
Abstract
Objective:
This trial examined the effects of proximal/distal mediators and moderators of an Active Music Engagement (AME) intervention on young child/parent distress, quality of life, and family function outcomes.
Methods:
Child/parent dyads (n = 125) were randomized to AME or Audio-storybooks attention control condition. Each group received 3 sessions with a credentialed music therapist for 3 consecutive days with data collection at baseline, post-intervention (T2), and 30-days later (T3). Potential proximal mediators included within session child and parent engagement. Potential distal mediators included changes in perceived family normalcy, parent self-efficacy, and independent use of play materials. Potential moderators included parent/child distress with prior hospitalizations, parent traumatic stress screener (PCL-6), and child age. Outcomes included child emotional distress and quality of life; parent emotion, traumatic stress symptoms (IES-R), well-being; and family function. Mediation effects were estimated using ANCOVA, with indirect effects estimated using the percentile bootstrap approach. Moderation effects were tested by including appropriate interaction terms in models.
Results:
No significant mediation effects were observed. Child distress with prior hospitalizations moderated AME effects for IES-R intrusion subscale scores at T2 (P = .01) and avoidance subscale scores at T3 (P = .007). Traumatic stress screener scores (PCL-6) moderated intervention effects for IES-R hyperarousal subscale scores at T2 (P = .01). There were no moderation effects for child age.
Conclusions:
AME is a promising intervention for mitigating traumatic stress symptoms and supporting well-being in parents of children with cancer, particularly for parents who screen high for traumatic stress and whose children are more highly distressed with hospitalization.
Keywords
Cancer and its related treatment are highly stressful and potentially traumatic life events for young children with cancer and their parents.1 -4 Cancer treatment can be especially difficult for young children due to their development. Immature logic can result in young children feeling responsible for their illness, and places them at risk for misinterpreting repeated hospitalizations, invasive medical procedures, or separation from family members due to treatment as punishment.2,5 Limited understanding of illness and treatment, inability to fully communicate feelings due to emerging language skills, and a more limited set of coping strategies contribute to increased vulnerability for traumatic stress symptoms (TSS) post-treatment.1,2,6 -8 Parents may also experience trauma as they witness their child’s distress, experience helplessness, and struggle with their own emotions as they strive to provide reassurance to their child.1,3,9,10
The emotional distress experienced by young children and parents is interrelated, prevalent, and often severe, with evidence suggesting that young children may experience more distress than older children.2,11 -13 Parents also experience heightened anxiety and depressed mood, with 40% to 83% reporting TSS within the first month of their child’s diagnosis (18%-33% at 6 months; 7%-27% >10 months post-diagnosis). 4 The immediate impact of parent distress includes changes in parent-child interaction and diminished parent confidence in their ability to support their child during treatment (self-efficacy), overall family function, and quality of life.3,4,12,14 -17 Despite these concerning symptoms, there are few empirically validated interventions for this age group and even fewer use a dyadic approach. 18
Music therapy has become a standard palliative care service in many pediatric hospitals, with a growing body of research that supports the use of active music making interventions to reduce distress and improve well-being in young children with cancer.19 -22 However, few studies have evaluated the mechanisms by which music therapy interventions work, limiting the evidence available to inform clinical decision making and evidence-based care.23 -26 Based on Robb et al’s Contextual Support Model of Music Therapy (CSM-MT), we developed and tested the music-therapist led Active Music Engagement (AME) intervention, establishing it as a feasible/acceptable intervention that reduces distress-related behaviors in young children hospitalized for cancer treatment.27 -29
Primary aims of this NIH funded multi-site mechanistic trial were to examine mediators (proximal and distal) and moderators of intervention effects. We examined 2 proximal mediators (child engagement; parent engagement with their child) and 3 distal mediators (perceived family normalcy; parent self-efficacy; independent use of music play materials). For moderation, we examined child and parent distress with prior hospitalizations, parent traumatic stress screener scores, and child age (Figure 1).
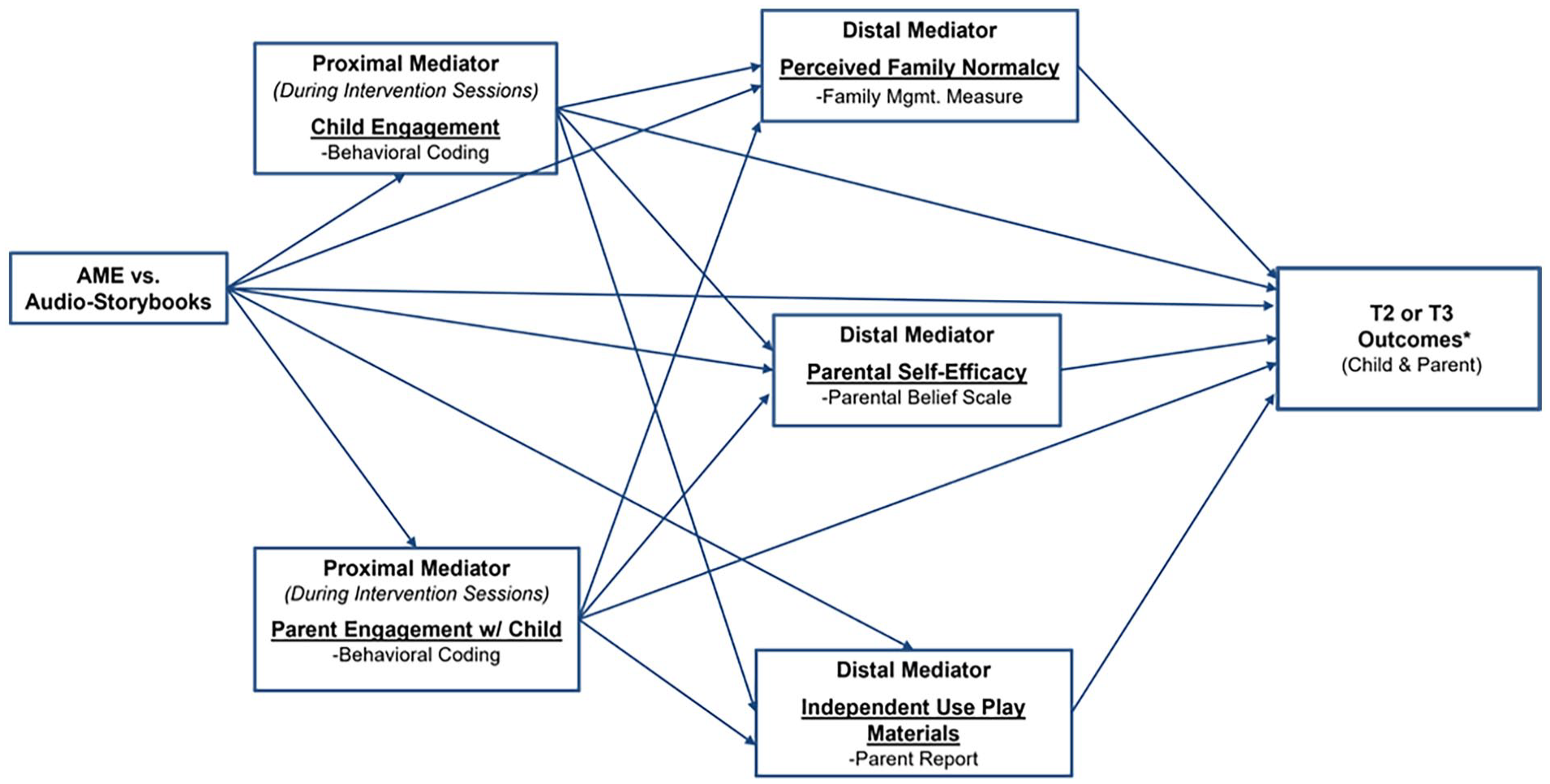
Hypothesized path model.
Methods
Participants
We obtained scientific and intuitional review board approvals and recruited participants from 4 Children’s Oncology Group institutions. Parents/children were recruited as dyads, requiring consent from parents and assent from children ≥7 years of age. Eligibility criteria included children aged 3 to 8 years at enrollment, an expected treatment course of at least 3 days to receive moderate to high intensity chemotherapy (in-patient or outpatient), and one parent (or person serving as primary caregiver) aged ≥18 years who could be present for all sessions. Exclusion criteria included parent unable to read and speak English and/or cognitive impairment that would hinder child participation (physician/parent determination).
Study Design and Procedures
This was a multi-site 2-group, randomized controlled trial. Participants completed study measures at 3 time points (baseline T1; post-intervention T2; 30 days post-intervention T3). Following informed consent, participants completed T1 measures. Parent/child dyads were stratified by site and child age (preschool 3-5 years; school-age 6-8 years) and randomized in blocks of 6 to the AME or Audio-Storybooks (ASB) attention control condition. Dyads received 3 sessions over 3 consecutive days, with Session 1 scheduled within 24 hours of admission. All sessions were video recorded to collect child and parent engagement data, and to monitor treatment fidelity. Parents completed T2 measures immediately after Session 3, and T3 measures 30 days post-intervention. Independent use of study activities was collected by parent self-report between sessions and T3.
Study Conditions
Parent/child dyads worked with the same board-certified music therapist (MT-BC) for all sessions. Our team included 17 MT-BCs (10 bachelors-prepared; 7 masters-prepared) all with pediatric oncology experience. Sessions were delivered in a private/semi-private space during an inpatient admission or a series of outpatient clinic appointments over 3 consecutive days. We trained MT-BCs to deliver both intervention and attention control conditions to minimize risk for unmasking evaluators and control for provider differences. All MT-BCs received the same training on standardized protocols and participated in bi-monthly calls. Risk for experimental drift, bias, and diffusion were addressed using self- and external quality assurance monitoring procedures for video recorded sessions.
Active music engagement intervention
Grounded in self-determination and motivational coping theory, 30 the CSM-MT specifies how music can be used to create supportive environments that encourage learning and enactment of active coping strategies to manage distress. 27 Supportive environments offer structure, autonomy support, and relationship support and these principles guided AME design and tailored delivery. First, AME uses age-appropriate, music-based activities to create a structured, predictable environment that supports the actions of children and parents (structure). Second, children choose materials and therapists use live music to support actions initiated by children/parents (autonomy support). Third, music-based play experiences support and sustain reciprocal parent-child interaction (relationship support). AME primary components included therapist-led music-based play activities, a music play resource kit, and session planning and parent tip sheets (Supplemental Table 1). Session duration was 45 minutes and included Introduction/Music Selection (~5 minutes), Music Play (~30 minutes), Tip Sheet Review/Resource Kit (~10 minutes).
Audio-storybooks attention control condition
The ASB condition controlled for attention from a trained clinician, shared parent-child activity, and audio-visual stimulation. Children received an ASB story kit that included 3 illustrated stories with audio narration. During sessions, children selected stories to listen to with their parent. Clinicians also encouraged children/parents to listen to stories between sessions. Session duration was 25 and 30 minutes and mirrored AME session structure: Introduction/Story Selection (~5 minutes), Stories (~20 minutes), and Closing/Resource Kit (~5 minutes).
Measures
Parents completed self-report and parent proxy questionnaires related to antecedent factors (demographics, parent/child distress with prior hospitalization, traumatic distress, and disease/treatment characteristics) known to affect outcomes in young children with cancer and parents 4,17,31 -33; distal mediators (family normalcy, self-efficacy, independent play), child outcomes (primary: emotional distress, secondary: quality of life), parent outcomes (primary: disturbed mood, secondary: TSS, well-being), and family function. Cronbach’s alpha coefficients for T1 multi-item scales ranged from .71 to .95. Supplemental Table 2 summarizes distributional and psychometric properties for measures.
Proximal mediators (child engagement & parent engagement with child) were measured using observational coding. 29 Child Engagement coding included 4 discrete behaviors indicative of active engagement and Parent Engagement with Child coding included 7 discrete behaviors indicative of parent interaction with their child. Independent observers viewed Session 3 videos and coded behaviors using 10-seconds time intervals for observation, followed by 10-seconds to record observed responses. All trained observers reached a minimum criterion of 0.85 for intra- and inter-observer reliability. To ensure consistency, we assessed 27% of videos for inter-rater reliability. If a reliability check fell below .85, we discussed discrepancies, provided retraining, and/or re-coded material. Supplemental Table 3 includes additional coding detail and forms.
Statistical Analyses
Power analysis
Our primary aim was to examine the mediation effects of the AME intervention relative to ASB. To test mediation, we used the percentile bootstrap method to estimate the indirect/mediated effect. 34 Simulations of the 3-path mediation model in Mplus 35 showed that 120 subjects were needed to have 85% power to test the total indirect effect using the Sobel approach when the effect of the independent variable (AME) on the proximal mediator, proximal mediator on distal mediator, distal mediator on outcome, and independent variable on outcome are all at least medium (13% of variation explained). If we allowed the effect of the distal mediator on the outcome and independent variable on outcome to be half-way between small and medium (7% of variation explained) then 156 subjects provided 81% power. Thus, we chose a target sample size of 156 (78 child/parent dyads per group). Using the percentile bootstrap method instead of Sobel should have afforded the same or greater power.
Preliminary analyses
Multicollinearity between the mediator scales was assessed by examining Pearson and Spearman correlations. All correlations were <.40, so all mediators were included together in the mediation models. We also compared the AME group to the attention control group with respect to demographic and baseline outcome variables using 2-sample t tests, chi-square tests, or Fisher’s Exact tests as appropriate. We controlled for age (categorical) and site in all models due to the stratified randomized design and for baseline outcome measures due to the ANCOVA analysis framework.
Main analyses
Per our a priori protocol specifications, we analyzed as randomized and attempted to collect outcome data on non-completers, following the intent-to-treat principle. For testing mediation, each of the 6 outcomes was modeled separately and T2 was modeled separately from T3. Mediation effects were estimated in an ANCOVA setting, fitting the appropriate mediation models using MPlus (version 8.5) 36 and then testing indirect effects (product method) using the percentile bootstrap approach to estimate the indirect effect. 43 The multiple mediation model with 3-path mediation effects specifies that the intervention will act through the proximal and distal mediator on the outcome and also have a direct effect on the outcome (Figure 1). Each outcome model had 6 key predictors (intervention, 2 proximal mediators, 3 distal mediators). Standardized direct, indirect, and total effects were estimated as were R 2 values for each mediator and outcome in the model.
For testing moderation, 2 outcomes (parent traumatic stress-IES-R and parent emotional distress-POMS) were examined with 4 potential moderators at each time point (child distress with prior hospitalizations, parent distress with prior hospitalizations, parent traumatic stress, and child age). We tested moderation effects by including the appropriate main effects and interaction terms with the intervention indicator (AME vs ASB) using linear regression in R (version 4.1.1). 37 Moderation effects were obtained in an ANCOVA setting testing each T2 and T3 outcome separately, adjusting for site and baseline version of the outcome. The moderators were treated as continuous variables, but, for ease of illustration, we estimated the intervention effects at the 25th, 50th, and 75th percentiles. Mean differences between AME and ASB were calculated at each of the percentiles of the moderator. Standardized mean differences were also obtained by dividing the mean difference by the model residual standard deviation.
Missing data and multiple comparisons
A priori, we planned to compare all baseline variables between subjects who dropped out of the study and those who did not but since the attrition rate was so low (12 of 136) we chose not to do this. We applied the Hochberg step-up procedure for the 4 secondary outcomes in the mediation analyses. For moderation analyses, we used alpha = .025 since there were 2 outcomes examined.
Results
Participants
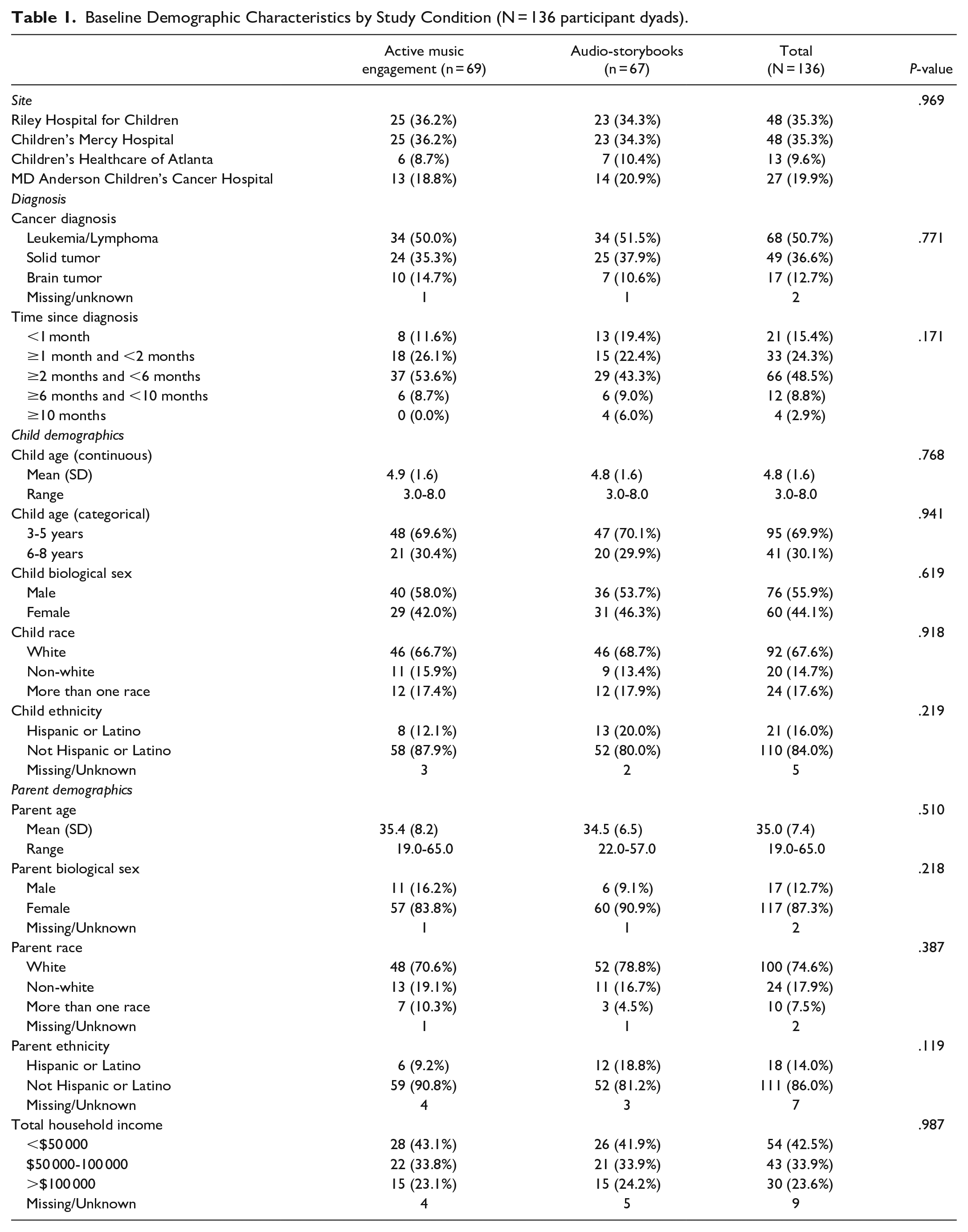
Figure 2 summarizes study accrual, intervention delivery, and data collection. Parent and child demographics (Table 1) and baseline outcome characteristics (Supplemental Table 4) are reported overall and by group. We had a final sample of n = 125. Mean child age was 4.8 years (SD 1.6; range 3-8 years), with the majority (69.9%) falling within the categorical age range of 3 to 5 years. Mean parent age was 35 years (SD 7.4; range 19-65 years). In addition, 33% of children and 25% of parents identified as non-white or more than one race, and 16% of children and 14% of parents identified as Hispanic or Latino. There were no statistical or clinical differences in baseline demographic characteristics between the 2 groups.

CONSORT diagram.
Baseline Demographic Characteristics by Study Condition (N = 136 participant dyads).
Intervention Delivery
The majority (89%) of both AME and ASB dyads completed all 3 sessions (3 dyads completed 2; 2 dyads completed one). Reasons for non-completion included unexpected discharge, parent unavailable, parent declined session, and appointment time change. A majority (97%) of sessions were delivered by the assigned MT-BC (in cases of illness a new therapist was introduced).
Mediation Effects
There were no direct effects of AME on child and parent outcomes; however, the absence of an overall intervention effect does not preclude examination of mediation. As discussed by O’Rourke and MacKinnon, regardless of an intervention effect, mediation analyses should be done to examine conceptual models by investigating the relationship between the intervention with potential mediators and potential mediators with outcomes. 38 As such, we proceeded with our planned analysis examining the relationship between the AME intervention with potential mediators and potential mediators with outcomes.
There was an indirect effect of AME on parent well-being (Index of Well-being Total Score) through parent engagement with their child at T2 (unadjusted P-value = .03) indicating that AME led to greater parent engagement with child and greater parent engagement through AME led to improvement in parent well-being (Table 3); however, this effect was no longer significant after multiple comparison adjustment (adjusted P-value = .12).
When examining the mediation effects of potential proximal mediators on distal mediators, we found that child engagement and parent engagement with child did not mediate the effect of AME on changes in perceived family normalcy and parent self-efficacy at T2, and independent use of play materials between therapist-led sessions. Standardized effects and 95% confidence intervals from the mediation models are reported in Table 2. In total (ie, combining direct and indirect effects) independent use of play materials between therapist-led sessions was greater for dyads in AME versus ASB.
Standardized Direct, Indirect and Total Effects for Proximal Mediators on Distal Mediators (N = 125 Patients, 95% Bootstrap Confidence Intervals, 5000 Replications).

Abbreviations: GRP, AME versus Audio-Storybooks; CE, child engagement (total active engagement score); PEC, parent engagement w/child (total score); PFC, perceived family normalcy (change in family life difficulty from baseline); PSE, parent self-efficacy (change in parent beliefs total score from baseline); IUP, independent use of play materials (total time between therapist-led sessions, reported at sessions 2 and 3); OUT, change in PFC and PSE at T2 or IUP.
All models were adjusted for site, age and baseline value of the distal mediator (if applicable).
Since the confidence interval did not contain 0, this effect (P-value < .001) is significant at the alpha = .05 level.
When examining mediation effects of potential distal mediators on child and parent outcomes, we found that change in perceived family normalcy, parent self-efficacy, and independent use of play materials did not mediate the effect of AME on child outcomes (emotional distress, quality of life), parent outcomes (emotional distress, TSS, well-being), or family function at T2 (Table 3) or T3 (Supplemental Table 5). Note that the low R 2 values for the distal mediators (ranging from 0.7% to 12%) in Tables 2 and 3, and Supplemental 5 show lower than medium relationships (<13%) between the group variable and proximal mediators with the distal mediators.
Standardized Direct, Indirect and Total Effects From 3-Path Mediation Model for T2 Outcomes (N = 125 Patients, 95% Bootstrap Confidence Intervals, 5000 Replications).

Abbreviations: GRP, AME versus Audio-Storybooks; CE, child engagement (total active engagement score); PEC, parent engagement w/ child (total score); PFC, perceived family normalcy (change in family life difficulty from baseline); PSE, parent self-efficacy (change in parent beliefs total score from baseline); IUP, independent use of play materials (total time between therapist-led sessions, reported at sessions 2 and 3); OUT, outcome; CHQ, Child Emotional Distress–CHQ – Mental Health Subscale; KINDLE, Child Quality of Life–KINDL Total Score Transformed; POMS, Parent Emotional Distress POMS-Short Form Total; IES, Parent traumatic Stress Symptoms–Impact of Events Scale-Revised (IES-R) Total; IWB, Parent Well-being–Index of Well-being Total; FACES, Family Function (FACES II)–Total Score.
All models were adjusted for site, age, and baseline value of the outcome.
Since the confidence interval did not contain 0, this effect is significant at the alpha = .05 level. However, the Hochberg-adjusted P-values were .08 and .12 for the total indirect and PEC indirect effect, respectively.
Moderation Effects
Parent and child distress with prior hospitalizations
Parent distress with prior hospitalizations did not moderate the effects of AME. Child distress with prior hospitalizations did not moderate the effect of AME versus ASB for parent IES-R total scores. However, we did find moderation of effect for intrusion subscale scores at T2 (P = .01) and avoidance subscale scores at T3 (P = .007).
Specifically, at T2 in the AME group there was no association between child distress with prior hospitalizations and parent intrusion symptoms (slope = 0.00, P = .79) but in the ASB group, greater child distress with hospitalization was associated with greater parent intrusion (slope = 0.04, P = .005). As shown in Figure 3, the intervention effect was significant at the 75th percentile (MD = −0.36, SMD = −0.66, P = .007). Standardized mean differences at 25th and 50th percentiles were .07 and −.29, respectively.

Moderation effect of child distress with prior hospitalizations on AME for parent intrusions symptoms at Time 2.
At T3 in the AME group there was no association between child distress with prior hospitalizations and parent avoidance symptoms (slope = 0.00, P = .98) but in the ASB group, greater child distress with hospitalization was associated with greater parent avoidance (slope = 0.05, P = .001, Supplemental Figure 1). Standardized mean differences at 25th, 50th, and 75th percentiles were 0.44, 0.03, and −0.38, respectively. As with parent intrusion symptoms, there was no relationship between prior child distress and avoidance symptoms in the AME group, but a positive relationship in the ASB; however, the effect was not significant at any of the 3 percentiles.
Parent traumatic stress screener
Parent scores on the traumatic stress screener (PCL-6) moderated the effect of AME versus ASB for parent hyperarousal subscale scores at T2 (P = .01); specifically, at T2 in the AME group there was no association between PCL-6 scores and parent hyperarousal symptoms (slope = 0.00, P = .85) but in the ASB group, greater PCL-6 scores were associated with greater parent hyperarousal (slope = 0.05, P = .003, Supplemental Figure 2). Standardized mean differences at 25th, 50th, and 75th percentiles were 0.27, 0.01, and −0.33, respectively. As with the child distress moderator, there appeared to be no relationship between PCL-6 scores and parent hyperarousal symptoms in the AME group, but a positive relationship in the ASB group, although the effect was not significant at any of the 3 percentiles.
Child age
Child age did not moderate the effect of AME versus ASB for primary or secondary outcomes.
Discussion
This study elucidates mechanisms of an active music engagement intervention on clinical outcomes in young children with cancer and parents. Specifically, we found evidence for a potential indirect effect of AME on parent well-being that was mediated through increased parent engagement with their child. In addition, our moderation analyses indicate a buffering effect of AME on parent TSS for 2 sub-groups of parents. Together these findings bring us closer to understanding how AME works and how to identify young children/parents who may derive the most benefit. Here we discuss main findings and implications for future trials and clinical practice.
We did not detect a mediation effect of the proximal mediators through the distal mediators. As demonstrated in the R 2 values, this was because the proximal mediators, combined with the group variable, explained very little of the variation in the distal mediators. Our mediational analysis did suggest that parent engagement with their child during AME explained changes in parent well-being post-intervention. Although this was not statistically significant after multiple comparison adjustment, qualitative data collected from these participants and reported elsewhere support and provide further insights into attributes of the shared music-play experience that promoted engagement and the relationship of parent engagement to well-being. 39
In brief, parents described how the therapist used music to create a safe and healthy space that helped divert their attention away from cancer, immerse themselves in a normalizing experience, and playfully connect with their child. Parents also described AME as a transformative experience where they witnessed marked changes in their child’s mood, energy, and symptoms, and that this led to experiences of profound relief for the parent. 39 Other qualitative studies have established that during cancer treatment, parents move into a state of vigilance where their focus is on their child’s survival and other aspects of life get put on hold.9,10,29,40 AME provided reprieve from this hypervigilance, lowered emotional distress, and created opportunities to focus on normal, joyful aspects of the parent-child relationship. These findings suggest that parent observed changes in child distress may be an important mediator of change in parent well-being that we need to examine in subsequent trials.
Our moderation analysis showed a buffering effect of AME on TSS for a subset of parents. Recent evidence has identified negative parent perceptions of child health status and health-related quality of life (HR-QOL) are powerful predictors of TSS in parents4,16,31 -33,41 -43—a relationship that was evident in our moderation analyses. Specifically, parent perceptions of child distress during prior hospitalizations moderated the effect of AME for parent IES-R subscale scores including intrusive thoughts immediately post-intervention and avoidance 30 days post-intervention (Figure 3). As shown in Figure 3, AME had a stabilizing effect on intrusive thoughts especially for parents in the 75th percentile who reported higher child distress with prior hospitalizations. Similarly in Supplemental Figure 2, the association between parent reported child distress and parent avoidance symptoms are present for control group parents, but not for AME parents.
Interestingly, qualitative data collected in this trial also revealed that as parents engaged in AME with their child, they experienced a cognitive shift. 39 Watching their child become active and playful helped them focus on well aspects of their child, rather than symptoms and illness. Ultimately, this shift in perspective helped parents view cancer as something that was “part” of their life, rather than all-consuming. These findings contextualize the buffering effect of AME on TSS for this subset of parents, suggesting that AME is shifting parent perceptions—a factor that has been identified as a strong predictor for parent TSS.4,16,31 -33,41 -43
We also found that parent scores on the traumatic stress screener (PCL-6) moderated the effect of AME versus control for hyperarousal post-intervention. Like our other moderation analyses, there was a pattern of no relationship between parents PCL-6 scores and hyperarousal in AME parents and a positive association for control group parents. Although the effect was not significant at any of the 3 percentiles, the effect size was greatest for parents in the 75th percentile suggesting AME had a stabilizing effect on hyperarousal for parents who reported higher traumatic stress symptoms at baseline. This is consistent with studies that have identified early symptoms of acute distress as predicting TSS in later phases of treatment17,31,33,42 and has important implications for the use of AME to prevent TSS symptoms early in treatment.
A strength of our trial was inclusion of families during the early phase of treatment when child distress and parent TSS are at their highest levels. 4 Most of our families (88%) were less than 6 months post-diagnosis, with more than one-third within the first month of diagnosis. High recruitment (87%) and retention (91%) rates speak to the acceptability of the AME and play based dyadic interventions during the early phase of cancer treatment. Also, important to note is that scores for attention control participants (Figure 3; Supplemental Figures 1 and 2) were consistent with prior studies examining the relationship between child distress and parent TSS during cancer treatment, 4 indicating the ASB condition functioned as an accurate comparator for our analyses.
Absence of an overall intervention effect may explain why we did not detect mediation; however, consistent with recommendations from O’Rourke and MacKinnon we still obtained valuable information from the mediation analysis. 38 Specifically, we noted that that the intervention and proximal mediators (ie, child and parent engagement) were not associated with changes in our distal mediators. This finding supports removal of the distal mediators (ie, perceived family normalcy; parent self-efficacy; independent use of play materials) from our conceptual framework and retention of engagement as an important mediator for parent outcomes. This finding also supports reduced emphasis on intervention content related to our distal mediators such as our parent tip sheets.
Clinical Implications
The AME intervention was designed to address the interrelated distress experienced by young children with cancer and their parents during the early phase of cancer treatment. The Integrative Trajectory Model of Pediatric Medical Traumatic Stress (PMTS), and related studies, have emphasized the role that subjective appraisal plays in the development of TSS and PTSD at the time of diagnosis and during acute medical care.4,31 -33 Consistent with the PMTS model, our data suggest the AME was successful in “changing the subjective experience” of cancer treatment and buffered TSS for parents reporting higher distress early in their child’s treatment. As such, we recommend regular screening for TSS in parents and high distress in children to identify families who may benefit most from AME during cancer treatment.
In summary, AME is a promising intervention to mitigate TSS and support well-being in parents of children with cancer. It is particularly useful for parents who screen high for TSS and whose children are highly distressed with hospitalization. We recommend pediatric oncology centers consider increased access to music therapy services, including AME, for this high-risk oncology population.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231218266 – Supplemental material for Mediators and Moderators of Active Music Engagement to Reduce Traumatic Stress Symptoms and Improve Well-being in Parents of Young Children With Cancer
Supplemental material, sj-docx-1-ict-10.1177_15347354231218266 for Mediators and Moderators of Active Music Engagement to Reduce Traumatic Stress Symptoms and Improve Well-being in Parents of Young Children With Cancer by Sheri L. Robb, Kristin Stegenga, Susan M. Perkins, Timothy E. Stump, Karen M. Moody, Amanda K. Henley, Jessica MacLean, Seethal A. Jacob, David Delgado and Paul R. Haut in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by NIH/NINR R01NR1578 (Robb, PI).
ClinicalTrials.gov Identifier: NCT03085927
Indiana University Institutional Review Board: Study # 1511888386
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.