
Abstract
Background:
Chemotherapy-induced nausea and vomiting (CINV) is one of the most prevalent and distressing side effects of chemotherapy among patients with cancer worldwide. Despite continuing advances in antiemetic medicines, nausea and vomiting associated with cancer chemotherapy remain a substantial therapeutic concern for many patients. However, P6 and Auricular acupressure (AA) have been recognized as potential therapy for managing chemotherapy-induced nausea and vomiting.
Aim:
This study aimed to evaluate the effectiveness of P6 and Auricular acupressure (AA) in reducing chemotherapy-induced nausea and vomiting among patients with cancer. And to explore a prominent and effective evidence-based protocol for implementing acupressure to treat chemotherapy-induced nausea and vomiting.
Method:
This systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Several databases were used to search for eligible studies using specific keywords. Only systematic reviews and clinical trials on acupressure for managing CINV among adults with cancer were included. This review covered articles published in English from 2015 to 2022.
Results:
A total of 14 published studies were included in this review study; 10 articles were trial studies, and the other 4 were systematic review and meta-analysis studies. The quality of 10 included clinical trials were assessed using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for quantitative studies, the overall result showed that 40% of study rated with moderate quality, no study was rated with low quality, and (60%) studies rated as high-quality study. As well as the quality assessment of all review studies showed that the majority of included systematic reviews and meta-analysis with a low risk of bias and high to moderate power of evidence. In all included studies the acupressure was utilized as a primary complementary intervention for chemotherapy induced nausea and vomiting. The result of this extensive and comprehensive review the P6 and auricular acupressure is an effective complementary therapy in reducing and controlling chemotherapy-induced nausea and vomiting among participants with various types of cancer and receiving various types of chemotherapy.
Conclusion:
The successful and effective application of acupressure in managing CINV for certain types of cancer had been supported in previous literature as a safe, affordable, and non-invasive alternative to pharmaceutical medications. However, standardization guidelines regarding the use of acupressure independently or in combination with other pharmacological therapies to address CINV in various cancers require immediate attention.
Background
Chemotherapy is a widely utilized therapy to control disease symptoms and inhibit cancer progression. Chemotherapy has many side effects that require interventions. 1 According to the American Cancer Society in 2023, 2 chemotherapy-induced side effects include nausea, vomiting, hair loss, and fatigue, which are caused by using chemotherapeutic drugs to treat cancer. In addition, the chemotherapy side effects are often linked with various other complications such as fatigue, muscle strain, anxiety, depression, and metabolic imbalance.3,4. However, chemotherapy-induced nausea and vomiting is one of the most common side effects of chemotherapy among patients with cancer worldwide. 5 Accordingly, 70% to 80% of patients with cancer experience nausea and vomiting within a week of chemotherapy sessions. 1 Chemotherapy-induced nausea and vomiting are frequently strongly correlated with a variety of complications, including fatigue, muscle strain, anxiety, depression, metabolic imbalance, and inadequate caloric and fluid intake. 3
There are different types of chemotherapy-induced nausea and vomiting; the delayed type of nausea and vomiting refers to the condition in which nausea and vomiting are frequently experienced at home from the second to the fifth day after chemotherapy. Acute nausea and vomiting begin between 1 and 2 hours after receiving chemotherapy medications and can last for up to 24 hours after that. 6
Different types of pharmacological approaches are widely used to manage chemotherapy-induced nausea and vomiting include serotonin, neurokinin 1 (NK-1) receptor antagonists, corticosteroids, and metoclopramide.7 -9 However, these medications have serious adverse effects such as extrapyramidal disorders and hypotension.10,11 Therefore, efforts have been directed toward non-pharmacological complementary therapies to treat chemotherapy-induced nausea and vomiting either alone or in combination with pharmacological agents. 9
Complementary and alternative medicine used among patients with cancer has been the subject of research in the past decade. 12 Complementary therapy is a range of alternative healthcare practices used with conventional medicine to promote healing and well-being. 13 Complementary and alternative medicine can include acupuncture, massage, herbal remedies, and meditation. 12
Acupressure is one of the well-studied non-pharmacological treatments for relieving nausea and vomiting. Acupressure is the method of using gentle but firm finger pressure to specific locations on the human body known as acupoints for 5 to 15 minutes. Acupoints are positioned at precise points along imaginary lines called meridians that run throughout the body. Acupressure on the P6 point by using 3 finger breadths underneath the wrist joint of the dominant arm benefited several patients control nausea and vomiting, and the impact prolonged 6 to 8 hours.14,15 Furthermore, acupressure is an effective, non-invasive, and feasible alternative therapy for many symptoms. 16
Specifically, previous studies have shown that P6 (Neiguan) and auricular acupressure can effectively reduce nausea and vomiting among patients with cancer.17 -19 However, previous studies showed that acupressure could cause problems like constipation, diarrhea, abdominal distension, fatigue, and headaches. 19 Whereas Tan et al conducted a study which revealed that auricular acupressure (AA) had mild to moderate side effects. However, an interesting finding emerged from their research, indicating that additional assistance was not required to manage these reported side effects. 5
Study Aims and Objectives
This review aimed to evaluate the effectiveness of acupressure in reducing chemotherapy-induced nausea and vomiting among patients with cancer. Furthermore, the primary objectives of this review were to: (1) Determine whether acupressure as a complementary therapy has a significant effect on reducing and managing nausea and vomiting induced by various types of chemotherapy and to (2) Determine whether the use of acupressure in conjunction with conventional intervention is superior to conventional intervention alone in relieving chemotherapy-induced nausea and vomiting.
The secondary objectives of this review were: (1) To determine the average duration time during each acupressure session and the number of sessions that are significantly effective for nausea and vomiting and (2) To determine the most common use and effective acupoints for acupressure that are effective among patients with cancer who complain of chemotherapy-induced nausea and vomiting.
Method
Protocol and Registration
This systematic review was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) standard. 20 The protocol for this study has been registered in the prospective international register of systematic reviews “PROSPERO,” with the registration number (CRD42023410895), and it is available at: https://www.crd.york.ac.uk/prospero/displayrecord.php?ID=CRD42023410895
Searching Strategies
The search process targeted articles published in peer-reviewed journals relevant to study keywords within the period from 2015 to 2023. The following electronic databases were used: MEDLINE, PubMed, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), EBSCO, SAGE Journals, Google Scholar, and Science-Direct. The PICO framework was used to form clinical queries and facilitate the literature search (Table A1; Appendix A). Relevant keywords were identified through the primary search on various electronic databases. The search included a variety of keywords such as “acupressure,” “acupoint therapy,” “acupoint pressure,” “acupressure for chemotherapy-induced nausea and vomiting,” “Cancer,” and “nausea and vomiting.” In order to enhance the search results, Boolean operators (AND, OR) were utilized both individually and in conjunction with the keywords. Therefore, this allowed for the expansion, combination, or exclusion of certain keywords to refine and filter the search results.
Eligibility
The inclusion criteria for considering relevant articles in this review were: (1) Patients diagnosed with any types of cancer who received chemotherapy, (2) Patients suffering from nausea and/or vomiting after receiving chemotherapy, (3) Patients older than 18 years, (4) Systematic reviews or Clinical trials (Randomized control trials and Quasi-Experimental studies) having acupressure with or without antiemetic medications as the intervention, and (5) Published in English. Studies were excluded if the population of interest was receiving more than 1 complementary therapy or at end-of-life care, or if their nausea and vomiting were not caused by chemotherapy.
Study Selection
In order to identify relevant articles that met the predetermined inclusion criteria, 2 researchers conducted independent screenings of retrieved studies based on their titles and abstracts. However, in cases of disagreement between the 2 researchers, a third researcher was consulted to resolve any differences in opinion. Subsequently, the studies that were deemed relevant and eligible based on this screening process were subjected to a thorough review of their full texts.
Quality Assessment
The quality of clinical trials was evaluated by using the Effective Public Health Practice Project (EPHPP) quality assessment tool. 21 Each study was evaluated in 6 domains (Study bias, study design, control of confounders, blinding, data collection method, and withdrawals and dropouts of participants from the study). Each article’s quality was classified as strong, moderate, or weak based on the scores given to each dimension. The results from each domain were then summed to provide an overall score. The studies were graded as poor quality (2 or more elements were rated as weak), moderate quality (1 element was rated as weak), or high quality (no element was rated as weak). Two researchers independently assessed the quality of all included studies (BA & AY).
The quality of systematic reviews was assessed using the measurement tool to assess systematic reviews (AMSTAR2). 22 The tool has 16 elements that have to be rated as (critically low, low, moderate, or high). The overall confidence rating was derived for each systematic review based on the combination of scores on 7 critical and 9 noncritical items. Therefore, each article could obtain a score between 0 (no criteria) and 16 (all criteria).
Disagreements and questions that emerged throughout the review process were resolved through discussions and agreement between researchers.
Risk of Bias
The risk of bias in the included quantitative studies was evaluated using the Cochrane risk of bias tool/version 2 (ROB 2). 23 Accordingly, each study was evaluated through different domains included in ROB 2, which reflect several aspects of the result of each included clinical trial. These domains include random sequence generation, allocation concealment, and degree of blinding, sample drop, and non-selective reporting. 24 Each domain of ROB 2 is evaluated in relation to the risk of bias found in 1 of the 3 major assessments: Low risk of bias, some concerns of bias, or high risk of bias23,24. Then, the overall risk of bias judgment was evaluated by assessing the different domains of ROB 2 for each study.
Assessment of bias was conducted using the ROBIS tool, which was designed specifically to assess the risk of bias in systematic reviews 25 . Accordingly, the bias assessment tool evaluated each systematic review as a “high,” “low,” or “unclear” risk. The tool was completed in 3 phases: relevancy assessment (optional), identification with the review process, and risk judgment of bias in the review study. The risk of bias assessment includes signaling questions to assist in analyzing specific concerns regarding potential biases. Thus, the evaluations from these signaling questions assist assessors in determining the overall risk of bias.
Study Synthesis
The data synthesis process involved 3 reviewers who carefully analyzed and assessed the collected data. In order to ensure accuracy and reliability, any differences in opinions or interpretations were resolved through mutual agreement among the reviewers. Only data that received unanimous agreement from all 3 reviewers were included in the final analysis. To provide a comprehensive overview of the evidence, a narrative-descriptive synthesis was created, which incorporated a summary table. This table highlighted the key findings from the various studies and also addressed the consistency of these findings across the different research studies.
Result
Study Selection
A total of 407 articles were retrieved from the specified electronic online databases; 204 duplicates were excluded. Subsequently, the researcher carefully evaluated the titles and abstracts of the remaining 203 articles to identify their relevance to the research topic. After this screening process, a final selection of 49 articles was made for full-text examination. Out of these 49 articles, only 14 were deemed suitable for inclusion in our review. The search strategy and selection procedure are depicted in the PRISMA flowchart (Figure 1). 20

PRISMA flow diagram of study selection.
Characteristics of Included Studies
Fourteen articles were included in this review study, all studies published between 2015 and 2022 and written in English. Acupressure was utilized as a complementary intervention for chemotherapy-induced nausea and vomiting among hematologic and oncologic patients in the included publications. In total, 10 out of 14 articles were clinical trial studies, and the other 4 were review studies. About 43% of studies are Chinese (n = 4). Other studies were conducted in India (n = 2, 14.2%), Iran (n = 2, 14.2%), Taiwan (n = 2, 14.2%), Turkey (n = 1, 7.1%), Palestine (n = 1, 7.1%), Korea (n = 1, 7.1%), and the United States (n = 1, 7.1%). A summary of the study’s characteristics is shown in Table A1, which includes the number of sample sizes, study design, country, chemotherapy rating, chemotherapy regimen, acupressure points, treatments, interventions, outcomes, and measurements.
Characteristics of trial studies
In terms of population characteristics, 10 articles included a total of 508 patients; the population sizes of the trials ranged from 20 to 300. Approximately 40% of the population were patients with breast cancer,5,6,26,27 and other diagnoses included myeloblastic leukemia, 28 colorectal cancer 1 , ovarian cancer, 29 head and neck cancer, 30 and lung cancer, 31 with the expectation that one study included a multi-hematologic and oncologic diagnosis. 18
According to study comparisons, 5 of the included studies were randomized clinical trials (RCTs), and the other 5 were quasi-experiments. One of the RCT studies 6 was designed as a crossover study; others were designed as parallel randomized control trials. Whereas 2 articles did not report the chemotherapeutic regimen.1,29 Other chemotherapy regimens were 30% cisplatin; the other 30% used moderate- to high-emetogenic chemotherapeutic agents such as doxorubicin; one study conducted by Augustine and Latha that used a radio-sensitizer therapy. 30 Most of the studies (70%) contained at least 1 cycle of chemotherapy.
In terms of outcome, the outcome assesses the severity, episode, and delayed nausea and vomiting experience among the population with different scales of measurements; almost 70% reported the intensity of nausea as the major outcome.
Characteristics of the included reviews
In this comprehensive review study, the researchers analyzed a total of 4 systematic reviews (SRs) that specifically focused on the use of acupressure as a complementary approach to alleviate the severity or frequency of nausea and vomiting experienced by patients undergoing chemotherapy treatment for hematologic and oncologic conditions. The selected SRs encompassed a diverse range of 68 studies.
The SRs included 31 randomized clinical trials among patients with cancer patients to measure the severity and delayed nausea and vomiting episodes.17,19 While the other SRs included control studies with parallel or crossover designs, 15 studies among patients with breast cancer measured the severity of nausea and vomiting as a main outcome. 9 In addition, the last included meta-analysis involved a thorough examination of 18 studies. These studies were specifically designed to investigate the effectiveness of acupressure in preventing nausea and vomiting caused by chemotherapy; moreover, it is worth noting that the included research studies were conducted among various types of cancer and across different countries. The main characteristics of the included SRs are shown in (Table A1).
Quality of Included Studies
Quality of included clinical trial studies
The quality of 10 included clinical trial studies (50% of studies were a Randomized Control Trials and 50% were a Quasi- Experimental studies) in this review were assessed using the effective public health practice project (EPHPP) quality assessment tool for quantitative studies Table 1. Each study was evaluated in 6 domains including study bias, study design, control of confounders, blinding, data collection method, and withdrawals and dropouts of participants from the study. Based on selection bias domain; all participants in all included studies were agreed to participate in the study prior any intervention and the authors stated that the consents were signed by all participants, furthermore, according to the blinding domain; one randomized controlled trial (10%) followed a double-blind study design. 26 However, the majority of included clinical trials applied partial blinding study designs (90%). Furthermore, the data in all included studies were collected using a tool shown to be reliable and valid, all authors of included studies (100%) reported the number of withdrawals and dropouts’ participants in their study, and the percentage of participants completed the study in all articles were above 80%. Thus, the overall result after both reviewer discussions showed the 40% of the study was rated with moderate quality, no study was rated with low quality, and (60%) studies rated as high-quality studies.
Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies (n = 10).

Total rating score (1 = strong, 2 = moderate, 3 = weak).
Quality of included review studies
The quality of all review studies in this review was assessed using a quality assessment checklist for systematic reviews (AMSTAR 2). According to this review, no systematic review or meta-analysis studies fulfilled all the AMSTAR 2 scale requirements. Indeed, the majority of included systematic reviews showed a low risk of bias and high to moderate power of evidence (Table 2). The score varied from (9) 32 to (13) 19 points, with an average of 11 out of 16 possible total points. Items 1, 2, 3, 6, 7, and 16 were scored as positive for all included reviews. However, all included studies (100%) did not score items 4 and 5. Moreover, items 8, 10, and 13 were scored as positive for 75% of studies; however, items 14 and 15 were not applicable for 50% of systematic reviews 9,32.
Quality Assessment Checklist for Systematic Reviews (AMSTAR 2).

Risk of bias assessment of the included clinical trials
The risk of bias for included trials was evaluated by Cochrane risk of bias tool (ROB). Each domain of ROB2 was evaluated in relation to the risk of bias found to 1 of the 3 major assessments: Low risk of bias, some concerns of bias, or high risk of bias.23,24 Overall risk of bias judgment was evaluated by assessing the different domains of ROB 2 for each study and the decision was made based on those domains’ evaluations of risk of bias. Among the included clinical studies (10 studies), 5 studies were considered to have low risk of bias after assessment with ROB 2. Whereas 3 studies had some concerns of bias, and the remaining 2 studies were considered to have a high risk of bias. Table 3 provides details of each ROB 2 domain evaluation for each included study coupled with overall risk of bias.
Cochrane Risk of Bias Tool for Quantitative Studies (n = 10).
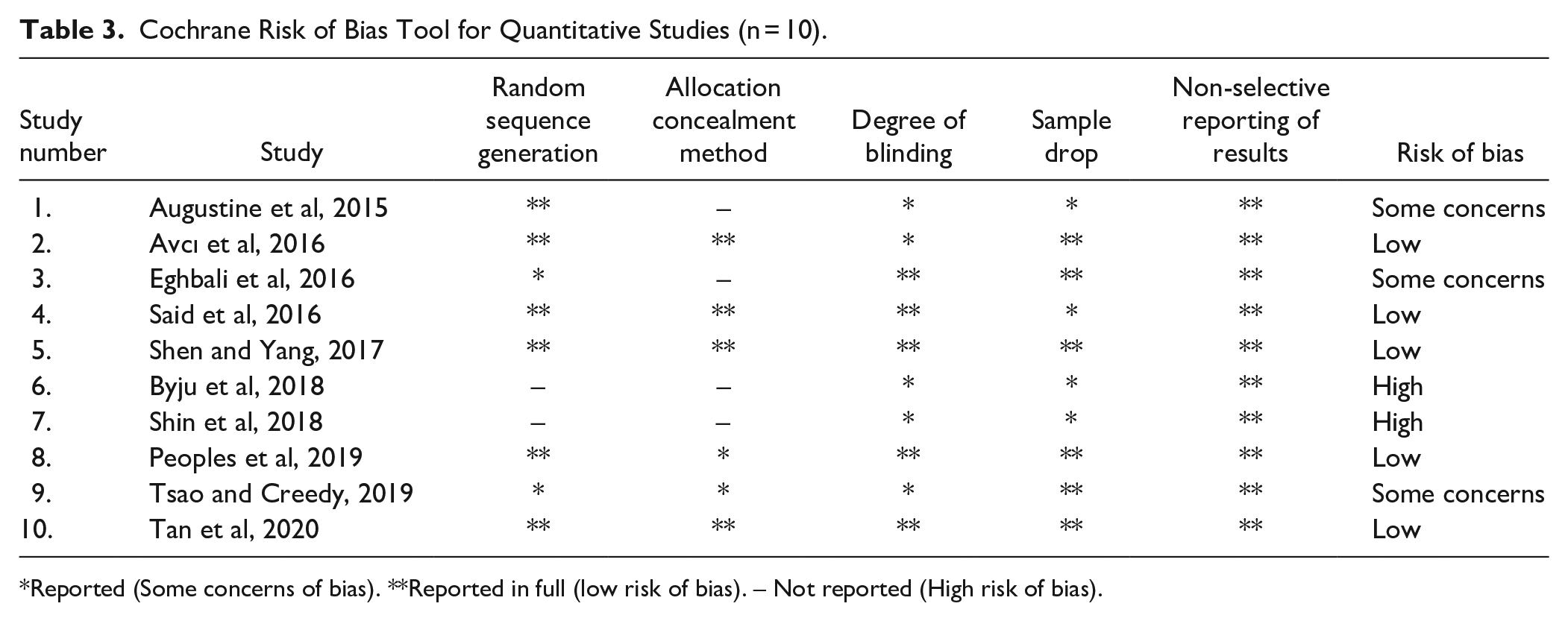
Reported (Some concerns of bias). **Reported in full (low risk of bias). – Not reported (High risk of bias).
Risk bias for systematic review
The evaluation results with the ROBIS tool showed that 2 of the 4 included reviews had a low overall risk of bias. The included SRs presented their research questions in a way compatible with this overview. All studies provided eligibility criteria details, while 1 of 4 studies had clearly defined PICO components. The domains that most frequently presented risk of bias were those related to eligibility criteria and the identification and selection of studies. None of the reviews reported the registration of a previous protocol, and all studies presented restrictions on including studies based on the language without justification. Only one study presented restrictions based on data, one included grey literature, and all the studies reported using at least 2 reviewers throughout the review process. However, one of the included reviews did not report. Three reports used some tools to analyze the quality of the included primary studies or their risk of bias. The risk of bias of the included SRs that evaluated by the ROBIS tool is shown in Figure 2 and Table 4.
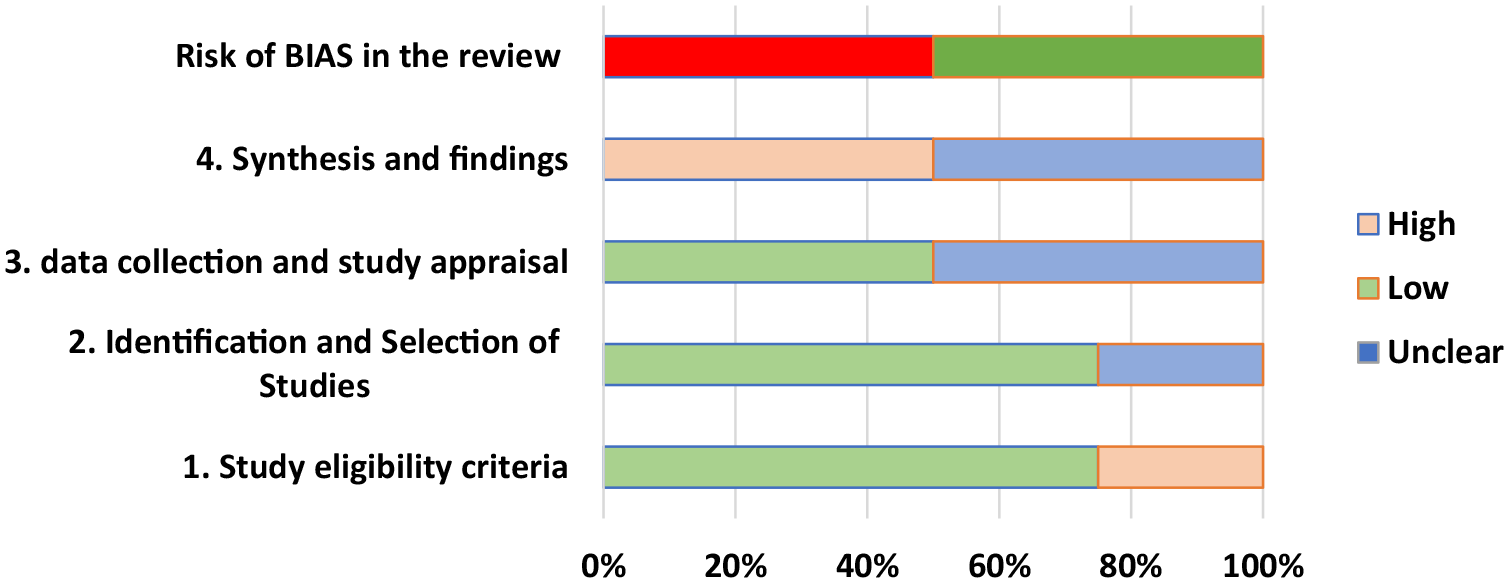
Risk of bias assessment with ROBIS tool.
Risk of Bias Assessment With ROBIS Tool.

? = unclear risk.
Acupressure Points and Interventional Protocol
In the intervention groups, participants were provided with acupressure-based treatments through either manual finger stimulation or the utilization of wrist bands. The specific length of time for which acupressure was administered using the fingers was found to be inconsistent across the various studies, ranging from a minimum of 12 minutes to a maximum of 30 minutes. Additionally, the application of acupressure on auricular points involved the use of different acupoints pressure, with the number of points applied ranging from 4 to 7. The maximum duration of acupressure application was found to be 5 days, with some studies implementing the intervention 30 minutes prior to chemotherapy administration. It is important to note that all patients in the studies received conventional treatment in the form of anti-emetic drugs. In addition, when it comes to the type of acupressure-acupoints intervention utilized in various studies, the majority of them focused on Neiguan (P6) points.1,18,26 -28,30,31 On the other hand, approximately 30% of the studies utilized auricular pressure.5,6,29
The Effectiveness of Acupressure for Chemotherapy-Induced Nausea and Vomiting
The result of this extensive and comprehensive review of 14 included publications with moderate to high-quality evidence. Acupressure is an effective complementary therapy in reducing and controlling chemotherapy-induced nausea and vomiting among participants with various types of cancer and receiving various types of chemotherapy. Two randomized controlled trial studies26,27 were conducted to examine the effectiveness of P6 acupressure in reducing chemotherapy-induced nausea and vomiting among patients with breast cancer undergoing doxorubicin chemotherapy; thus, the results showed that acupressure delayed chemotherapy-related nausea severity and delayed emesis and showed that acupressure significantly decreased the severity of vomiting among patients with breast cancer. Furthermore, there was a quasi-randomized controlled trial carried out in Taiwan that focused on patients with ovarian cancer. This study aimed to investigate the efficacy of auricular acupressure in alleviating various adverse effects associated with chemotherapy, including pain, fatigue, nausea, sleep disturbances, distress, shortness of breath, memory problems, loss of appetite, drowsiness, dry mouth, sadness, vomiting, and tingling. In this trial, the participants were provided with auricular acupressure treatment 3 times daily. The results of this study revealed that the 6-week intervention of auricular acupressure exhibited a noticeable reduction in side effects among women undergoing chemotherapy for ovarian cancer, with a moderate level of effectiveness. One noteworthy advantage of auricular acupressure is its non-invasive nature, as well as its self-managing aspect, making it a cost-effective approach for patients. 29
According to the patients with head and neck cancer, the 6 sessions of P6-H7 as 2 sessions per day for 12 minutes of acupressure (3 minutes for each point bilaterally) in the morning and evening, started from the second day of chemotherapy combined with conventional antiemetic medicine alone has been proven as effective complementary therapy in reducing nausea and vomiting. 30 As well, P6 (Neiguan) acupressure had a statistically significant impact on lowering the frequency and severity of nausea episodes among patients with myeloblastic leukemia who were receiving idarubicin and cytarabine chemotherapy. However, this study did not find any evidence to support the use of P6 (Neiguan) in reducing vomiting intensity. 28 Correspondingly, the findings of another clinical trial study revealed that applying pressure to the P6 point of the patient’s dominant hand for 3 days, starting the day before chemotherapy, significantly reduces nausea and vomiting severity among patients undergoing chemotherapy. 18 In addition, the effectiveness of applying acupressure on both sides of the body, specifically targeting the P6 and SP4 acupoints was shown as a successful approach for alleviating chemotherapy-induced nausea and vomiting among individuals diagnosed with lung cancer who have undergone cisplatin treatment. 31
Based on this review finding, auricular acupressure has a positive outcome in reducing nausea or vomiting among different types of cancer. But there is still inconsistency through applying auricular acupressure in conjunction with ear massage on patients with colorectal cancer. However, there is also statistically significant effectiveness in lowering the severity and frequency of nausea episodes using auricular acupressure in other chemotherapy patients. 1 Furthermore, evidence showed that auricular acupressure effectively reduces and controls chemotherapy-induced nausea and vomiting among participants with breast cancer; for instance, 2 randomized controlled trial studies5,6 were carried out to examine the effectiveness of auricular acupressure in breast cancer patients reducing chemotherapy-induced nausea and vomiting. Thus, the results indicate that in both the acute and delayed phases, the intensity and number of nausea and vomiting reduced significantly in the intervention group.
Side Effects of Acupressure
Out of all included studies in this review, it is worth noting that only 2 research studies that were included in this review have provided evidence of the occurrence of side effects associated with acupressure; These side effects include constipation, diarrhea, abdominal distension, tiredness, and headache, as reported by Chen et al. 19 Furthermore, another study conducted by Tan and her colleagues in 2020 5 revealed that adverse effects resulting from auricular acupressure (AA) were relatively mild to moderate in nature. Interestingly, it was observed that these side effects gradually diminished once the AA tapes were removed, without the need for any additional intervention aimed at treating these adverse effects.
Discussion
Chemotherapy-induced nausea and vomiting (CINV) represent one of the chemotherapeutic treatments’ major unpleasant side effects, impacting patients’ quality of life and therapy compliance significantly. In addition, CINV management is commonly inadequate, posing a serious clinical challenge for healthcare providers and chemotherapy patients.13,19,33 However, numerous limitations of pharmacological treatment had contributed to raise the utilization of complementary therapies or alternative nausea and vomiting management methods. Thus, there are several non-pharmacological alternative therapies commonly used to control nausea and vomiting among patients with cancer and receiving chemotherapy. 9
Acupressure is one of the most prevalent and effective alternative non-pharmacological interventions to manage chemotherapy-induced nausea and vomiting (CINV)1,5,6,26,27. Thus, the result clarified the objective of this comprehensive review study to find out the effectiveness of acupressure in reducing chemotherapy-induced nausea and vomiting among people with cancer. Furthermore, this systematic review elucidated that acupressure as a complementary therapy has a significant effect on reducing nausea and vomiting that caused by different types of chemotherapy and it is superior to conventional intervention that used in CINV. In addition, this study could find out the average duration time for each acupressure session and the number of sessions that are significantly effective for nausea and vomiting. In addition, this study provides a comprehensive summary of the acupoints that are frequently utilized and considered highly effective for acupressure treatment among patients suffering from cancer and experiencing chemotherapy-induced nausea and vomiting (CINV).
Based on the review findings, acupressure is an effective alternative intervention for minimizing and managing chemotherapy-induced nausea and vomiting among individuals with various types of cancer and receiving various types of chemotherapy. For instance, in a recent study conducted by Li et al in 2022, 32 the focus was on assessing and consolidating the most reliable evidence regarding non-pharmacological approaches for managing chemotherapy-induced nausea and vomiting (CINV); therefore, this study concluded that applying pressure on the Neiguan point has proven to be an effective method for reducing both the occurrence and intensity of CINV among patients with cancer. Additionally, the utilization of acupressure techniques has demonstrated the ability to alleviate acute and delayed CINV. These findings align with another study that investigated the use of various acupressure techniques as part of complementary and non-pharmacological interventions, effectively preventing severe nausea and vomiting among patients with breast cancer undergoing chemotherapy. 9
Acupressure in conjunction with antiemetic pharmacological treatment significantly reduces nausea and vomiting. Accordingly, Miao et al 17 conducted a systematic review and meta-analysis of 12 studies including 1419 patients which showed that acupressure plus antiemetics significantly reduced the severity of chemotherapy-induced acute and delayed nausea. Furthermore, the subgroup analysis found that the acupressure bands decreased the severity of acute nausea, while manual acupressure decreases the incidence of acute vomiting and delays nausea symptoms; accordingly, combining different protocols may have better outcomes. Notably, another systematic review recommended use of auricular acupressure (AA) as a complementary therapy for the management of CINV, especially for patients with breakthrough CINV; AA delays chemotherapy-induced nausea and vomiting as well as constipation, diarrhea, and tiredness; AA reduces some adverse reactions of antiemetic’s; however, AA alone or AA supplementation has little effect on acute nausea and acute vomiting. 19
Based on extensive research conducted in the field, it has become evident that there exists a significant gap in the existing body of literature when it comes to discussing the various negative side effects associated with the practice of acupressure. As an illustration, a study conducted by Chen in 2021 19 found a multitude of adverse effects related to acupressure, such as constipation, diarrhea, bloating in the abdominal region, fatigue, and headaches. Moreover, the research conducted by Tan et al 5 also shed light on the fact that mild to moderate side effects could emerge as a result of auricular acupressure (AA), although these effects were observed to gradually diminish upon the removal of the AA tapes, thereby eliminating the need for any further treatment to mitigate the occurrence of these side effects.
In the context of acupressure protocol, there is no standardization for the protocol and guidelines regarding the application of acupressure in terms of the number of sessions, duration time for each session, and even the number and sites of acupoints. Based on the findings of this review, the method of acupressure with fingers varied in duration, with a range of 12 to 30 minutes. Auricular points varied from 4 to 7 points with various seed pressure applied. The maximum duration of acupressure treatment was 5 days, with some studies beginning the intervention 30 minutes before the start of chemotherapy points.1,5,6,18,26 -31 Thus, there is a significant need for a standardization protocol to guide the acupressure intervention among chemotherapy patients who experienced nausea and vomiting.
Limitations
This systematic review has the following limitations to be considered: the unavoidable clinical heterogeneity between the existing studies, such as different cancer types, chemotherapy, antiemetic regimens, and sample size. The lack of standardized implementation of acupressure for cancer patients post-chemotherapy led to different clinical results. The quality of the existing evidence in this review was considered moderate because only 5 clinical studies were evaluated as at low risk of bias after assessment with ROB 2, no systematic review and meta-analysis study fulfilled all the AMSTAR 2 scale requirements, and only one included trial followed a double-blind study design. Therefore, further research might significantly impact the confidence of this systematic review study.
Conclusion
Employing acupressure in managing CINV for different types of cancer alone or with combination of pharmacological treatments is needed to enhance the quality of life among cancer patients. However, the scarcity of studies about how to effectively use acupressure and the major dependence on the easily accessible pharmacological options to manage CINV, contradict the use of acupressure, despite the well-known side effects of different pharmacological options. Indeed, among all other non-pharmacological options, acupressure can be easily learned and applied by health care providers or by patients themselves. In addition, acupressure is lower cost when it is compared with the widely used pharmacological treatment for CINV. So, the usage of acupressure must be encouraged in low-income countries that suffer from the burden for cancer patients and their treatment.
The usage of acupressure to manage CINV is still needs to be standardized and a well-established unified protocol validated for different types of cancers. So, a call for more studies that successfully evaluate acupressure with the different types of cancer is needed to pave the road ahead of its usage. Moreover, acupressure and other non-pharmacological and complementary methods for management of the different disease symptoms should be included in education curriculums and the continuous training programs for the different health professions. Courses and training about acupressure can be applied in different health care facilities, which will increase the dependence on it. This will be reflected in successful usage of this low cost and easily applied method with different types of cancer, which may increase the number of conducted studies.
Footnotes
Appendix A
Characteristics of Included Trial Studies and Review Studies.

| Author/ Year | Country | Sample Size | Study Design | Chemotherapy Rating | Chemotherapy Regimen /Diagnosis | Acupressure Point | TMT | Intervention /Control | Outcomes/Measurement |
|---|---|---|---|---|---|---|---|---|---|
| Augustine and Latha, 2015 | India | 20/40 | Quasi experimental, posttest with control group. | -Third or fourth cycle of radio sensitizer chemotherapy in case of weekly regimen and second cycle in case of 3 weekly regimen. | -Radio sensitizer chemotherapy -The majority of participants diagnosed with Head and neck cancer. |
(P6-H7) Pericardium -6 /P6, Heart −7/H7 | Acupressure was given by applying firm pressure using thumb. -Two session/day - 12 minutes of acupressure provided for 3 minutes for each point bilaterally in the morning and evening. - Three days started from the second day of CTX |
Intervention: Acupressure + antiemetic. Control Antiemetic |
The group that received acupressure treatment reported a significantly reduced level of nausea compared to the other group. |
| Avcı et al, 2016 | Turkey | 60/90 Band group:30. Pressure group: 30 |
RCT Parallel group |
First cycle of chemotherapy |
-idarubicin + cytarabine drugs -Myeloblastic Leukemia |
P6 (Neiguan) | The pressure group implemented a 15-minute application of pressure on each wrist, totaling 30 minutes in total before the CTX event. On the other hand, the band group had a P6 point wristband placed on their wrists, specifically 30 minutes before the CTX event, and this routine was repeated for 4 consecutive days. | Pressure + antiemetic. Band + antiemetic. Antiemetic |
There was a statistically significant difference observed in the frequency of nausea episodes and their severity within the intervention group. However, no statistically significant difference was found in the severity of vomiting. |
| Eghbali et al, 2016 | Iran | 48 total women | Crossover clinical trial design | Second cycle of chemotherapy | -Cisplatin and anthracycline -Breast cancer patients mild to severe stages |
Auricular acupressure | -Ear seed placed on ear point -pressing each point at least 3 times every day (morning, noon and night) for 3 min. -The ear seeds remained in their place for 5 days -After 21 days in second cycle the group were switched |
Antiemetic |
-Intensity & frequency of nausea and vomiting significantly decrease in intervention group in acute and delayed phase standard questionnaire with 16 items (7-degree Likert scale) |
| Said et al, 2016 |
Palestine | 42/126 Acupressure 42 Non -acupressure 42 Control 42 |
RCT Parallel |
Second cycle of chemotherapy | highly emetogenic chemotherapy ie, doxorubicin -Breast cancer diagnosis, stage of cancer I-III. |
P6 (Neiguan) | -Acupressure to P6 point (active) -Acupressure to nonacupoint (placebo (n = 42). A point on the dorsal side of both forearms, Four fingers’ breadth proximal to the proximal flexor palmar crease was used. -Group 3 usual care only (control) (n = 42). -Time and duration not mentioned |
Acupressure wristband non acupressure Sea-Bands +Antiemetic dexamethasone Antiemetic+ dexamethasone |
Acupressure delayed chemotherapy related nausea severity and delayed emesis. afternoon, evening, night) for 4 days |
| Shen and Yang, 2017 | Taiwan | 35/ 70 | Quasi-experimental research design | Received at least 1 cycle of chemotherapy. | Chemotherapy with cisplatin lung cancer patients receiving chemotherapy. |
PC6 and SP4 on both sides of the body | The program consisted of 3 minutes of acupressure each on points (total 12 minutes). The first session at 30 minutes before the chemotherapy, the second session before dinner on the day of chemotherapy, and the third session before breakfast 3 consecutive interventions in the next day. |
Acupressure PC6 & SP4 + antiemetic Antiemetic |
The severity of both nausea and vomiting showed statistically significant differences between the 2 groups, with the experimental acupressure group experiencing greater improvements compared to the control group. assessment of nausea and emesis (MANE) before each intervention session and 48 hours after chemotherapy. |
| Byju et al, 2018 | India | 20/40 | Quasi posttest control only | -At least 1 complete cycle chemotherapy | Chemotherapy cisplatin and others multi cancer Diagnosis | P6 point | Pressure at the P6 point of the patient’s dominant hand the first time before chemotherapy and Second time before lunch. Acupressure for the third one before dinner. |
Acupressure |
Acupressure is effective in reducing nausea and vomiting severity among patients receiving chemotherapy. - |
| Shin and Park, 2018 | Korea | 50 | Quasi-experimental design Pre-test-posttest non-equivalent control group. |
At least 2 cycles of chemotherapy | Diagnosed with colorectal cancer | P6 point | Tappan’s ear massage protocol stickers on 5 points on the ear (auricular acupressure) Benjamin points Six times in total (for 2 days). Auricular acupressure was applied to patients in the ward on the day after hospitalization (chemotherapy day) thrice per day for 2 |
The auricular acupressure was conducted with a combination of ear massage and attaching acupressure stickers. Not received any massage, and non-acupressure stickers |
The experimental group showed significantly lower nausea and retching than did the control group after receiving auricular acupressure. There were significant interaction effects between time and group on auricular acupressure on nausea and retching. There were significant interaction effects between time and group on auricular acupressure on total score of (Index of Nausea, Vomiting, and Retching). Measurement: the researcher adopted the Korean version of Rhodes and McDaniel’s Index of Nausea, Vomiting, and Retching (INVR) |
| Peoples et al, 2019 | USA | 161/242 participants | Randomized control trial Parallel |
First cycle | Doxorubicin based chemotherapy. Diagnosis: Breast cancer |
P6 point proximal to the distal skin crease of the wrist joint |
-Acupressure bands up to 5 days as needed to -Both enhancing and expectancy-neutral relaxation music MP3 recordings were 12 minutes in length with a background of soothing flute music and relaxation instructions with guided imagery based on a published script -Patients reported the severity of nausea 4 times each day morning, afternoon,evening, and night) over a 5-day period |
acupressure bands and expectancy-enhancing material material Only an expectancy-neutral handout without the mention of acupressure bands. |
After utilizing acupressure as a method to reduce nausea and vomiting, it was observed that patients in interventional group and who underwent doxorubicin treatment experienced lower levels of peak chemotherapy-induced nausea (CIN) compared to the control group. |
| Tsao and Creedy, 2019 | Taiwan | 34/65 | Quasi-randomized controlled trial | Third cycle of chemotherapy | Diagnosed ovarian cancer | Auricular acupressure seeds on the outer ear. | The 4-acupressure point’s, Vaccaria seed placed on each point attached with adhesive tape. The press on each point 3 times/day for 3 minutes per time (ie, morning, noon, and night) | Received routine care and auricular acupressure treatment. Received routine nursing care |
The severity of symptoms experienced by both groups was heightened. However, the application of auricular acupressure proved to be effective in alleviating side effects, including disrupted sleep patterns, feelings of fatigue, and loss of appetite. Anderson Symptom Inventory (MDASI) |
| Tan et al, 2020 | China. | 38/114 True AA group (n = 38). Sham AA group (n = 38). Standard care group (n = 38). |
RCT Parallel |
First chemotherapy cycle | Moderately high to highly emetogenic chemotherapy -Breast cancer patient’s I–III. |
Auricular (True acupressure in 7 points / less than 7 points in Sham acupressure) |
Seven acupoints were conducted from Day 1 to Day 5 of for the true AA and the sham groups. -Three times daily in; morning, afternoon, & evening, with each time lasting about 4 to 7 minutes |
Auricular + antiemetic Antiemetic |
Both the true and sham AA groups reported improved - |
| Miao et al, 2017 | China | Twelve studies with 1419 patients | Systematic review with meta-analyses and trial sequential analyses of randomized controlled trials. | --------- | --------- | --------- | --------- | Acupressure was used with or without antiemetic medications. Compared with antiemetic medications or nursing care |
The pooled results of the involved RCTs showed acupressure plus antiemetics significantly reduced the severity of chemotherapy-induced acute and delayed nausea. |
| Chen et al, 2021 | China | Contain 1449 patients. | Systematic Review and Meta-Analysis of randomized controlled trials of auricular acupressure; including crossover randomized design study | --------- | --------- | --------- | --------- | auricular acupressure with or without antiemetic medications Either placebo or antiemetic |
AA still played an important role in reducing delayed nausea and vomiting (delayed nausea frequency. |
| Pourfard et al, 2022 | Iran | Total of 952 patients | -Systematic review for fully randomized trial, a parallel control study design or a crossover studies. | --------- | --------- | --------- | --------- | Acupressure+ antiemetic Antiemetic |
Acupressure has shown promising results in mitigating severe nausea and vomiting in breast cancer patients receiving chemotherapy. Multiple research studies have explored different techniques and approaches to implement acupressure as a preventive measure in these individuals. |
| Li et al, 2022 | China | 22 articles | Systematic review of clinical decisions, guidelines, evidence summaries, recommended practices, systematic reviews, and expert consensus. |
|
|
|
|
Acupressure +antiemetic Antiemetic |
Acupressure has been proven to be highly effective in alleviating the symptoms of nausea and vomiting caused by chemotherapy treatment. |
Acknowledgements
The authors would like to express their utmost gratitude for the invaluable collaboration and unwavering support provided by Professor Jafar Alasad Alshraideh from the University of Jordan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.