrated significant improvement in model fit relative to the UGM and the CGM incorporating only minoritized status and its interaction with occasion (χ2 = 8.301, P = .040) (Somatic Depressive Symptoms, Table 5, Model 4). Among women of color, lower SES women experienced greater declines in somatic depressive symptoms compared to their higher SES counterparts, while minimal decline was observed among non-Hispanic White women of any SES group. Further, the greatest decline in somatic symptoms was observed among women of color of the lowest SES group (Figure 6).

Tri-faceted Interaction among occasion, minority status, and SES in predicting somatic depressive symptoms.
Anxiety
State anxiety
A significant average decrease of 6.21 units was observed in standardized state anxiety across the sample from pre- to post-intervention (State Anxiety, Table 6, Model 2). CGMs evaluating potential moderating effects of minority status (State Anxiety, Table 6, Model 3a), age (P = .797) (State Anxiety, Table 6, Model 3b), and diagnosis (State Anxiety, Table 6, Model 3c) on occasion revealed no significant differences in state anxiety change across these characteristics (ps > 0.050). While significant model improvement relative to the UGM was observed when incorporating SES and its interaction with occasion (χ2 = 76.991, P < .001), this was likely attributable to a trend toward higher SES women exhibiting lower overall state anxiety (b = −2.00, P = .076) (Table 6, Model 3b, effect for SES), with no significant interaction observed between occasion and SES (P = .266).
Summary of Models for State Anxiety.

Abbreviations: MS, Racial and/or ethnic minority status; SES, socioeconomic status; Dx, diagnosis; LT, linear time (occasion); AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; eta-squared, r-squared, additional variance explained relative to prior model in sequence.
Model 1 = UMM; Model 2 = UGM; Model 3 = CGM with Demographic or Socioeconomic Predictor, Demographic or Socioeconomic Predictor*Occasion.
CGMs incorporating fixed effects of racial and/or ethnic minority status and its interaction with LT.
CGMs incorporating fixed effects of SES and its interaction with LT.
CGMs incorporating fixed effects of age and its interaction with LT.
CGMs incorporating fixed effects of Dx and its interaction with LT.
P
Random effects of occasion not evaluated due to presence of only two occasions and associated Hessian error.
Trait anxiety
The UGM for trait anxiety scores revealed no significant change in trait anxiety from pre- to post-intervention across the sample (P = .669), with no improvement in model fit when incorporating occasion to the unconditional means model (χ2 = 0.185, P = .669). Thus, no CGMs examining demographic, socioeconomic, or diagnostic effects on change in symptoms over time were pursued for trait anxiety.
Discussion
This study demonstrates proof-of-concept 32 that a single-arm, integrated, group yoga and psychological intervention 33 can mitigate certain distress indicators in women with common non-breast cancers, including gynecologic cancers. Specifically, women demonstrated significant average declines in total and somatic depressive symptoms and state anxiety, and trended toward reduction in psychological distress related to FCR from pre- to post-intervention.
These findings are consistent with meta-analyses demonstrating efficacy of yoga in reducing distress in breast cancer.12 -14 The current study contributes to an emergent corpus of literature supporting similar effects among women with gynecologic and other non-breast cancers, specifically in reducing depression and state anxiety.28 -30 It is among the first to examine how a combined psychological and yoga intervention may impact various distress indicators with an explicit focus on gynecologic cancers, while expanding proof-of-concept to other cancer populations whose potential benefit from such interventions has been minimally studied. Further, these results uniquely decompose intervention impact on specific components of depression and anxiety among women with these malignancies, suggesting differences in intervention efficacy in reducing different aspects of these distress indicators. This study also is among the first to examine how an integrated psychological and yoga intervention may plausibly reduce distress among women with cancer may differ based on marginalizing indicators, such as minority status or SES.
These results revealed that demographic and socioeconomic factors moderated changes in distress across the intervention, which persisted controlling for cancer site. Higher SES participants demonstrated greater reductions in psychological distress related to FCR and total and affective depressive symptoms. However, women of color, who are underserved in cancer care,45,46 exhibited greater reductions in somatic depressive symptoms. These 2 results provide limited evidence that while participants without socioeconomic marginalization might benefit more from the intervention in reducing cognitive-emotional aspects of distress, participants originating from racially or ethnically minoritized backgrounds may experience greater improvements in somatic distress symptoms. However, these conclusions are qualified by the exploratory, tri-faceted moderation analyses of this study. Specifically, these results revealed largest benefit in reducing somatic symptoms among lower SES women of color, that is, women at the intersection of racial and/or ethnic minority status and socioeconomic marginalization. Such findings may be consistent with growing evidence indicating more somatic presentations of depressive symptoms among women of color and/or low SES relative to their non-Hispanic White or higher SES counterparts. 47 While linguistic and acculturative effects were unassessed in the present study, especially with the exclusion of monolingual, Spanish-speaking women, these improvements in psychological outcomes may be even further strengthened among women of color who are less acculturated to dominant ideologies, and thus outcomes, regarding mental health in the United States, as is partially consistent with mixed evidence addressing the Hispanic and immigrant health paradox.48,49 Given that yoga aims to improve health outcomes via mind-body integration, it may be uniquely effective in addressing differences in depressive symptom presentation among socially and/or economically disadvantaged participants that may be overlooked in other mental health interventions. 50 Overall, these findings support the complexity inherent to the impact of racial, ethnic, and/or socioeconomic marginalization on proof-of-concept of this type of intervention in mitigating distress outcomes among women with gynecologic, gastrointestinal, and thoracic cancers.
Despite demonstrating proof-of-concept that (1) an integrated yoga and psychological intervention may be effective in reducing depression, anxiety, and distress related to FCR and (2) social and economic factors may moderate these effects, the intervention did not significantly impact other critical distress outcomes. Significant reductions in overall FCR and sub-components were not observed, contrasting with other studies supporting significant impact of mind-body interventions on FCR. However, these prior studies have been predominantly among individuals with breast cancer.15,16 These results suggest that psychological yoga interventions may benefit from unique tailoring to address elevated recurrence and associated realistic fears among women with gynecologic, 20 gastrointestinal, 51 and thoracic cancers, 52 to enact more clinically significant impact on FCR. Similarly, this study did not support proof-of-concept for yoga in reducing cancer-related distress, about which minimal prior investigation has been conducted. While recent literature suggests that the NCCN DT may be limited in applicability in detecting distress among women with gynecologic and other understudied cancer types, 53 further investigation may be necessary to better target cancer-related distress specific to women with these malignancies in yoga intervention development.
Limitations
These proof-of-concept results are qualified by several limitations. Examining demographic and socioeconomic moderators of pre- to post-intervention changes in distress indicators was an exploratory aim to better address health disparities. Thus, the parent study did not enroll a sample size adequately powered and oversampled with individuals experiencing social or economic marginalization, such as women of color, older adults, and lower SES women, for this aim. Nevertheless, more than 25% of the sample were women of color, and further, Hispanic women approached for participation were more likely to enroll than their non-Hispanic White counterparts. 39 While this reflects potential progress in subverting underrepresentation in cancer clinical trials among women of color, still greater representation of such women is critical for examining proof-of-concept of the intervention with ecological validity that generalizes to the lived experiences of diverse female cancer patients. This is vital given the disproportionately high cancer burden women of color and of lower SES bear, including in gynecologic, gastrointestinal, and thoracic cancers.9,11,31 Still further, given the exclusion of non-English speaking women, these findings are limited in their ecological validity accounting for the potential impacts of linguistic and acculturative factors on cancer clinical trial participation and resulting benefits.54 -56
Likewise, there was modest diversity related to age and socioeconomic indicators of marginalization. The present sample was predominantly younger than 60 years of age and, on average, exhibited middle SES, thus reducing generalizability of the study to older, lower SES, who endure poorer cancer outcomes and remain underrepresented in clinical trials. 46 As such, to better investigate moderating effects of sociodemographic indicators on intervention outcomes with strong validity, it is critical to achieve higher representation of women impacted by low SES and older age. Furthermore, 56.8% the enrolled sample was lost to follow-up, withdrawn, or deceased before the initiation of study procedures, potentially further compromising the generalizability of its findings. Predictors of study attrition and their implications for trial representativeness are further explored by Hanvey et al, though these findings are limited to participants enrolled prior to the COVID-19 pandemic, and thus, virtual intervention administration. 39
Clinical Implications and Future Directions
These results are clinically informative in that they support plausibility that an integrated yoga and psychological intervention for women with gynecologic and other common non-breast cancers can mitigate certain distress outcomes, with some evidence of differential impacts among marginalized women. Prominent models for behavioral treatment development 32 indicate establishing feasibility as an important next step of the preliminary testing phase. Results from this aim are forthcoming and will be used to optimize study design and methodology for a Phase IIc efficacy trial. This is vital, given increasing evidence of the deleterious impacts of distress on cancer-related quality of life, treatment, and survival. 57 While prior research has indicated similar efficacy of yoga interventions in samples of individuals with breast cancer,12 -14 the present study is among the first to extend these findings to women with common, understudied, non-breast malignancies, namely gynecologic, gastrointestinal, and thoracic cancers.
These findings suggest that certain marginalizing indicators moderate intervention effects in reducing distress by eliciting greater or weaker improvements among women of color and lower SES women, depending upon the dimension of distress. Changes in distress may be contingent upon the type of symptoms upon which the intervention primarily acts among diverse samples. This was evidenced by results indicating greatest improvements in somatic depressive symptoms among lower SES women of color and larger reductions in affective, cognitive symptoms of distress among their higher SES counterparts. These findings indicate that socially and/or economically marginalized populations may especially benefit from mind-body interventions for distress, such as the one developed for this study, due to unique responsivity to intervention components that address somatic symptoms. Further, this suggests that integrated psychological yoga interventions for women with cancer should be developed and implemented from an emic, rather than etic, perspective, to account for the diverse needs of this population by centering cultural sensitivity and thus promoting equitable intervention outcomes across social, economic, linguistic, and acculturative factors. 58
After establishing preliminary efficacy, this research should move into a Phase III efficacy trial using a randomized controlled trial design, across a larger sample exhibiting greater diversity social, economic, and cancer diversity. Such studies will be essential to identify more closely (1) causal impacts of the yoga intervention on multiple indicators of distress and (2) differences in impacts that may occur among diverse samples. Additionally, future studies should focus on tailoring interventions to both disease site and relevant marginalizing experiences to maximize efficacy across distress indicators. Should phase III efficacy trials corroborate results of the present study, subsequent investigation could prioritize development of culturally adapted interventions that account for the impacts of marginalization, such as minoritized racial or ethnic identity or lower SES, and evaluate the comparative effectiveness of such tailored interventions.
In conclusion, this study constitutes a preliminary foundation for a Phase III efficacy trial, following establishment of feasibility through Phase IIb pilot research. Specifically, this study supports proof-of-concept for yoga in mitigating certain distress outcomes among diverse women with gynecologic and other understudied cancers, and differences in impact based on demographic and socioeconomic marginalizing indicators. The present study and its proposed future directions can prioritize investigating disparities in efficacy across these indicators and contribute to research that optimizes quality of life and, ultimately, disease outcomes among understudied and underserved cancer populations.
Footnotes
Acknowledgements
We express our gratitude to the clinic directors, medical assistants, nurses, and medical residents/fellows who assisted with achieving our goal of reaching our research population to provide access to this study. We also express our gratitude to Keri Johnson, PhD, and Cayley Balser, Post Graduate Law Fellow, for serving as additional yoga interventionists and providing conceptual contributions to the intervention.
Authors’ Note
Elizabeth L. Kacel is also affiliated to Rush University Medical Center, Chicago, IL, USA.
Author Contributions
GAH outlined aims to address in the present manuscript, developed methodology to evaluate manuscript aims, conducted formal analyses, provided data visualization, and wrote the original draft of the manuscript. EK conceptualized the overarching parent study, designed its integrated intervention under DBP’s supervision, and developed its overarching aims. GAH, EK, KB, AP, and HM contributed to data collection, project administration, and intervention monitoring throughout the parent study. EK, DBP, and SM assisted with intervention development and served as the primary yoga interventionist. ER, MJM, FK, DJ, TG, and DBP provided clinical, research, and/or funding resources to support the project. All authors contributed to editing the manuscript to its finalized form. EK and DBP supervised GAH in developing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author (DBP).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the UF Health Cancer Center, supported in part by state appropriations provided in Fla. Stat. § 381.915 and the National Cancer Institute of the National Institutes of Health under Award Number P30CA247796. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the State of Florida.