
Abstract
Background:
Integrative oncology [IO] is sought-after by patients, endorsed by clinical guidelines, and valued within National Cancer Institute Centers. Shared Medical Appointments [SMA] leverage health education and social connection to deliver enhanced patient experience, population health, cost-reduction, and clinician well-being. Integrative Oncology Shared Medical Appointments increase access to integrative medicine but delivering these services via telehealth have not been evaluated.
Objective:
We created, and pilot tested a Virtual Integrative Oncology Shared Medical Appointment Series (VIOSMAS) to assess its feasibility, acceptability, and efficacy at an urban academic teaching hospital.
Methods:
The 7-session hour-long Living Well with and after Cancer series included didactics, multi-disciplinary experiential sessions, and group discussion. Topics included (1) Introduction, (2) Herbs/Botanicals/Fungi, (3) Mindful Movement, (4) Acupuncture, (5) Narratives and Nature, (6) Diet and Culinary Medicine, and (7) Vitamins/Supplements. Virtual visits via telehealth were offered to enhance patient participation during the pandemic. Outcome measures included recruitment, retention, pre/post-series patient survey and qualitative clinician feedback.
Results:
Between 9/2021 and 4/2023, 72 unique patients were recruited to 5 cohorts and had a total of 332 VIOSMAS visits. A total of 50 patients (69%) attended 4 or more of the 7-session series; 60 (83% were women); patients ranged in age from 28 to 93 years (median 66); 36 (50%) lived outside the city center; the most common cancer diagnoses were breast, lymphoma, and lung cancer. Patients were from diverse demographics. Pre-program, patients reported desiring assistance in addressing diverse symptoms including fatigue, insomnia, pain, gastrointestinal (GI) symptoms, anxiety, and depression. Post-series, patients reported that the VIOSMAS addressed their goals and symptoms; they also reported incorporating recommended lifestyle changes in diet, exercise, sleep, and stress management; they were satisfied with the number of sessions and telehealth format. The participating clinicians reported high levels of satisfaction with VIOSMAS. Revenue to the institution from VIOSMAS exceeded the revenue potential of equivalent time spent for individual visits while supporting extended physician-patient contact.
Conclusion:
VIOSMAS is feasible for patients and clinicians, addresses patients’ symptoms and questions about lifestyle and complementary therapies, and generates more revenue than individual visits. Larger implementation trials with appropriate comparison groups are recommended.
Keywords
Background
Shared medical appointments (SMA), also called group medical visits, have increased in popularity over the past 50 years as an innovative approach to improve health education and social support, access to care, and clinician well-being without increasing the cost of care.1 -11 Integrative SMA add complementary and integrative health (CIH) care education and services to existing SMA models 12 and may increase patient access to CIH services often inaccessible due to limited insurance coverage 6 and high out-of-pocket costs. 13 They may also advance health equity by serving patients negatively impacted by health and health care disparities.3,5,14,15
While telehealth can improve access to care for underserved patients for conditions such as chronic pain, and became routine during the pandemic,16,17 few studies have evaluated their feasibility and impact on oncology patients and clinicians. 18
Integrative oncology19,20 is highly sought-after by patients,21,22 endorsed by clinical guidelines,23,24 and part of National Cancer Institute-Designated Comprehensive Cancer Centers.25 -27 In 1 study in a large, urban, academic oncology clinic, 90% of CIH non-users were interested in gaining more information, and 70% wanted their primary oncologist to provide information about lifestyle and complementary care options and discuss their safety and potential benefit in managing cancer and associated symptoms. 2 This care model holds significant potential for addressing patient medical and psychological needs, enhanced communication, 28 improved patient outcomes, and costs4,29,30 for oncology patients.
What Is Known About Integrative Oncology SMA?
In the first published study that examined the implementation of integrative SMA, among 32 patients, predominantly white higher income women, with an average age of 52, a range of cancer diagnoses (mostly commonly colorectal and breast), including stage 3 or 4 disease and active cancer treatment, the SMA was found to be a feasible and promising model to increase access to IO services. 4 An online mindfulness-based group program was also found to be feasible and acceptable for metastatic gastrointestinal oncology patients and caregivers. 31 A mindfulness based smoking cessation group visit was found to be feasible and acceptable in a small group (n = 10) of low SES and minority smokers with cancer. 3 In another study, group acupuncture at a cancer institute improved access and affordability. 5 Men with prostate cancer (average age 62 years, n = 26) on active surveillance found SMA to be acceptable. 30
What Is Not known?
Current gaps in knowledge and questions remain on feasibility with diverse oncology patient populations and virtual delivery.
The purpose of this study was to investigate (1) Is a 7-session telehealth VIOSMA feasible in terms of recruitment and retention of patients? (2) How well does the VIOSMA meet patients’ goals for lifestyle and complementary integrative therapies for common symptoms? (3) How satisfied are participating clinicians with VIOSMA? (4) Is VIOSMA financially sustainable, that is, do institutional charges for services meet or exceed those generated by typical in person individual visits? Our rationale for implementing VIOSMA at our institution was to introduce and educate patients on the various integrative services we provide, improve patient access to physicians, increase consecutive visits, support continuity of care, provide affordable care, offer group support, improve physician efficiency and productivity, and leverage the health benefits of social connection.
Methods
This was a prospective cohort pilot study at Weil-Cornell Medicine-NY Presbyterian’s Integrative Health and Wellness Center from September 2021 to April 2023.
Patients were eligible if they were adult oncology patients of Weill Cornell Medicine-New York Presbyterian, English speaking, and had internet access.
Clinicians were eligible if they were a part of Weill Cornell Medicine-New York Presbyterian Integrative Health and were certified in an Integrative Oncology related field.
Recruitment: Invitations were made through patient flyers, referrals from integrative medicine clinicians, referrals from institution primary care providers and specialists, hospital events page, email blasts, word of mouth/patient testimonials, grand rounds presentations, and community outreach programs.
Intervention
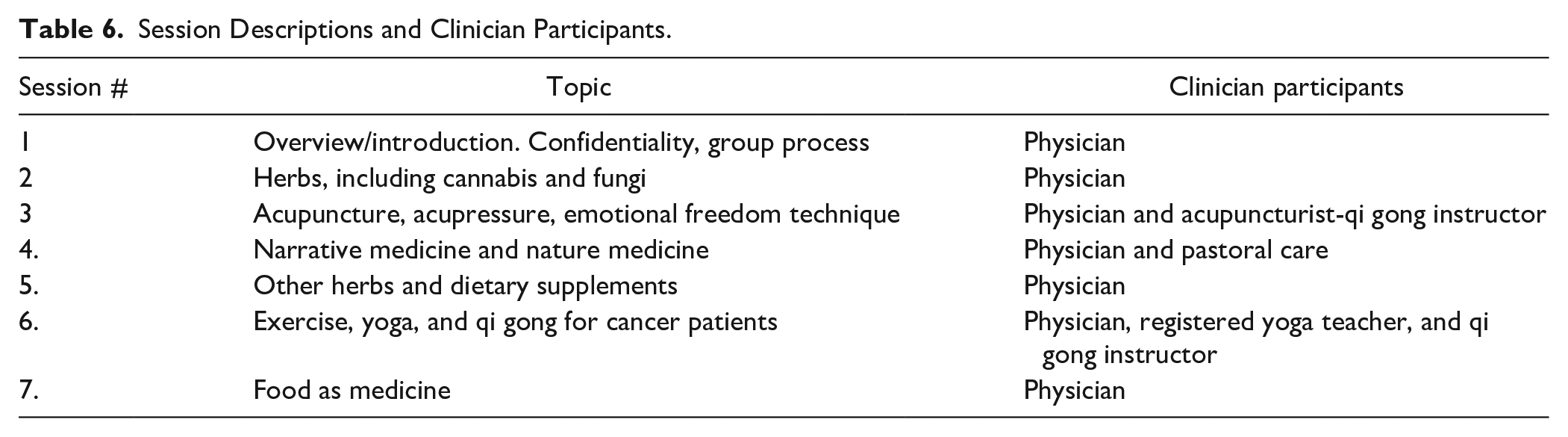
The 7-session hour-long Living Well with and After Cancer (LWWAC) Virtual Integrative Oncology Shared Medical Visit Series (VIOSMAS) combined didactics with multi-disciplinary experiential learning in nutrition, culinary arts, herbs/botanicals, exercise, yoga, qi gong, acupuncture/acupressure, mindfulness, and narrative medicine. The telemedicine sessions were created and led by an integrative medicine physician-acupuncturist with 2 of 7 sessions involving other interprofessional clinicians (qi gong instructor/acupuncturist, yoga therapist, and pastoral care physician). Each 1-hour session consisted of a review of the small group confidentiality agreement, distinct didactic content, demonstration/experiential, and question/discussion time. The session topics included: (1) Overview; (2) Herbs, Botanicals, Fungi, and Medical Cannabis; (3) Acupuncture, Acupressure, and Emotional Freedom Tapping; (4) Narrative Medicine and Nature Medicine, (5) Vitamins and Supplements; (6) Joyful Movement, Yoga, and Qi Gong; (7) Nutrition/Culinary Medicine.
Individual check-ins were done periodically prior or after the SMA via physician/patient call. For most weeks, especially at the beginning of the series, the physician would call each patient prior to the group visit for a brief check-in. During the series, most of the patients would have either seen the integrative physician, another integrative physician in the practice, or one of their oncologists at least once. Electronic medical record notes were reviewed at each group medical visit for coordination and continuity of care. Generic advice was given during the didactic portion of the group, and individualized advice based on diagnosis was provided during one-on-one consultation call and documented in the electronic health record. Participants were informed at the first session that the goal of the SMA was to present IO information to a larger number of individuals at 1 time and not to serve as a support group. Although patients reported enjoying informal peer interaction, this was not the primary focus. Following the SMA, digital health resources and links based on questions from the discussion time were sent by the physician to patients through an email from the group visit coordinator. Following the SMA, patients were also given complimentary access to yoga/somatic therapy videos (including English, Mandarin, and Spanish meditation resources), qi gong video, and other supportive digital health resource links.
Documentation of the SMA visit along with individual medical management and customized recommendations and treatment plan, was completed by the physician with billing based on decision making complexity. Individual patient SMART goals were included in the SMA documentation as were links between integrative modalities and individual diagnoses. The creation of detailed, customized visit templates (purpose, group interventions utilized, and topics discussed) for each session greatly facilitated the electronic charting needed to generate billing information.
Implementation
The standard operating procedure was to target 2 times the final group size (maximum 15 patients/provider). The group visit coordinator communicated with patients through phone, email, and the patient portal. The SMA coordinator’s role was to contact interested patients, verify insurance, set up and disseminate the zoom link, and send follow up resources to patients. SMA sessions were scheduled 2 weeks apart to allow patients to make changes based on what they learned in prior sessions and to share the impact of these modifications. Electronic pre and post surveys using Qualtrics were sent via email from the SMA coordinator to participants at time of enrollment and after each series. Responses to the 5-question pre survey and 10-question post surveys were optional and completely voluntary. No incentives were available or offered. Surveys were written in English, however, all participants in this pilot were fluent in English. Additional qualitative feedback data from participating interdisciplinary professionals was also gathered.
Data and Outcome Measures
Sources of data included patient demographics and post survey evaluations, qualitative data, and materials from the program development process. Brief interviews with the integrative medicine physician-acupuncturist were completed with the co-moderators (yoga therapist, qi-gong-acupuncturist, and pastoral care physician) after co-led sessions without patients present. These interviews facilitated iterative processing of what was working and areas of improvement. Materials were created in the process of developing and implementing the SMA, including e-mails, fliers. Descriptive data were collated, and means were calculated in Excel. Financial efficiency of the SMA program was calculated by comparing the billing practices used in typical 1-hour individual consultations with the same amount of time spent seeing patients in SMAs. Mathematical cost-benefit modeling at our practice demonstrated that SMA can be financially sustainable and possibly even a net income generator for the institution. With our payor mix of 40% Medicare, 60% Commercial insurance and complexity of patients, cost neutrality for SMA was achieved when each group enrolled an average of 8 pts with an enriched staffing model (eg, MD + yoga therapist) or 5 patients when groups were staffed by a single clinician (eg, MD). We estimate a no-show rate of 20%, although as seen with data from first cohort, our no-show rate was lower. Costs for the support staff (administrative coordinator at $40/hour) were included as well as pre-visit and post-visit charting work for MDs.
Results
Recruitment and Retention: Between 9/2021 and 04/2023, 72 patients were recruited, of whom 51 (71%) completed the online pre-program survey. The 72 patients divided into 5 groups (cohorts) attended a total of 332 VIOMAS visits. Most (N = 60) participants were women and most (N = 53) reported Caucasian race; the median age was 66 years (Table 1). Median cohort size was 14 (range 7-25). About 50 (69%) attended at least 4 of the 7-session series, with 31 (43%) attending 6 or 7 sessions (Figure 1).

Patient recruitment and retention.
Patient Description.
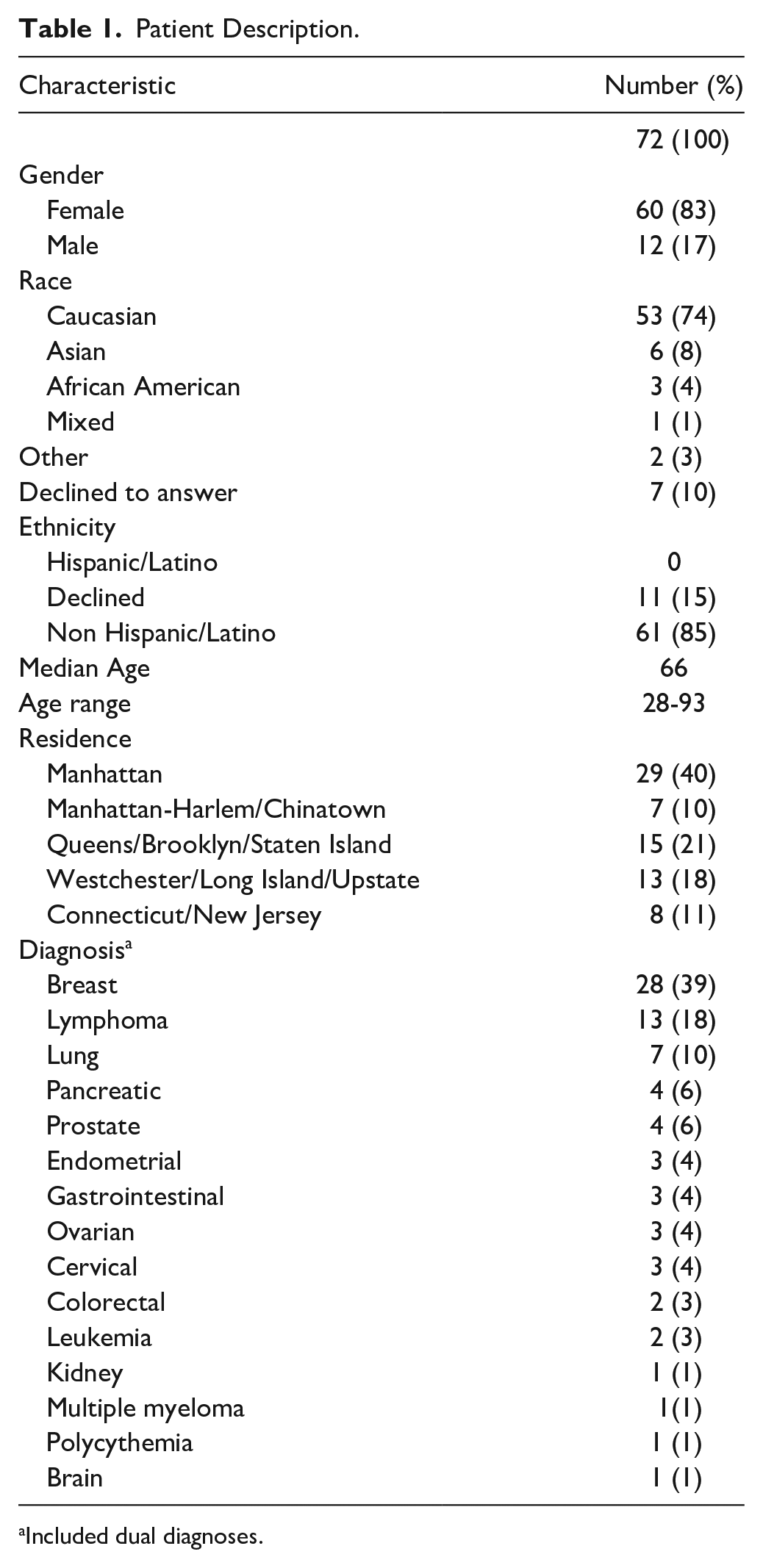
Included dual diagnoses.
Before the program, patients reported a variety of symptoms and side effects (Table 2), most commonly fatigue (30/51) and stress (25/51) Pre-program (n = 51), patients reported fatigue (n = 30), stress/irritability (n = 25), insomnia (n = 21), anxiety/fear (n = 19) weakness (n = 15), pain (n = 15), nausea/vomiting/constipation/diarrhea (n = 12), brain fog (n = 11), and sadness/depression/hopelessness (n = 10). Patients’ priorities for the program included relief from these symptoms or side effects, information about lifestyle (eg, diet, exercise, and stress management) and complementary therapies (eg, acupuncture, yoga, aromatherapy, and herbs/dietary supplements), preventing recurrence, and survivorship. Patients desired guidance over areas of their life perceived to be under their control including meal planning, sleep, herbs, exercise, everyday routines, and mental support. They desired to “feel more in control of healthcare,” “empower self,” “get back on feet,” “reverse old life,” “change daily routine,” and “conceptualize living” (Table 3).
Patients’ Symptoms/Goals and How Well They Were Addressed by the Program.

Nausea/vomiting/constipation/diarrhea.
Topics of Interest Pre-Program.

Post-series (n = 14), patients reported VIOSMAS addressed and improved sleep, fatigue, anxiety/fear, irritability/stress, gastrointestinal symptoms, and pain/weakness. Patients reported incorporating dietary changes, regular exercise, meditation, mindful breathing, yoga, self-acceptance, stopping supplements, sleep-prioritization, and addition of beneficial foods (mushrooms, yogurt, and green tea).
Patients were satisfied with the program with 93% reporting goals were met, 93% recommending to others, 79% reporting 7-sessions being perfect length. About 21% preferred more. Half of the 72 patients (n = 36) directly benefited from remote delivery as they lived in boroughs and counties outside city center. A total of 22 patients (31%) lived in underserved locations. All patients reported remote delivery acceptable with no patients requesting in-person group visits. The flexibility to access care at convenient times (lunch hour or at the end of the workday) made it easier for patients to participate. Regarding implementation, the combined didactics with experiential was enjoyed by patients. Patients most valued evidence-based research, physician warmth and knowledge, extensive information (self-care and symptom/recurrence risk reduction), comprehensive/novel approaches, and the positive group dynamic. Patient suggestions for improving future programming included more food as medicine and hands-on demonstrations, tai chi/yoga demonstrations, take-home fact sheets, meal plans, recipes, and pre-session emails.
Patients’ Qualitative Feedback
Regarding implementation, the combined didactics with experiential was enjoyed by patients.
Patients described a positive group dynamic, with group encouragement and affirmation of personal goals enhancing their sense of self-efficacy. The scheduling of SMA sessions 2 weeks apart seemed optimal to allow patients to make changes based on what they learned in prior sessions and to share the impact of these modifications.
Clinician Feedback
The integrative medicine physician was present at every session. For 2 of the sessions, 3 other interprofessional clinicians (pastoral care physician, yoga therapist, qi gong teacher/acupuncturist) co-moderated the 1-hour sessions. Clinicians were part of Integrative Health staff; therefore, no additional FTE was required. The physician and interprofessional clinicians reported high levels of satisfaction with VIOSMAS and found it to be a sustainable option from the clinician perspective.
Telehealth Implementation and Access
The flexibility to access care made it easier for patients to participate. Patients with limiting physical conditions or immunocompromised states appreciated the ease and safety of “gathering” and building community. All our patients were able join via phone or computer. In addition, the coordinator and physician would routinely call patients ahead of time to confirm attendance. If any discomfort with or access to technology was detected, technology guidance was provided. Several of our patients joined from free internet hotspots (such as libraries, community centers, or cafes).
Discussion
Our pilot confirmed the existing literature suggesting potential benefits of SMAs to patients, clinicians, and institutions. Recruitment and allocation to groups was feasible, but there was high rate of patients’ non-response to surveys after the program. Patients who did respond expressed favorable opinions about the program as did participating clinicians, and financial projections indicate that this is a sustainable model.
Patient Benefits
Patient-reported benefits both from the literature and in our SMAs included social bonds,32,33 peer support,32,34 patient and caregiver health literacy, 10 patient self-efficacy and self-agency, 10 reduction in isolation, and extended clinician-patient contact time.
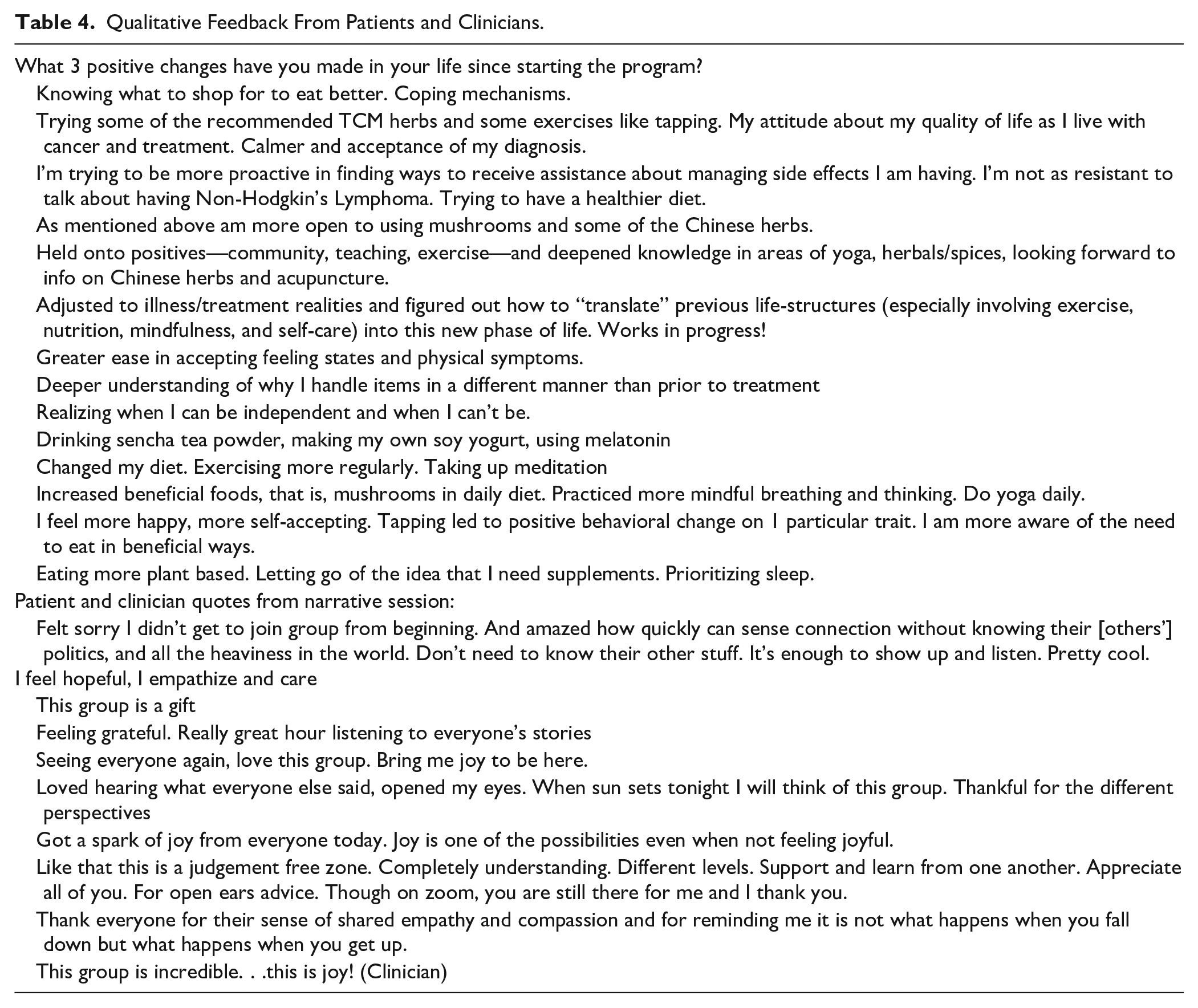
During the question/discussion time, mutual sharing about disease self-management, behavior change tools, lifestyle interventions resulted in patients being inspired by peer adaptive coping strategies and development of patient/provider equitable relationships. 35 Co-participants (patients and providers) connected, and patients noted that any cultural or socio-economic differences receded (Table 4-quotes).
Qualitative Feedback From Patients and Clinicians.
Social support, social networks and support groups can be protective against mortality36 -38 with survival improvements in cancer populations.39 -42 While our study did not capture this longitudinal data, frequently group members would voluntarily connect with peers outside of the SMA as they found the relationships supportive. Patients would ask to exchange emails or phone numbers through the chat voluntarily. Some would arrange for walks together. This was not facilitated by SMA providers.
Clinician Benefits
Clinician-reported benefits cited from the literature and reflected in our SMAs included extended time with patients, 9 ability to provide team-based care, 9 deeper understanding of patients’ social context, increased efficiency, decreased clinical burnout, 10 sense of purpose8,9,11,43 and deepened collegiality especially with interprofessional collaboration.44 -48 In our SMA series, LAc/Qi Gong instructor, yoga therapist, pastoral care physician and group medical visit coordinator enjoyed taking on expanded roles within VIOSMA alongside the integrative medicine physician-acupuncturist with deepened mutual appreciation and rapport. The fourth aspect of the quadruple aim in health cancer systems was achieved with our clinicians experiencing higher clinician morale, sense of purpose, productivity, and rapport.
Institutional Benefits
Institutional benefits reported from the literature include increased access to care,4,5,49 increased affordability,14,50,51 patient retention, staff retention due to practitioner job satisfaction,8,52 employee wellness, 53 and medical education. 54 While calculation of these benefits was not possible in this short pilot, our practitioners reported high satisfaction in participating in the VIOSMA and enjoyed the change in pace from 1:1 patient care. Patients reported appreciating increased access to integrative physician care. Very few academic institutions, to our knowledge, offer insurance based integrative oncology group medical care and our patients appreciated this opportunity. Medical students, residents, fellows, and physicians (both within and outside our institution) regularly requested to observe either as part of an integrative medicine rotation or elective.
SMA can be financially sustainable and possibly even a net income generator for the institution. For our institution, group visits were a financially viable alternative to individual IO visits. It was more efficient for a provider to see patients in SMAs rather than spending that time in private 1-h consultations and extended clinician-patient contact time. The revenue to institution from VIOSMAS exceeded the revenue potential of equivalent time spent for individual visits while supporting extended physician-patient contact. While not all patients attended all 7 visits and the payer mix varied from series to series, the revenue from group visits significantly exceeded the revenue potential compared with the same amount of time spent in individual visits, particularly if there was a minimum of 5 to 8 patients (Tables 5 and 6).
Cost/Revenue Forecasting.

To estimate the true cost of the SMA, you can calculate the hourly rate of non-revenue generating providers and administrative support. For example, in an SMA run by MD and yoga therapist, yoga therapist hourly cost $60, administrator cost $40 per hour.
Session Descriptions and Clinician Participants.
An average of 15% of the patients who present to Integrative Health are brand new to our institution and frequently request for referrals to other subspecialists at our institution. Additional downstream revenue includes referrals for physical therapy, labs, imaging, and other primary care/subspecialist physician care within the institution. Overhead cost with virtual SMAs was minimal. The only administrative costs are associated with scheduling and are accounted for in the mathematical forecasting. We have had no SMA specific insurance denials.
Minority Access
Accessibility of CIH is a concern. Bari et al 2 reported that most underserved minorities with cancer were interested in gaining more information from reputable sources (their oncologist) and to learn about the safety and potential complementary benefit in the management of cancer and associated symptoms. For those who used CAM therapies (only 16% in their study group) the most used CAM modality was meditation (56%), followed by herbal remedies (31%), yoga (31%), and acupuncture (12%) with all users reported benefit from CAM use. Emotional wellbeing was the most common benefit followed by improvement in treatment related adverse effects, chemotherapy related symptoms, pain, and sleep.
Our population included minorities (26% non-White) and both interest and response mirrored Bari’s study. The telemedicine delivery format allowed patients from surrounding boroughs to participate (half of our participants), many of whom were minority or undeserved, and future goals include Medicaid enrollment of providers to expand access. Future goals also include partnering with medical center Patient Family Advocacy Council members to expand non-English patient materials beyond the meditation recordings that we currently offer to patients (in Mandarin Chinese and Spanish).
Telehealth Delivery and Access
Telehealth has been associated with cost savings to patients, with 1 study estimating $147 to 186 per visit) 55 and time savings (2.9 hours driving time, roundtrip) and can be important especially from a diversity, equity, inclusion standpoint. Savings can be used by patients and caregivers for other things while mitigating the financial burden of cancer care and associated stress (financial toxicity). The NCI has prioritized this and supports research on the use of telehealth in cancer care through its 4 Telehealth Research Centers of Excellence (TRACE). 56 Many of our patients who benefited from telehealth visits live in boroughs and counties outside Manhattan (city center). While limited access to internet/devices or low digital literacy are health equity challenges, efforts were made by physician and coordinator to confirm attendance through phone call, screen for discomfort with or access to technology, and provide guidance. Beyond increasing access to underserved populations, virtual delivery expands access to patients with limited physical conditions or immunocompromised states.
Program Assessment and Revisions
Patients were interested in follow-up sessions, more yoga classes, further reading, research updates, additional information on food as medicine, meal plans, recipe ideas, and checklists for healthy foods. Recommendations made by the earlier cohorts were often implemented in subsequent cohorts, such as providing meal plans, recipe ideas, checklists, and more frequent yoga sessions. Although 5/7 sessions included food related topics, our patients, requested more information on food as medicine. Participants enjoyed and requested for more culinary medicine “hands-on food prep,” qi gong, yoga, meditations, and experientials. In response to iterative feedback, patients were encouraged to attend separately initiated non-oncology specific SMAs such as lifestyle medicine, women’s health, mental health or community events (walks, farm-to-table culinary events) for additional support.
Facilitators
Factors that contributed to the success of the VIOSMAS included program team credentials and expertise, staff passionate about the cause, dedicated team members (included medical secretary), strong rapport with patients, sense of community, peer support/social connection, and diverse age group of patients and multi-credentialed working group (MD/Acupuncturist, Acupuncturist/Qi Gong, and Yoga Therapist/Somatic Therapist) In addition, the hybrid/virtual insurance model (not grant/philanthropy supported) and adjunctive role of the SMA (not a substitute for 1:1 visits) aided in program advancement. Finally, the multi-disciplinary collaborative relationship with oncology departments (grand rounds invitations, tumor board invitations, patient feedback to oncologists, and referrals) provided a steady stream of interested patients.
Barriers/Challenges
Initial challenges included administrative resources, clinician time, billing/insurance coverage questions, digital access, patient demand, and last-minute cancellations.
Adaptations/Lessons Learned
Based on lessons learned, we made adaptations including having 1 administrative point of contact (medical secretary dedicated as group visit coordinator) who sets up links, organizes schedules, troubleshoots technology issues, sends weekly reminder emails, and provides online platform instructions to patient. The coordinator distributes the welcome packet including insurance/billing information. After each VIOSMA, a follow up email with resources, educational content, links, recipes are sent. Clinician time is blocked for program development and documentation. Some SMAs have been scheduled during evenings and weekends.
Future Directions
Scaling up the program will require recruitment (eg, nurse practitioner, mental health, pharmacist, chef). Future considerations to train other physicians (adolescent medicine and hematology/oncology) is important both for patient care and research. Providers are being enrolled in Medicaid to expand access. As interest for in-person visits increases, a hybrid option can be considered. Exploring partnership with Human Resources to offer SMA for employee health can contribute toward the quadruple aim. Community collaborations including children/families will benefit the next generation. If funds allow for a research/practice coordinator to help with program administration, baseline symptom assessment and demographics, program evaluations, and note-taking would aid in efficiency.
Limitations
SMA implementation examined in this study had several limitations. First, only 14 patients responded to the post-study questionnaire. This is a significant limitation in terms of reporting patient benefits from the program. The small number of patients suggests that responses could have come preferentially from patients who had positive experiences in the group. This would bias the results. Second, the study pilot sample may not be representative of patients with cancers served by Weill Cornell Medicine New York Presbyterian (WCM NYP). WCM NYP including NYP-Queens, NYP-Brooklyn cares for many non-English-speaking patients, but the VIOSMAS program was limited to patients fluent in English. All materials were provided in English as all our patients were English speaking; however, no specific health literacy review was made of patient facing material and should be considered for the future. The study sample may also include patients from higher income households consistent with other integrative clinics at academic medical centers, although we did have a significant number of patients who lived outside of the city center. In general, our program demographic skews toward more older women compared to the overall demographics of the cancer center. Specific efforts to recruit more diverse groups of patients to the SMA are planned with WCM One Meyer Cancer Center. 57 Existing literature demonstrates that SMA models can benefit both health outcomes and patient experience for patients from a wide range of racial/ethnic and socioeconomic backgrounds and have been implemented in languages other than English.58 -60 Proactive recruitment and streamlined referrals are needed to improve access among the racial and socioeconomic disparate populations.
Recommendations for Future Research
Well-controlled studies comparing SMAs to individual usual care visits should be conducted with endpoints including knowledge, patient and staff satisfaction, clinical outcomes, treatment adherence, financial data, insurance coverage data, office efficiency, process measures, resource utilization, and health care utilization (hospitalizations/emergency room visits, Accountable Care Organizations, and Value Based Care). Future research and implementation efforts could examine health outcomes over time after participation in GMVs, as well as the feasibility of using this model with more diverse patient populations.
Conclusion
Using a pre-post design, VIOSMA demonstrated feasibility and acceptability for urban oncology patients with high and consistent attendance over time among a mixed demographic (diagnosis, age, gender, race, and location), satisfaction with SMA topics/modalities, goals, and preliminary efficacy evaluating symptoms addressed, symptom improvement, and lifestyle changes. SMA was acceptable to providers/institutions and feasible/sustainable with time, cost, and referral benefits. Interdisciplinary co-facilitation increased deepened clinician collegiality, sense of purpose, productivity. Access to integrative oncology services (including minority populations) increased with satisfaction, feasibility, and sustainability reported by patients and providers.
VIOSMAS among a mixed demographic is feasible, acceptable, sustainable, cost effective to patient, providers, institutions and shows preliminary efficacy in this pilot. VIOSMAS provides valuable knowledge and insight into the use of this unique model for integrative oncology care. Larger methodologically sound implementation trials with longer follow-up periods and appropriate comparison groups are recommended.
Footnotes
Acknowledgements
We wish to recognize all the patients affected by cancer who participated in VIOSMA and provided evaluation data for this report. We also wish to acknowledge Mary Acosta for her administrative support and Anne-Marie Audet MD, Lisa Tatham RYT-500, Tim Fatato MA for their roles in the VIOSMA. We wish to thank Kathi J. Kemper, MD, MPH for her substantive review of the manuscript.
Contributions
Dr. Loy conceptualized and designed the study, coordinated, and supervised data collection, collected data, conducted the initial analysis, drafted the initial manuscript, reviewed, and revised the manuscript. Dr. Parikh reviewed the manuscript. Lauren Prisco assisted in the data analysis. All authors approve the manuscript as submitted and agree to be accountable for all aspects of the work.
Data Availability Statement
Data used in this program evaluation will be made available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The WCM Institutional Review Board (IRB) determined on 31 January 2023 (#23-01025565) that this activity is not considered research involving human subjects due to its anonymous, retrospective, program evaluation nature and that further IRB review and approval is not required.