
Abstract
Purpose:
About 1 in 3 people experience persistent fatigue after cancer treatment. People with severe fatigue describe a disabling lack of stamina, anxiety, depression and distressing cognitive changes. Cognitive behavior therapy (CBT) is recommended for people with severe fatigue after cancer treatment, however due to limited resources and lack of available clinicians very few people with cancer have access. This study explored feasibility of a virtual stepped-care CBT program.
Methods:
English speaking adults experiencing persistent fatigue who had either completed cancer treatment, or with stable disease on maintenance therapies were recruited. All participants engaged in a 6-week supported self-help program using a CBT workbook targeting fatigue (STEP 1). After the self-help program, participants with severe ongoing fatigue were stepped-up to a telehealth CBT group focused to fatigue led by a Clinical Psychologist (STEP 2). Feasibility and perceived changes were assessed at baseline, 6 and 12 weeks.
Results:
Of 19 participants, 17 completed STEP 1 and 8 completed STEP 2. Remotely delivered CBT was feasible with high retention, adherence, participant feasibility and satisfaction scores. Cost to deliver STEP 1 was AUD $145 and STEP 2, AUD $280 per participant. Overall, fatigue and self-efficacy improved significantly following STEP 1. Participants with higher baseline fatigue achieved limited improvements with self-help alone, requiring guidance to set achievable goals and reframe cognitions. Fatigue, self-efficacy and mood improved with STEP 2.
Conclusions:
Remotely delivered CBT for cancer fatigue was feasible. The effectiveness of stratified rather than stepped CBT approach, based on fatigue severity should be trialed.
Trial Registration:
Australian and New Zealand Clinical Trials Registry (ACTRN # 11 12622000420741).
Introduction
Cancer-related fatigue (CRF) is reported by approximately 50% of people receiving cancer treatment and is a side-effect that can persist long after treatment finishes for up to a third of survivors.1,2,3 CRF is defined as “a distressing, persistent, subjective sense of physical, emotional and/or cognitive tiredness or exhaustion related to cancer and/or cancer treatment that is not proportional to recent activity, and significantly interferes with usual functioning.” 4 Many people report that CRF limits their capacity to engage in usual activities such as work, exercise and social activities. Cancer-related fatigue is associated with pain, depression and distress. 5
Over the past 2 decades psychological interventions, specifically those using Cognitive Behavior Therapy (CBT), have been endorsed as first line treatment for persistent fatigue in people with cancer. 4 A 2019 systematic review reported that 5 randomized controlled trials of CBT with primary outcome of fatigue all described significant decline over time in fatigue for survivors in the CBT arm, compared to usual care. Improvements in sleep, quality of life, and mood were also observed. 6
Despite the evidence for CBT as an effective treatment for CRF, very few people have access to CBT treatments. In part, this may be due to the resource intensive, costly nature of these health care interventions, with fatigue also being a barrier to access and participation. 7 Provider barriers include lack of knowledge and assessment pathways for CRF symptoms and treatment, lack of published resources specifically targeting CRF that includes a treatment pathway (rather than education materials alone), difficulty allocating clinical resources (eg, clinician time) to delivering CRF treatment programs and limited availability of clinicians with specialized training to deliver these intensive interventions. 8 Hence, CBT has not been integrated as an essential part of fatigue management in oncology services and clinical services providing CBT to address cancer fatigue are scarce in Australia.
Stepped-care interventions offer a solution to standard CBT approaches, as they cater to people with differing needs using different intensity interventions. Stepped-Care uses low-intensity treatments (eg, self-help workbook) for people with lower acuity and “steps up” to specialist services (eg, face-to-face CBT), dependent on symptom severity and/or response to first line low-intensity treatment. 9 Both self-help and face to face CBT are known to be effective for a range of psychological presentations.10,11 Stepped-care approaches can therefore help more people using the same resources as standard CBT. The feasibility of embedding a stepped care CBT program for fatigue into “real world” clinical settings (outside of the research context), that considers reach and sustainability has not been established in Australian cancer services.
This manuscript reports on the feasibility, acceptability, appropriateness and perceived benefits of a CBT stepped-care program targeting CRF. Specifically, the authors examined the feasibility and potential benefits of a self-help CBT workbook for CRF and secondly the feasibility and potential benefits of a CBT group for those that needed more intensive support than the self-help workbook alone. It was hypothesized that the program would be feasible, acceptable and appropriate for participants and health care provider.
Methods
Study methodology is described in detail elsewhere, 12 and summarized below.
Participants
English speaking adults who had either completed cancer treatment or were on long term maintenance treatment for any cancer with stable disease, and reported moderate to severe fatigue on a series of researcher-administered eligibility screening questions were eligible to participate. Screening included questions related to the study inclusion and exclusion criteria (ie, fatigue rating, treatment status, sleep apnea, suicidal ideation). Participants were excluded if researchers or the participant’s medical team considered that a medical or major psychological condition would interfere with fatigue treatment.
Procedure
Ethics approval for the study was obtained in 2021 from Peter MacCallum Cancer Centre human research ethics committee (HREC # 21/142L) and the trial was registered with the Australian and New Zealand Clinical Trials Registry (ACTRN # 12622000420741).
Clinical staff at Peter MacCallum Cancer Centre, Melbourne, Australia, referred potential participants to the research team from November 2021 to May 2022. A research team member screened eligibility over the telephone. Eligible participants were invited to enroll in the study and provide their informed consent via email. Consenting participants completed an online baseline questionnaire and received the self-help workbook by mail. After completing supported self-management (STEP 1), eligibility for CBT group therapy (STEP 2) was determined using change in fatigue score on the Time 1 (T1) online questionnaires. Participants scoring below 34 (severe) on the FACIT-Fatigue, 13 or whose T1 fatigue score did not increase by at least 10 from baseline, reported as a meaningful change, 14 were invited to participate in STEP 2.
Intervention
STEP 1: Supported self-management
The REFRESH CBT self-help workbook was developed for this study by experienced health professionals and researchers based on existing literature, with review and input by multidisciplinary experts, people affected by cancer, health literacy specialists and graphic designers. The self-help workbook is structured into 5 chapters, outlined in protocol. 12 Participants were encouraged to read and complete the activities of 1 chapter per week, for 5 weeks, and to complete feedback questions about the chapter attempted. A study psychologist contacted participants each week via email or telephone to support participation and troubleshoot problems. In some circumstances, up to 2 weeks extra time to complete chapters was allowed due to illness or life events.
STEP 2: CBT group therapy
STEP 2 participants attended a CBT group facilitated by a Clinical Psychologist. The hour-long group was delivered weekly for 4 weeks via Telehealth. The REFRESH CBT program was manualized for consistency, with each group session focused on 1 of chapters 2 to 5 of the self-help workbook. Content was tailored to the group based on their particular concerns and areas of need. For example, in Session 1 when group members were already competent in diaphragmatic breathing, another activity was introduced and rehearsed, such as mindfulness. Homework tasks were tailored to the individual’s current capabilities (eg, if previously sedentary, planning a 5 minute walk 3 times a week). Participants referred to their self-help workbooks during groups and the Clinical Psychologist shared the workbook on the screen and completed example activities. Though infrequent in occurrence, individual telehealth sessions were offered as a “catch-up” session to those who were unable to attend group sessions.
Evaluation Measures
The primary aim of this study was to evaluate feasibility of this intervention delivery mode. Psychometric features of all measures are described in full elsewhere. 12 Briefly, feasibility was evaluated using three 4-item self-report measures after STEP 1 and STEP 2: the Acceptability of Intervention Measure, Intervention Appropriateness Measure, and the Feasibility of Intervention Measure. 15 In addition, feasibility evaluation included satisfaction with the intervention using the Client Satisfaction Questionnaire 16 ; qualitative workbook chapter feedback, rates of recruitment, retention and adherence; cost (time) and fidelity.
Secondary outcomes included self-report questionnaires for fatigue, quality of life, perceived self-efficacy and perceived changes. These were measured using The Functional Assessment of Chronic Illness Therapy - fatigue subscale (FACIT-F) 13 ; EuroQual 5 Dimension 5 Level Scale 17 ; Perceived Self-Efficacy for Fatigue Self-Management scale 18 and a study-specific questionnaire about perceived changes in personal, social and lifestyle factors that are targeted in the REFRESH program.
Data Analysis
Descriptive statistics were used to summarize demographic, feasibility and measures of fatigue, self-efficacy and quality of life. Repeated measures t-tests were used to assess changes in fatigue, self-efficacy and quality of life from baseline to time 1 (after completing STEP 1 self-help). Effect sizes were calculated as described by Kazis et al. 19 with Cohen’s d references used of 0.2, 0.5, and 0.8 as small, medium and large effect sizes respectively. Qualitative responses of participant’s experiences and feedback on the program were summarized using content and thematic styles of analysis. Where applicable, data is presented by total group in addition to Group A (those who completed STEP 1 self-help workbook only) and Group B (those who completed STEP 1 and STEP 2 CBT group therapy).
Results
Key socio-demographic, clinical and treatment characteristics of participants are shown in Table 1. Participants were evenly distributed in identified gender (52.9% female), the majority were born in Australia (84.2%) with English as first language (88.2%), were married or de facto (73.7%) and had completed a higher education degree (68.4%). The median age was 64.3 years (range = 19.8-79.8). Approximately two-thirds of participants had a hematological cancer diagnosis with median time since diagnosis of 22.6 months (range = 6.6-425.2). Just under half (47.0%) resided in metropolitan Melbourne, with the remaining participants residing in regional or remote areas of Australia. The median distance from treating hospital to participant’s home was 44.4 km, with the greatest distance reported being over 2000 kms.
Participants’ Baseline Socio-Demographic Characteristics.

Abbreviation: Group A, Self-management only; Group B, Self-management + CBT group therapy.
Based on the question “How would you rate your fatigue at its worst on average over the past 3 days from 1 (no fatigue) to 10 (worst fatigue possible)?”
Program Feasibility: Recruitment and Retention
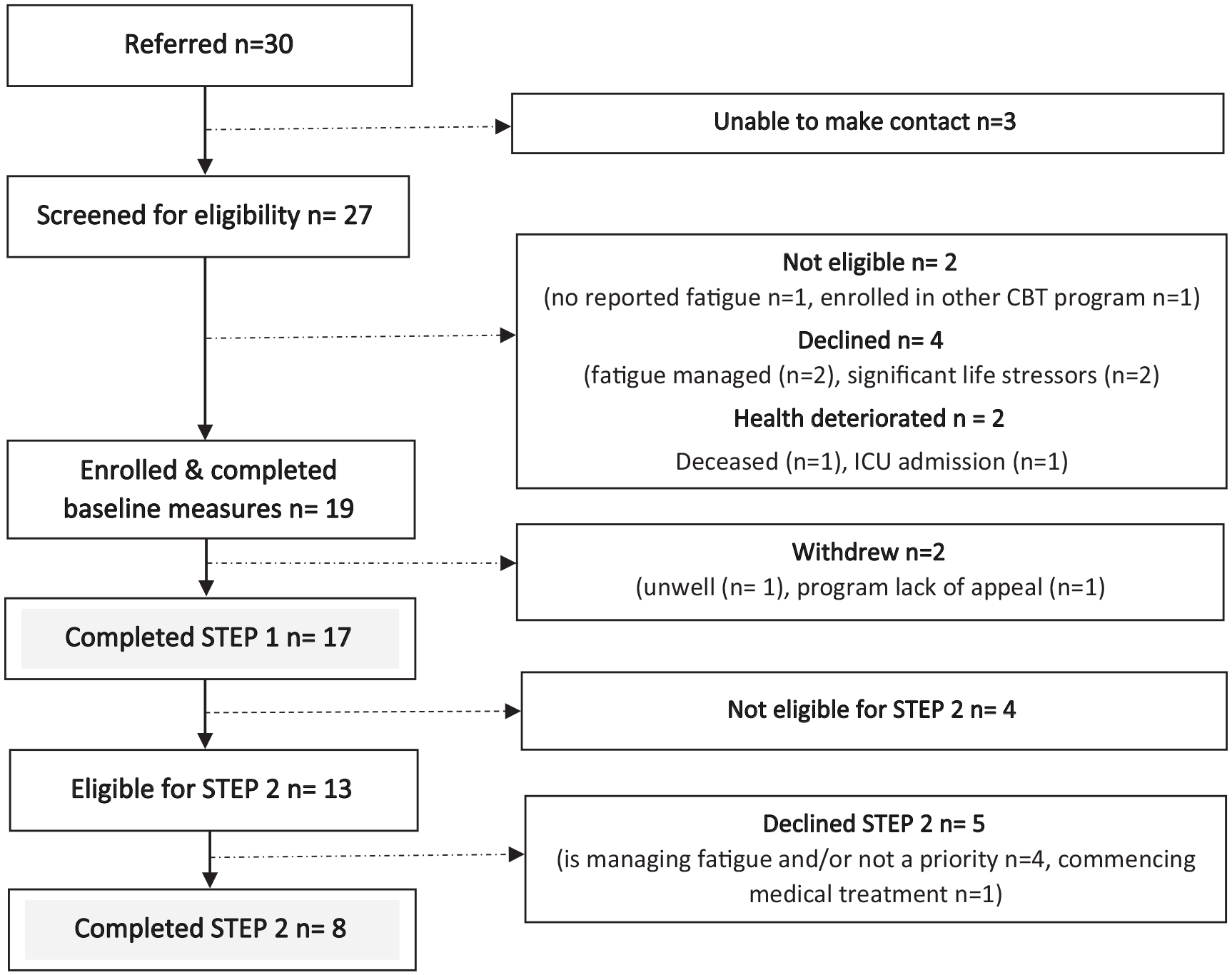
Of 30 people referred to the REFRESH program, 25 were screened as eligible and 19 (63.3%) were enrolled and completed baseline questionnaires. Figure 1 shows recruitment flow and reasons for inability to participate. Seventeen people completed STEP 1 of REFRESH, 13 were eligible for STEP 2 and 8 completed STEP 2. Reasons for declining STEP 2 (n = 5) were self-reported fatigue symptoms were adequately managed and/or lack of time to engage with STEP 2 due to medical or other commitments (eg, work).
Recruitment and participation.
STEP 1 retention rate was 88.2%. Two participants withdrew from the program during STEP 1; 1 was hospitalized and 1 person felt that the program did not meet their needs. STEP 2 retention rate was 100%, and attendance rate was 90.6%. Two participants missed 1 session each due to work commitments and illness respectively. A make-up 1:1 online session was provided to 1 participant with the second participant declining this session due to lack of time.
Program Feasibility: Time and Resources
Table 2 shows details of the time and resources to implement both STEPS of REFRESH. The average cost to deliver STEP 1 was AUD 145 per participant. Costs include program materials, clinical and administrative time. Although these all tasks were conducted in the current study by the project manager/clinical psychologist, the administrative costs were calculated using an allied health assistant hourly pay rate. Group A participants, who did not complete the CBT group therapy, each incurred approximately 20 minutes additional administration time. As shown in Table 2, clinical time required to deliver each STEP 2 group was approximately 8 hours, with an additional 80 minutes per participant needed for clinical administration. Based on 2.6 participants per group, the average cost to deliver STEP 2 was AUD 280 per participant.
Resources to Deliver STEP 1 and STEP 2.

STEP 1 Feasibility, Appropriateness, Acceptability and Satisfaction (Self-Help Program)
Quantitative assessment of STEP 1 feasibility, appropriateness, acceptability and satisfaction is shown in Table 3. Overall, participants perceived the self-help program to be feasible, appropriate and acceptable with high ratings of program satisfaction. No difference in these measures was apparent between Group A—who completed STEP 1 only and Group B—who completed both STEPs 1 & 2.
REFRESH Feasibility, Satisfaction, Acceptability and Appropriateness Scores for STEP 1 and STEP 2 of the Program.
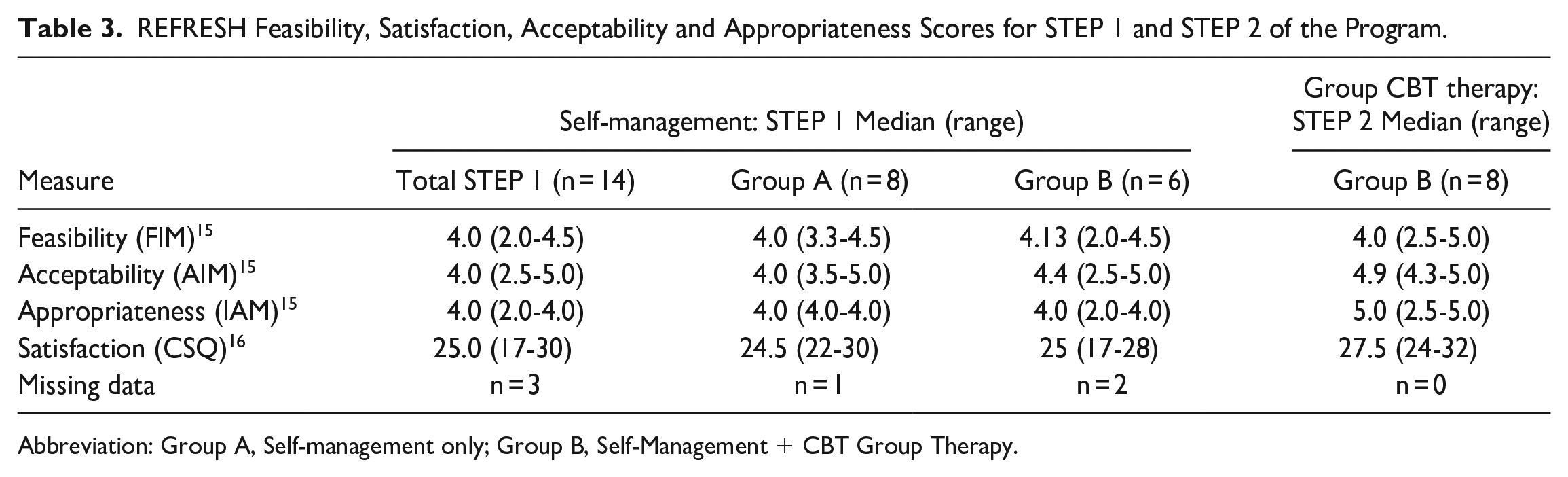
Abbreviation: Group A, Self-management only; Group B, Self-Management + CBT Group Therapy.
STEP 1 Qualitative Feedback—Acceptability and Satisfaction
Overall, feedback for STEP 1 of the REFRESH program was positive with participants expressing satisfaction with the program in addition to feedback that the program was validating and provided helpful strategies to manage fatigue.
I think if this had reached me a little earlier I would not have deteriorated so much.
I am much kinder to myself - more likely to not be angry with myself for being this way. I think now I had suddenly reached the end of my tether so the recognition and hope given by the booklet came at the right time.
The absolute best bit was recognition in myself that the condition I find myself in has a name and some chance of improving- higher level exercise, being outside and treating myself with the same compassion I give to others has improved me and I am less likely to procrastinate and be hard on myself.
Some participants reported that the short timeframe and therefore fast pace needed to complete chapters was challenging, especially when suffering with fatigue, poor motivation and concentration difficulties. A few people found the information too dense and at times demanding to complete. One participant who withdrew from the study, stated that the information was not specific enough for users of different ages, diagnoses and treatment.
My only note is that as someone with fatigue, it was difficult for me to get through it all in the time provided. I really like the content of the booklet, especially chapter five [synthesising coping strategies], and I look forward to working more on the techniques at my own pace.
My motivation and lack of ability to focus on participation in this was the main problem, it was all too much work and reading. I think I would need something more personable. Humans helping humans. . .. . .. . .. . ..not “read a book”
Participants also suggested improvements to the program. Ideas included increasing clinician support/blending support, rather than purely self-help, having a closed weekly online Facebook support group, providing the resources online and offering the program to people during treatment or closer to diagnosis.
Ten participants gave specific feedback on the self-help workbook chapters (Supplemental Appendix 1). Overall feedback of the self-help workbook was positive, with participants noting that the workbook was “well-structured and user friendly” and helped them feel “accepted” and more “confident” in managing symptoms. Everyone who rated the workbook chapters found the activities at least somewhat helpful, with most rating them as “very helpful.”
A wonderful self-help booklet and I intend to use the guide when managing my fatigue and other issues which arise (in) my everyday life.
STEP 2 Feasibility, Appropriateness, Acceptability and Satisfaction (CBT Group Therapy)
Quantitative assessment of STEP 2 feasibility, appropriateness, acceptability and satisfaction is included in Table 3. Overall, participants perceived the CBT group was feasible, appropriate and acceptable with high ratings of program satisfaction. Ratings of group CBT feasibility, appropriateness, acceptability and satisfaction appears to be somewhat higher than that observed for STEP 1 self-help.
STEP 2 Qualitative Feedback—Acceptability and Satisfaction (CBT Group Therapy)
All group CBT participants (Group B) reported that they found the sessions useful. Some suggestions for preferred format included running STEP 1 and STEP 2 concurrently (n = 3), doing STEP 2 only (n = 1), and stepped-care as trialed (n = 2). Others reported the contact with other people in similar situations was beneficial, particularly “hearing other people’s experiences” and the personal interaction. This made them feel “less isolated” and “comfortable opening up.”
I liked the contact with others in much the same situation. I didn’t feel so isolated when listening to others with the same issues.
Another perceived benefit of the group noted by participants was the facilitation of goals, positive reinforcement for weekly achievements, improved motivation and less self-criticism of their ability to manage with fatigue. A couple of people noted that telehealth delivery made the group very accessible.
They were very beneficial for a variety of reasons, the most important in my view is: Identifying goals that will effect change and then breaking those down into achievable tasks. The personal interaction sparked my interest, where the book on its own did not. (ID#)
Roughly half of Group B participants would have liked more group sessions, observing that they were just starting to initiate changes in the 4 weeks. One person thought that a list of personalized recommendations at the conclusion of the group would have been helpful in addition to group support for partners.
I think these sessions need to last a bit longer to change habits, I would propose a minimum of three months. I wish it was longer lasting. All my best wishes for the success of the program in the future, I believe it is worth funding and supporting.
Field Diary Results: Facilitating and Implementing STEP 2 CBT Group therapy
The CBT group facilitator (LW) recorded aspects of group facilitation and delivery that were relevant to feasibility and implementation in a field diary (Supplemental Appendix 2). These included the Psychologist’s observations on group size, frequency, mode, duration and appropriateness.
STEP 1 & 2 Secondary outcomes: Fatigue, Self-Efficacy, Quality of Life and Perceived Changes in Symptoms and Activities
Table 4 shows overall results for self-reported fatigue, self-efficacy and quality of life outcomes at baseline (T0), after STEP 1 (T1) and at 12 weeks (T2). Group A includes participants who did STEP 1 only. Group B participants completed both STEP 1 and 2.
Results - Fatigue, Self-Efficacy, and Quality of Life Raw Scores.

Group A - self-management only; Group B - self-management + CBT group therapy T0 baseline; T1 end STEP 1 self-management; T2 end STEP 2 CBT group therapy (Group B) or 12 wk (Group A).
Fatigue: t(16) = 3.7, P = 0.002.
Self-efficacy: t(16) = 3.8, P = 0.001.
Quality of life: t(16) = −1.5, P = 0.14.
Repeated measures t-test comparing T0 to T1 (all participants).
Fatigue
Of the 17 participants who completed STEP 1, 14 had a positive change score of 3 to 17 points on the FACIT-F. This represents a significant overall improvement in fatigue following STEP 1 [t(16) = 3.7, P < .002, 95% CI (2.7, 9.7)], with a medium effect size 20 (d = 0.63). Despite the overall improvement after STEP 1, 13 participants were eligible for STEP 2. The remaining 4 participants did not meet STEP 2 criteria. Ten eligible participants (58.8%) remained categorized as severely fatigued following STEP 1 (FACIT-F score <34) and 3 participants had fatigue scores ≥34 but had changed by less than 10 points.
Time-2. For both Group A and Group B, there was a trend for continued improved fatigue at 12 weeks.
Self-efficacy for managing fatigue
There was a significant improvement in self-efficacy in managing fatigue following completion of STEP 1 [t(16) = 3.8), P < .001, 95% CI (0.7, 2.3)] with medium effect size 20 (d = 0.7). At baseline, median self-efficacy for managing fatigue was higher for Group A than Group B participants. At the end of STEP 1, both groups achieved a median increase in self-efficacy.
Time-2. Group A participants had the same median self-efficacy score at Time-1 and Time-2 indicating no further improvements after completion of the self-help workbook. Group B participants’ median self-efficacy score increased after each STEP, indicating improved confidence in managing fatigue after each intervention.
Quality of life
Quality of life scores improved following STEP 1 however, this result did not reach statistical significance (t(16) = −1.5, P = 0.14). Lower median quality of life scores indicated higher quality of life for Group A at baseline compared to Group B and remained unchanged after STEP 1 and STEP 2. Group B median quality of life score improved from 7.5 to 5.5 from baseline to completion of STEP 1 however, drifted out to 6.5 at the end of STEP 2.
Perceived changes in symptoms and activity
After STEP 1 almost half the participants perceived improvements in mood, exercise levels, social activities, hobbies and/or concentration/motivation, particularly those in group A (self-help only). Figure 2a and b shows perceived changes for groups A and B at Time-1 and Time-2.

Perceived improvements in symptoms and activities following participation in REFRESH: Group A. (a) Perceived improvements in symptoms and activities following participation in REFRESH: Group A at T1 and T2 and (b) Perceived improvements in symptoms and activities following participation in REFRESH: Group B at T1 and T2.
Of note is that no participant perceived worsened symptoms at Time-2. Although they did not engage in further REFRESH intervention, 14.3% to 57.4% of Group A participants reported psychosocial factors were further improved at Time-2. For some symptoms, the proportion of people perceiving improvements at Time-2 was greater for those that completed STEP 2. For example, 75% of Group B participants reported that their mood was better (Group A: 28.6%), 87.5% in Group B perceived their stress and anxiety were better (Group A: 57.1%) and 87.5% of Group B stated their exercise levels were better (Group A: 14.3%).
Discussion
This study demonstrated that a low-resource “short-course” CBT program targeting CRF is feasible, and may have benefits for participants with moderate to severe CRF.
The proportion of participants eligible for STEP 2 (76.5%) suggests that a 5-week self-help CBT program was helpful in improving symptoms of fatigue however, insufficient to achieve meaningful reductions in fatigue for the majority of participants, who reported poor concentration and/or motivation issues. However, it is unlikely that long-term or severe fatigue would reduce meaningfully over 5 weeks, therefore additional time for STEP 1 should be planned.
We avoided comparing change scores in groups A and B because of (a) small numbers in each group, (b) a mix of participants both ineligible and eligible for STEP 2 in Group A, and (c) some participants were not severely fatigued at T0 in Group B. However we can see that Group B participants, whose fatigue did not improve substantially with STEP 1, had greater median baseline fatigue, lower quality of life and lower confidence in managing fatigue than Group A. This suggests that people with greater baseline fatigue may be less likely to respond to self-help CBT and need a more tailored approach. This was apparent in the REFRESH group CBT sessions, when severely fatigued individuals commonly identified activity goals that far exceeded their capacity, doomed to fail. They needed expert guidance to set small, achievable activity goals, and encouragement to practise self-compassion. It is plausible that people who have suffered severe fatigue and activity limitations need professional guidance to address thoughts and emotions before or alongside activity based interventions.
While our study demonstrated the stepped-care approach was feasible, the results suggest a stratified approach using an indicator of baseline impairment may be even more resource- and participant-friendly. For example, a baseline FACIT-F cut-point around 30 could be used to identify people who may only need a self-help workbook and those requiring more expert guidance with STEP 2. To align with participants’ request for more time to practise CBT strategies, the REFRESH STEP 2 program could be delivered with alternating weeks of self-directed therapy and small group CBT, at no additional cost.
This study has several strengths and limitations. The REFRESH program was developed with the needs of severely fatigued individuals and cost in mind. Delivered via telehealth, the group program is accessible to people with limited stamina, regardless of location. In contrast, other successful CBT programs have involved attendance at individual and/or lengthy programs,21,22 web-based 23 or hybrid approaches. 24 While self-help and telehealth can address some of the barriers to implementing CBT for fatigue, 4 it does not suit everyone. However, this approach is readily scalable, and should further testing prove it efficacious, many can benefit at low cost. STEP 1 does not require senior clinical expertise and could be managed by a clinic administration team, trainee psychologist or allied health assistant, costing less than a typical session with a private Psychologist. Enrollment processes could be streamlined with online enquiry, self-referral and preliminary screening.
Although this feasibility study was not designed to detect statistically significant changes in fatigue, the small sample size is a study limitation and conclusions regarding efficacy or applicability in a wider oncology population cannot be made. Additionally, eligibility criteria used for STEP 2 created heterogenous groups that could not be reasonably compared.
Based on feasibility findings, further investigation is warranted into the efficacy of short-course CBT to reduce the impact of moderate to severe fatigue, and feasibility for people who are not fluent in English. Although running the CBT group in languages other than English could be challenging in many settings, producing the CBT workbook in other languages may be feasible.
Conclusion
The REFRESH stepped-care program was feasible for participants and providers, with indicators of improvement in self-reported outcomes. Further research is warranted to evaluate a stratified approach with modified delivery of STEP 2, using a well-designed hybrid effectiveness-implementation trial.
Supplemental Material
sj-docx-1-ict-10.1177_15347354231191701 – Supplemental material for Virtual Delivery of Stepped-Care Cognitive Behaviour Therapy for Cancer Related Fatigue: A Feasibility Study
Supplemental material, sj-docx-1-ict-10.1177_15347354231191701 for Virtual Delivery of Stepped-Care Cognitive Behaviour Therapy for Cancer Related Fatigue: A Feasibility Study by Lauren K. Williams, Maria Ftanou and Elizabeth J. Pearson in Integrative Cancer Therapies
Footnotes
Acknowledgements
The authors acknowledge the contribution of staff and consumers who assisted with the development of the REFRESH self-help workbook in addition to the REFRESH steering group committee who assisted with the research protocol design and methods for participant recruitment.
Author Contributions
L.W, M.F and E.P contributed to the design and implementation of the research. L.W analyzed the results with the support of a biostatistician. L.W facilitated the CBT groups. L.W, M.F and E.P contributed to the writing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Australian Philanthropic funding from the following: Isobel Hill Brown Charitable Trust, Ethel Herman Charitable Trust, TR & RB Ditchfield Med Res Endowment Fund, The Aldred Charitable Endowment, The Alan Gordon McMillen Charitable Endowment, John Williams Endowment, and CF - Lily and John Barlow Fund.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.