
Abstract
Objectives:
To evaluate the efficacy of prophylactic traditional Chinese medicine (TCM) on skin toxicities in patients with advanced lung adenocarcinoma treated with first-line epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) in a randomized-controlled trial (RCT).
Materials and methods:
This pilot study was a prospective, single-center, double-blinded RCT. The study enrolled patients with a new diagnosis of locally advanced and metastatic lung adenocarcinoma harboring EGFR mutations who were treated with first-line afatinib from July 1, 2016 to December 31, 2017. Thirty patients who met the inclusion and exclusion criteria were assigned to the TCM and placebo groups with simple randomization. TCM and placebo were initiated at the same time as afatinib and were administered for 3 months. The survival of each subject was followed until 3 years.
Results:
There were 36 patients with newly diagnosed lung adenocarcinoma during the study period. After the exclusion of 6 patients, the remaining 30 patients were assigned to the TCM (n = 14) and placebo (n = 16) groups comprising the intention-to-treat population. The time to first skin toxicity was 22.3 days in the TCM group and 17.6 days in the placebo group (P = .510) in the per-protocol population. The analysis of the present pilot study results determined that the difference in time to first skin toxicity between the 2 groups would reach statistical significance with a sample size of 237 based on a power of 0.8. There were significant differences in certain subscales of quality of life between the TCM and placebo groups; however, there was no significant difference in progression-free survival or overall survival between the 2 groups.
Conclusions:
Integrative TCM may prolong the time to first skin toxicity in patients with advanced lung adenocarcinoma treated with first-line afatinib. Prophylactic TCM could delay skin toxicity of any grade and reduce the incidence of grade 3 skin toxicity. Future large-scale RCTs are warranted to validate these findings.
Trial Registration:
ClinicalTrials.gov, NCT05204758. Registered on 24 Jan 2022.
Keywords
Introduction
Driver mutations in epidermal growth factor receptor (EGFR) and anaplastic lymphoma kinase play an important role in oncogenesis of non-small cell lung cancer (NSCLC).1-3 EGFR-tyrosine kinase inhibitors (TKIs) have become a first-line therapeutic option in patients with advanced NSCLC harboring EGFR mutations due to their success in tumor reduction and improved progression-free survival (PFS) compared with standard chemotherapy.4-9
The first-generation EGFR-TKIs gefitinib or erlotinib are considered to be equivalent in clinical practice. 10 The second-generation EGFR-TKI afatinib, which irreversibly inhibits tyrosine kinase activity, has higher affinity for the EGFR kinase domain compared with gefitinib and erlotinib, which reversibly inhibit tyrosine kinase activity. 11 The LUX-Lung 7 trial demonstrated that afatinib as first-line treatment significantly improved PFS and overall survival (OS) compared with gefitinib as first-line treatment in patients with advanced lung adenocarcinoma harboring EGFR mutations.12,13 However, patients with advanced NSCLC harboring EGFR mutations receiving the first- and second-generation EGFR-TKIs acquire resistance after 9 to 14 months. The most common mechanism of acquired resistance to the first- and second-generation EGFR-TKIs is the acquisition of the T790M mutation of EGFR, which is detected in up to 50% of patients treated with gefitinib, erlotinib, or afatinib.14,15 The third-generation EGFR-TKI osimertinib, an irreversible T790M mutant-specific EGFR-TKI, was developed to overcome the acquired resistance to the first- and second-generation EGFR-TKIs.16-19
The EGFR-TKIs gefitinib, erlotinib, afatinib, and osimertinib were approved in May 2003, November 2004, July 2013, and November 2015, respectively, by the U.S. Food and Drug Administration. Under Taiwan National Health Insurance payment regulations, patients with locally advanced lung adenocarcinoma (stage IIIB) and those with stage IV metastatic lung adenocarcinoma harboring EGFR mutations are covered for treatment with first-line EGFR-TKIs, including gefitinib and erlotinib since 2006, afatinib since May 2014, and osimertinib since April 2020.
The most common adverse events (AEs) in patients with advanced NSCLC harboring EGFR mutations receiving EGFR-TKIs are skin and gastrointestinal toxicities, and a small proportion of patients with NSCLC treated with EGFR-TKIs require treatment discontinuation due to severe AEs.19-21 Importantly, disease flare after the discontinuation of EGFR-TKIs has been reported to predict poor survival in Chinese patients with NSCLC. 22
The pooled analysis of severe AEs associated with first- and second-generation EGFR-TKIs revealed that rash and diarrhea of grade ≥3 were significantly more frequent with afatinib than with erlotinib or gefitinib. 22 The overall withdrawal rate of EGFR-TKIs was higher with afatinib or gefitinib than with erlotinib. The most common AEs necessitating withdrawal were skin toxicity, interstitial lung disease, and hepatotoxicity. 23 The most common EGFR-TKI-related skin AEs are rash, paronychia, xerosis, and pruritus. 24 The time between TKI initiation and skin rash appearance was 7 (95% confidence interval, 5-12) days for afatinib, which was shorter than that for erlotinib and gefitinib. Several basic strategies have been proposed to manage skin AEs of EGFR-TKIs, which have the potential to improve quality of life (QOL) and prevent dose reduction or treatment discontinuation. 20
The Pan Canadian rash trial, a prospective, multicenter, randomized phase III trial, evaluated the impact of a prophylactic skin treatment regimen on erlotinib-induced skin toxicities in patients with metastatic NSCLC. The study had 3 treatment arms: prophylactic minocycline, treatment at rash initiation, and treatment at the time of grade 3 rash only. 23 Prophylactic minocycline treatment significantly prolonged the time to the development of rash with the most severe grade. The OS was not significantly different among treatment arms, but the OS was longer in patients receiving prophylactic and reactive treatments (7.6 and 8 months, respectively) than in those who did not receive rash treatment unless grade 3 (6 months). 25 Prophylaxis for EGFR-TKI-related AEs are not widely utilized. The Pan Canadian rash trial was an open-label trial, and the patients were not blinded. Moreover, the trial focused on erlotinib-induced skin AEs and erlotinib was used as second- or third-line after platinum doublet therapy. 25
Traditional Chinese medicine (TCM) is one of the most common complementary and alternative medicine therapies for patients with lung cancer. A retrospective case-control study reported that PFS and median survival were significantly longer and that the incidence of skin rash was significantly lower in patients with advanced NSCLC treated with gefitinib plus TCM than in those treated with gefitinib alone. The study prescribed FZKA (Fuzheng Kang-Ai) decoction as the main TCM formula; however, there were further adjustments based on specific symptoms of patients. 26
According to a systematic review and meta-analysis of patients with advanced NSCLC, objective response rate (ORR), disease control rate, and 1- and 2-year survival rates were statistically significant higher in patients treated with EGFR-TKIs plus TCM than in those treated with EGFR-TKIs. Furthermore, the rates of severe rash as well as those of nausea, vomiting, and diarrhea were significantly lower. However, the review included 13 high-quality and 6 low-quality studies and the authors concluded that additional high-quality randomized-controlled trials (RCTs) were necessary to verify the findings. 27
Although several studies indicated that TCM facilitated the treatment of lung cancer, no clinical study to date has analyzed the effect of prophylactic TCM in EGFR-TKI-related skin AEs. Based on TCM syndrome differentiation and treatment, we found that some TCM compositions might be effective in addressing these toxicities.
Therefore, we conducted a prospective, single-center, double-blinded RCT as a pilot study to determine the impact of TCM on EGFR-TKI-related skin AEs. The purpose of the trial was to investigate the synergistic effect of TCM with EGFR-TKIs and to assess whether TCM reduced or prevented EGFR-TKI-related skin AEs without interfering with formulary cancer therapy.
Patients and Methods
Patient Selection
The inclusion criteria were as follows: (1) patients with histologically confirmed diagnosis of locally advanced or metastatic lung adenocarcinoma with EGFR mutations, (2) patients with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) score of 0 to 2, (3) patients receiving afatinib as first-line treatment to ensure a shorter time to observe skin AEs of any grade, and (4) patients with measurable disease evaluated by the Response Evaluation Criteria in Solid Tumors (version 1.1). Additionally, patients with brain metastases were included after adequate treatment.
Study Hypotheses
According to the Pan Canadian rash trial, the mean durations to maximum rash onset were 17.4, 13.3 and 12 days in patients who received prophylactic minocycline, treatment at rash initiation, and treatment at the time of grade 3 rash only, respectively, with an average of 14.2 days. The rates of grade 3 rash were 12%, 8%, and 28% in patients who received prophylactic minocycline, treatment at rash initiation, and treatment at the time of grade 3 rash only, respectively. 25
In the present study, the first hypothesis was that prophylactic TCM with standard of care (SOC) delays skin AEs of any grade beyond 14 days. SOC was defined as appropriate symptomatic treatment for any EGFR-TKI-related AEs. The Pan Canadian rash trial also demonstrated that the rates of grade 3 skin toxicity were 12% and 28% in patients who received prophylactic minocycline and treatment at the time of grade 3 rash only, respectively. 25 Thus, our second hypothesis was that prophylactic TCM with SOC reduces the rate of grade 3 skin toxicity from 30% to <10%.
Study Design and Treatment
This prospective, single-center, double-blinded RCT was a pilot study conducted in China Medical University Hospital in Taiwan, with the aim to compare skin toxicity between first-line afatinib plus TCM and first-line afatinib plus placebo in patients with locally advanced or metastatic lung adenocarcinoma harboring EGFR mutations. The extension to randomized pilot and feasibility trials of CONSORT 2010 statement suggested that the pilot study should explain rationale for numbers in the pilot trial. 28 Accordingly, a total of 30 patients were planned for enrollment with assignment to one of the 2 groups (TCM group receiving SOC with prophylactic TCM and placebo group receiving SOC with placebo) with simple randomization, and the random number table was generated using a computer. Administration of TCM and placebo were initiated at the same time as afatinib and continued for a total of 3 months.
The study nurse generated the random allocation sequence within sealed opaque envelopes, enrolled participants, and assigned participants to interventions. Once a patient consented to enter this trial, a sealed opaque envelope was opened and the patient was then offered the allocated treatment regimen. Neither the patient nor the researcher knew whether the patient belonged to the TCM or placebo group until the data were completely collected, and then the randomization codes were released.
The severity of EGFR-TKI-related skin AEs were categorized into 5 grades according to the Common Terminology Criteria for Adverse Events grading system (version 4.03). 29 All patients were evaluated by 4 attending physicians of thoracic medicine blinded to the group assignment once a week for the first 2 weeks and once every 2 weeks or as needed thereafter. The trial was recommended to end by interim analysis if obvious harmful effects occurred.
All patients provided informed consent prior to study enrollment. The study was approved by the Joint Institutional Review Board of China Medical University Hospital (CMUH105-REC1-055) on May 12, 2016.
TCM and Placebo Preparation
Based on TCM syndrome differentiation and treatment, TCM recipe was chosen from 3 essential TCM formulas, including Bai He Gu Jin Tang (yin nourishing), Wen Dan Tang (phlegm reducing), and Qing Shang Fang Fen Tang (heat clearing). A supplemental file shows the ingredients of the 3 formulas. Placebo without the medical ingredients was prepared to be similar to the weight, color, smell, taste, and packaging of the TCM formulas. The packages contained 1.6 g of TCM or placebo preparations, which were manufactured in powder form by Sun Ten Pharmaceutical (Taichung, Taiwan) according to the good manufacturing practice requirements. In accordance with the standard of Institutional Review Board, any essential TCM formula is permitted in the clinical trial, but more than 2 essential TCM formulas which are mixed as a new drug could not be used in the clinical trial; therefore, patients were instructed to intake 3 packages of TCM or placebo in powder formulation with each meal 3 times a day, for a total of 9 packages per day.
Outcome Measures
Patients were instructed to maintain a diary to record the first presentation date and the day on which maximum EGFR-TKI-related skin AEs occurred. Tumor response to EGFR-TKIs was assessed by chest X-ray once a month and chest computed tomography once every 3 months. QOL evaluation included Dermatology Life Quality Index, Functional Assessment of Cancer Therapy-Lung (FACT-L; version 4), European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Lung Cancer (EORTC QLQ-C30/LC13 version 3.0), and ECOG PS scale. Safety evaluation included complete blood and differential counts, renal and liver function tests, and tumor markers.
All dose reductions, delays, and discontinuations of afatinib as well as changes in the starting dose of afatinib were also recorded. Afatinib at 40 mg/day is recommended as first-line treatment for patients with EGFR-mutant NSCLC. A study reported that reducing the starting afatinib dose to 30 mg/day reduced the incidence and severity of AEs, with no significant difference in PFS between the reduced-dose (30 mg/day) and normal-dose (40 mg/day) afatinib treatments. 30 Therefore, both normal-dose (40 mg/day) and reduced-dose (30 mg/day) afatinib were permitted in the present study.
The primary endpoints were time to skin toxicity of any grade and incidence of grade 3 skin toxicity. The secondary endpoints were OS, PFS, safety, and QOL. The skin toxicities, safety, and QOL of each subject were followed until 3 months. The survival of each subject was followed until 3 years.
Statistical Analysis
The baseline patient characteristics included age, sex, body mass index, EGFR mutation status, smoking, comorbidities, tumor stage, brain metastasis, and metastasis status at the time of screening.
We performed group comparisons between the TCM and placebo groups in the intention-to-treat (ITT), modified ITT, and per-protocol (PP) populations using the Chi-square test for categorical variables and independent sample t-test for continuous variables for baseline patient characteristics and skin toxicities. Safety and QOL were analyzed by paired sample t-test.
The Kaplan–Meier method was used to estimate the cumulative probability of OS and PFS in the TCM and placebo groups, and the log-rank test was used to compare the curves of OS and PFS between the 2 groups.
All analyses were conducted with the SPSS software for Windows (version 25.0, SPSS, Chicago, IL, USA).
Results
Among a total of 36 patients with a new diagnosis of advanced lung adenocarcinoma harboring EGFR mutations from July 1, 2016 to December 31, 2017, 2 patients treated with gefitinib, 1 patient treated with erlotinib, and 3 patients who declined to be included in the trial were excluded. The patient survival was followed up until December 31, 2020. Within the remaining 30 patients, 14 and 16 patients were assigned to the TCM and placebo groups, respectively, in the ITT population using simple randomization. Before the data on time to first skin toxicity were collected, 1 patient with hyperglycemic hyperosmolar state and 1 patient with sepsis in the TCM group and 1 patient with poor compliance and 1 patient with diarrhea in the placebo group withdrew from the study. Therefore, the modified ITT population comprised 12 and 14 patients in the TCM and placebo groups, respectively. During the study duration, 5 patients withdrew due to the following reasons: poor compliance (n = 1), interstitial lung disease (n = 1), stroke (n = 1), progressive disease (n = 1), and pneumonia (n = 1) in the TCM group. Therefore, the per-protocol (PP) population comprised 7 and 14 patients in the TCM and placebo groups, respectively (Figure 1). The baseline patient characteristics did not significantly differ between the TCM and placebo groups in the ITT, modified ITT, and PP populations (Table 1).

CONSORT flow diagram of the patient enrollment process in the TCM and placebo groups in the ITT population, modified ITT population, and PP populations.
Baseline Patient Characteristics in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.

Disease stage was determined according to the seventh edition of the Cancer Staging Manual of the American Joint Committee on Cancer.
Abbreviations: EGFR, epidermal growth factor receptor; ITT, intention-to-treat; NA, not applicable; PP, per protocol; SD, standard deviation; TCM, traditional Chinese Medicine.
Primary Endpoint: Skin AEs
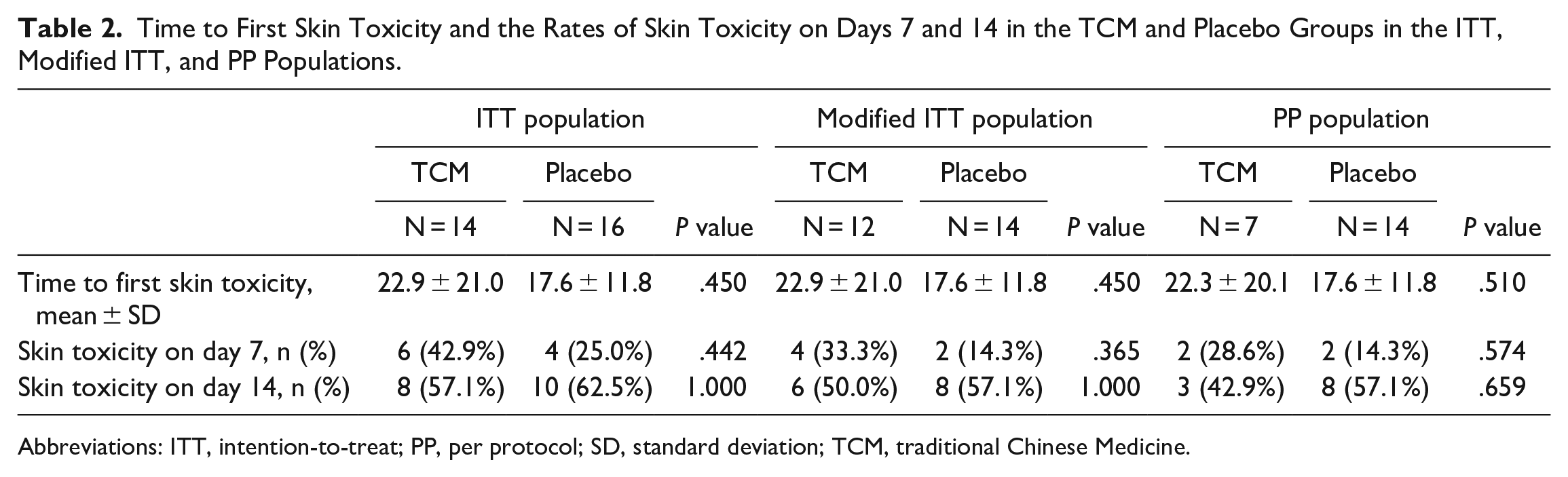
The time to first skin lesion, skin toxicity on day 7, and skin toxicity on day 14 were not significantly different between the TCM and placebo groups in the ITT, modified ITT, and PP populations (Table 2). The date of maximum skin reaction was not analyzed because some patients did not know how to evaluate the severity of skin toxicities and thus the date of maximum skin reaction was not completely recorded.
Time to First Skin Toxicity and the Rates of Skin Toxicity on Days 7 and 14 in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.
Abbreviations: ITT, intention-to-treat; PP, per protocol; SD, standard deviation; TCM, traditional Chinese Medicine.
Albeit not statistically significant, the rate of skin toxicity on day 14 was lower in the TCM group than that in the placebo group in the PP population (42.9% vs 57.1%, P = .659) (Figure 2).

Skin toxicity of any grade on day 14 in the TCM and placebo groups in the PP population.
The time to first skin toxicity was 22.3 days in the TCM group and 17.6 days in the placebo group (P = .510) in the PP population (Figure 3). According to these preliminary results, we determined that the difference in time to first skin toxicity between the 2 groups would reach statistical significance with a sample size of 237 based on a power of 0.8.

Time to first skin toxicity of any grade in the TCM and placebo groups in the PP population.
The cross analysis of skin AEs including paronychia, maculopapular rash, acneiform rash, and Dermatology Life Quality Index from the first visit to the tenth and last visit revealed that there were no significant differences between the TCM and placebo groups in the PP population (Table 3). The incidences of grade 3 skin toxicity in the TCM and placebo groups were <10% in the last visit, and there were no significant differences in the rate of skin AEs of any grade between the TCM and placebo groups in the PP population (Table 4).
Cross Analysis of Skin Adverse Effects in the TCM and Placebo Groups in the PP Population.
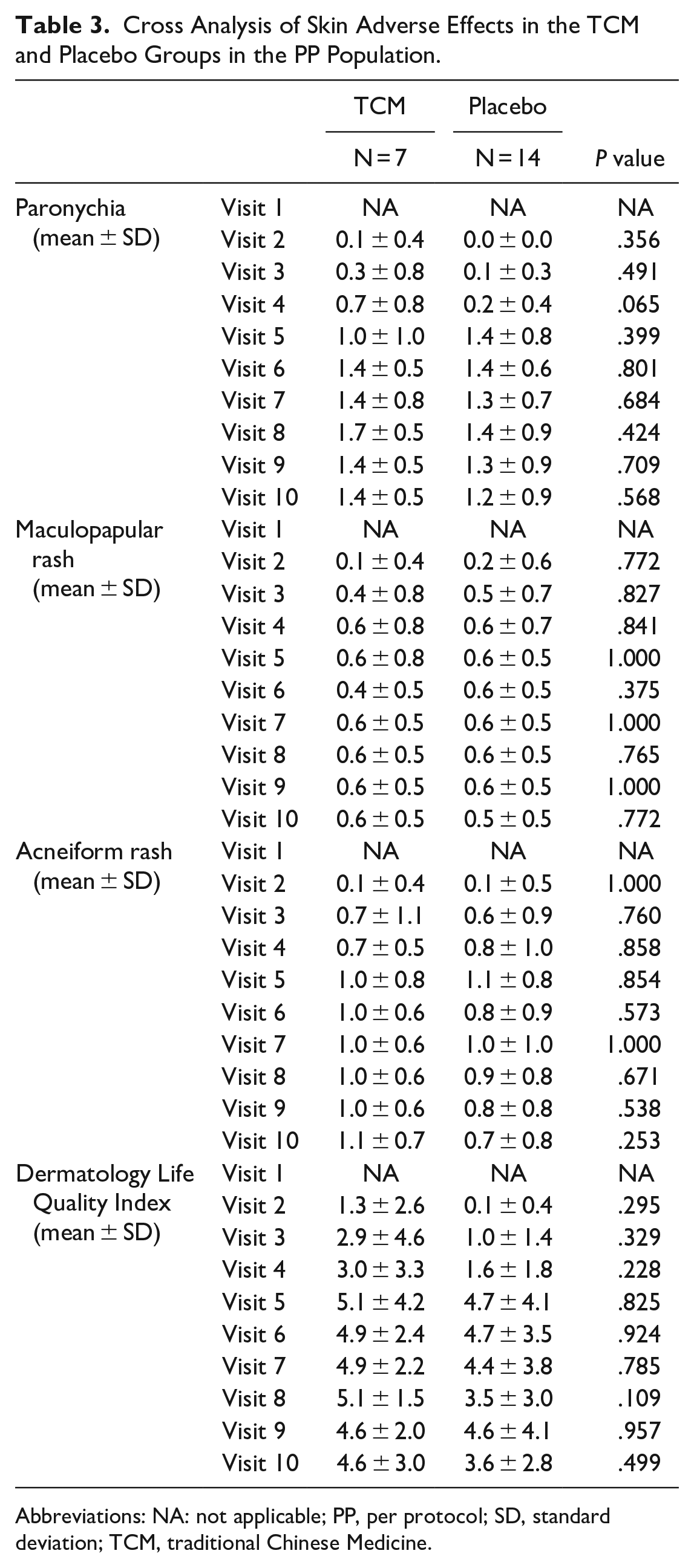
Abbreviations: NA: not applicable; PP, per protocol; SD, standard deviation; TCM, traditional Chinese Medicine.
Cross Analysis of Skin Adverse Effects of Any Grade in the TCM and Placebo Groups in the PP Population.

Abbreviations: NA, not applicable; PP, per protocol; TCM, traditional Chinese Medicine.
Secondary Endpoints: Safety, QOL, and Survival
The analysis of laboratory data revealed that there were no significant differences in any of the parameters except for hemoglobin level between the TCM and placebo groups in the ITT, modified ITT, and PP populations. The mean hemoglobin level was significantly decreased with treatment in the TCM group in the ITT and modified ITT populations (t = −2.969, P = .021 and t = −2.969, P = .021, respectively). Conversely, the mean hemoglobin level was also decreased with treatment in the TCM group in the PP population, albeit without statistical significance (t = −2.427, P = .051) (Table 5).
Changes in Blood Test Results in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.

Abbreviations: ITT, intention-to-treat; PP, per protocol; SD, standard deviation; TCM, traditional Chinese Medicine.
Paired sample t-test.
The ECOG PS scores were not significantly different between the TCM and placebo groups in the ITT, modified ITT, and PP populations (Table 6).
Changes in ECOG PS Scores in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.

Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance score; ITT, intention-to-treat; NA, not applicable; PP, per protocol; SD, standard deviation; TCM, traditional Chinese Medicine.
Paired sample t-test.
FACT-L includes 5 subscales: Physical Well-Being (PWB), Social/Family Well-Being (SWB), Emotional Well-Being (EWB), Functional Well-Being (FWB), and Lung Cancer Subscale (LCS). 31
After proper reverse scoring, PWB, EWB, and LCS got worse with the higher score, but SWB and FWB got better with the higher score. The scores for PWB, EWB, FWB, and LCS did not significantly differ between the TCM and placebo groups in the ITT, modified ITT, and PP populations. The score for SWB increased after treatment in the TCM group, albeit without statistical significance, whereas the score for SWB significantly increased after treatment in the placebo group (t = 2.233, P = .044) (Table 7).
Changes in FACT-L in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.

Abbreviations: EWB, emotional well-being; FACT-L, Functional Assessment of Cancer Therapy-Lung; FWB, functional well-being; ITT, intention-to-treat; LCS, Lung Cancer Subscale; PP, per protocol; PWB, physical well-being; SD, standard deviation; SWB, social/family well-being; TCM, traditional Chinese Medicine.
Paired sample t-test.
EORTC QLQ-C30 consists of 30 questions assessing health-related quality of life which are grouped into 5 functional scales, including physical functioning, role functioning, emotional functioning, cognitive functioning, and social functioning; into 3 symptom scales, including fatigue, nausea and vomiting, and pain; and into 6 single-item scales, including dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties. EORTC QLQ-LC13 consists of 13 questions assessing lung cancer-associated symptoms (cough, hemoptysis, dyspnea, and site-specific pain), treatment related side effects (sore mouth, dysphagia, peripheral neuropathy, and hair loss), and pain medication. 31 After proper reverse scoring, each subscale of EORTC QLQ-C30-LC13 Questionnaire got worse with the higher score. Within the EORTC QLQ-C30 Questionnaire, the scores for social functioning and diarrhea significantly increased after treatment in the TCM group (t = 2.970, P = .025 and t = 2.521, P = .045, respectively) (Table 8). Additionally, within the EORTC QLQ-LC13 Questionnaire, the scores for sore mouth and hair loss significantly increased after treatment in the TCM group (t = 4.500, P = .004 and t = 2.500, P = .047, respectively); these 2 subscales also significantly increased after treatment in the placebo group (t = 4.204, P = .001 and t = 2.463, P= .029, respectively). Although hemoptysis was the only subscale that significantly decreased after treatment in the placebo group (t = −2.280, P = .040), parallel analysis of the same subscale could not be conducted in the TCM group because the standard error of the difference was 0 (Table 8).
Changes in EORTC QLQ-C30 and QLQ-L13 in the TCM and Placebo Groups in the ITT, Modified ITT, and PP Populations.

Abbreviations: EORTC, European Organization for the Research and Treatment of Cancer; ITT, intention-to-treat; NA, not applicable; PP, per protocol; QLQ, Quality of Life Questionnaire; SD, standard deviation; TCM, traditional Chinese Medicine.
Paired sample t-test.
t cannot be computed because the standard error of the difference is 0.
The results of the EORTC QLQ-C30 and QLQ-L13 are the same in the ITT, modified ITT, and PP populations.
In the Kaplan–Meier analysis of OS, the mean follow-up durations were 359.4 and 506.3 days in the TCM and placebo groups, respectively. There were ten deaths during the 5-year period. In the Kaplan–Meier analysis of PFS, the mean follow-up durations were 220.3 and 397.8 days in the TCM and placebo groups, respectively. The OS and PFS were not significantly different between the 2 groups. Finally, the OS and PFS were not significantly different between the 2 groups among the patients harboring the most common EGFR mutations in advanced lung adenocarcinoma, including del19 and L858R mutations (Figure 4). 32

(A–C) Kaplan–Meier curves of OS in patients with advanced lung adenocarcinoma in the ITT population who were treated with first-line afatinib in combination with TCM or placebo during the follow-up period. (A) All patients, (B) those with del19, and (C) those with the L858R mutation. (D–F) Kaplan–Meier curves of PFS in patients with advanced lung adenocarcinoma in the ITT population who were treated with first-line afatinib in combination with TCM or placebo during the follow-up period. (D) All patients, (E) those with del19, and (F) those with the L858R mutation.
Discussion
To date, there have been few clinical studies of the prophylactic efficacy of adjunctive TCM on skin AEs in patients with advanced lung adenocarcinoma treated with first-line EGFR-TKIs. To our knowledge, this is the first prospective, double-blinded RCT to investigate the impact of prophylactic adjunctive TCM therapy on skin AEs in this patient population.
Our analyses suggest that integrative TCM may prolong the time to first skin toxicity. The time to first skin toxicity observed in the TCM group in the PP population, which was 22.3 days, confirmed our first hypothesis that prophylactic TCM with SOC would delay skin toxicity of any grade beyond 14 days. The present study also confirmed our second hypothesis that the incidence of grade 3 skin toxicity in the TCM group would be <10%. The TCM group did not exhibit any additional AEs except for significant decreases in hemoglobin levels in the ITT and modified ITT populations but not in the PP population. Both the TCM and placebo groups exhibited worsening QOL in sore mouth and hair loss subscales. The TCM group also exhibited worsening QOL in diarrhea and social functioning subscales, probably because the TCM recipe used in the study was formulated against skin toxicity and not gastrointestinal or other toxicities.
A clinical study by Tang et al. 33 demonstrated that the PFS was significantly longer in the absence of additional AEs in patients with NSCLC harboring EGFR mutation, including del19 and L858 mutation, who were treated with EGFR-TKIs in combination with TCM compared with patients who were treated with EGFR-TKIs only. These results are inconsistent with the findings of the present study, which might be owing to several reasons. First, the study by Tang et al. was not a double-blinded RCT. Second, the study by Tang et al. was designed to administer 4 different TCM recipes in 4 patient groups, whereas the current study utilized the same fixed TCM recipe comprising 3 TCM formulas in the TCM group. Third, the study by Tang et al. enrolled patients with NSCLC harboring EGFR mutations who were treated with gefitinib or erlotinib whereas the current study included patients with EGFR-positive lung adenocarcinoma who were treated only with afatinib. Fourth, the previous study excluded patients with serious complications whereas the current study accepted patients with an ECOG PS score of 0 to 2. Fifth, the present study did not exclude patients who were lost to follow-up from the final analysis, contrary to that employed in the study by Tang et al. Finally, the TCM recipe was administrated 3 times a day for 2 weeks in the previous study whereas in the current study, the patients were instructed to intake 3 packages of TCM or placebo in powder formulation with each meal, 3 times a day for 3 months. 33
Another multicenter, randomized, double-blinded, placebo-controlled trial reported significantly longer median PFS, improved ORR and QOL, and lower rates of grade 1 to 2 AEs in the EGFR-TKI with TCM group compared with the EGFR-TKI group alone in patients with EGFR mutation-positive advanced pulmonary adenocarcinoma. Nevertheless, that trial also took TCM syndrome differentiation with different TCM recipes in the EGFR-TKI with TCM group. 34
There are several limitations of the present study. First, TCM and placebo were administered only for 90 days, which might account for the lack of significant differences in PFS and OS between the TCM and placebo groups. Future studies should consider longer treatment durations because 1 cohort study reported that TCM use for ≥180 days was associated with a significantly decreased risk of mortality (68%) and disease progression (59%) compared with TCM nonuse in patients with advanced lung adenocarcinoma treated with first-line EGFR-TKIs. In the cohort study, 3 herbs including Fritillaria thunbergii, Oldenlandia diffusa, and Platycodon grandiflorum, and 1 formula, Bai He Gu Jin Tang, could significantly reduce mortality, and this formula was the same as one of the formulas in the current study. 35 Second, the complicated administration scheme for the TCM or placebo powder formulas might be associated with a higher frequency of poor compliance in the present study. Using only 1 TCM formula should be considered. Third, this was a pilot study and our analyses based on the results revealed that a sample size of 237 was necessary to observe a significance effect of TCM on the time to first skin toxicity. Therefore, future studies should consider larger cohorts.
We might be able to delay the time to acquired resistance of afatinib by prolonging the time to first skin toxicity, decreasing the incidence of grade 3 skin toxicity, and preventing the discontinuation of EGFR-TKIs by integrating TCM into treatment regimens. Delaying the time to acquired resistance of afatinib also means delaying the time to acquired resistance of osimertinib and subsequent chemotherapy.17,18,36
In conclusion, the results of the present study suggest that TCM could provide a synergistic effect with EGFR-TKIs, indicating that TCM could prevent and reduce EGFR-TKI-related skin AEs without interfering formulary cancer therapy. In the future, large-scale RCTs are warranted to validate these findings.
Supplemental Material
sj-docx-1-ict-10.1177_15347354221086663 – Supplemental material for Efficacy of Prophylactic Traditional Chinese Medicine on Skin Toxicity of Afatinib in EGFR Mutation-Positive Advanced Lung Adenocarcinoma: A Single-Center, Prospective, Double-Blinded, Randomized-Controlled Pilot Trial
Supplemental material, sj-docx-1-ict-10.1177_15347354221086663 for Efficacy of Prophylactic Traditional Chinese Medicine on Skin Toxicity of Afatinib in EGFR Mutation-Positive Advanced Lung Adenocarcinoma: A Single-Center, Prospective, Double-Blinded, Randomized-Controlled Pilot Trial by Chia-Ling Li, Te-Chun Hsia, Su-Tso Yang, Kun-San Clifford Chao, Chih-Yen Tu, Hung-Jen Chen and Chia-Hsiang Li in Integrative Cancer Therapies
Supplemental Material
sj-docx-2-ict-10.1177_15347354221086663 – Supplemental material for Efficacy of Prophylactic Traditional Chinese Medicine on Skin Toxicity of Afatinib in EGFR Mutation-Positive Advanced Lung Adenocarcinoma: A Single-Center, Prospective, Double-Blinded, Randomized-Controlled Pilot Trial
Supplemental material, sj-docx-2-ict-10.1177_15347354221086663 for Efficacy of Prophylactic Traditional Chinese Medicine on Skin Toxicity of Afatinib in EGFR Mutation-Positive Advanced Lung Adenocarcinoma: A Single-Center, Prospective, Double-Blinded, Randomized-Controlled Pilot Trial by Chia-Ling Li, Te-Chun Hsia, Su-Tso Yang, Kun-San Clifford Chao, Chih-Yen Tu, Hung-Jen Chen and Chia-Hsiang Li in Integrative Cancer Therapies
Footnotes
Acknowledgements
Author Contributions
Chia-Ling Li: conception of study design, statistical analysis, interpretation of the data, literature review, and writing the manuscript. Te-Chun Hsia: conception of study design, subject enrollment, evaluation of the clinical data, interpretation of the data, critical revision, and study supervision. Su-Tso Yang: conception of study design, interpretation of the data, critical revision, and study supervision. K. S. Clifford Chao: conception of study design, interpretation of the data, and critical revision. Chih-Yen Tu: subject enrollment and evaluation of the clinical data. Hung-Jen Chen: subject enrollment and evaluation of the clinical data. Chia-Hsiang Li: conception of study design, subject enrollment, evaluation of the clinical data, interpretation of the data, and critical revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially sustained by Center of Augmented Intelligence in Healthcare, China Medical University Hospital, China Medical University, Taichung, Taiwan and Department of Computer Science and Information Engineering, Asia University, Taichung, Taiwan (Grant No. CMU102-ASIA-19). This research is primarily supported by the Phase 3 Cancer Research of Cancer Center Project and Cancer Research Project of Innovative Medical Technology and Integrated Chinese and Western Medicine, China Medical University Hospital, Taiwan and sponsored by the Health and Welfare Surcharge of Tobacco Products and Cancer Research Center of Excellence, China Medical University Hospital, Taiwan (Grant No. MOHW107-TDU-B-212-114024 and MOHW108-TDU-B-212-124024).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.