
Abstract
Objectives:
Since pre-existing expectations, that is, beliefs, in a treatment may modify outcomes, and acupuncture studies often fail to measure expectations, we wanted to investigate the use of acupuncture, interest, and belief in acupuncture effects among patients undergoing cancer therapy.
Method:
A cross-sectional design, where the participants answered a study-specific questionnaire with questions regarding their use of, interest and belief in acupuncture treatment.
Results:
A total of 457 patients with cancer (48% men, mean age 65 years) answered the questionnaire. Acupuncture was used by 4 (1%) patients during their cancer therapy, and 368 (83%) expressed an interest in receiving acupuncture. Of the 457 patients, 289 (63%) believed acupuncture to be effective for at least 1 of 17 requested symptoms, most commonly pain (56% of the patients) and muscle tension (40%). They believed acupuncture to be effective for a mean value 3 of the 17 requested symptoms. Women (P < .001), and patients 41 to 65 years (P < .001), expressed a stronger belief in acupuncture effects than others.
Conclusions:
Men and older patients expressed weaker beliefs in acupuncture effects than other patients, indicating the importance of collecting expectancy data in future randomized sham-controlled acupuncture studies to be able to treat expectancy as an effect-modifier. The high interest and beliefs in acupuncture effects found also indicate that acupuncture should be available for patients with cancer, for side effects where acupuncture has shown to be effective. In a clinical setting, older men might need more encouragement regarding positive expected outcomes of the acupuncture treatment than younger women.
Keywords
Introduction
Shared decision-making between the healthcare practitioners and the patients is an approach where clinicians and patients share the best available evidence when making treatment decisions, and where patients are supported to consider options, to achieve informed preferences. Shared decision-making has the potential to increase the level of quality of care and thus patients’ quality of life based on studies of healthcare in general. 1 Integrative oncology is a patient-centered, evidence-informed field of cancer care that utilizes mind and body practices, natural products, or lifestyle modifications from different traditions, for example acupuncture, alongside conventional cancer treatments. Integrative oncology aims to optimize health and to empower patients with cancer to share the decision-making regarding their therapies. The concept of evidence-informed captures a broad range of evidence, from case reports to randomized, placebo controlled trials, and reflects patients’ values and beliefs, which are privileged in integrative oncology. 2 Belief that a treatment has a potential to provide positive effects, so called treatment expectations, has been shown to highly affect the outcome of both medical 3 and acupuncture4-6 treatments.
Acupuncture therapy is incorporated within the public health care system in many European countries. 7 With the increasing incidence of cancer and major advances in cancer treatment in recent decades, acupuncture has become a popular complementary treatment in oncology care,8-11 even though few sham-controlled studies have evaluated the effects for the symptoms commonly experienced.8,9,12-16 Approved Western health care offers acupuncture to treat a wide range of symptoms and it, therefore, seems important to investigate patients’ pre-existing beliefs about acupuncture. Acupuncture is defined as “a family of procedures involving stimulation of anatomical locations on the skin by a variety of techniques.” Most commonly, the skin located at each acupuncture point is penetrated by thin, solid, metallic needles, which are manipulated manually or by electrical stimulation. 17 Numerous studies of acupuncture suggest that the effect of acupuncture is primarily based on sensorial stimulation to and the responses of the neuro-endocrine system involving the central and peripheral nervous systems.17,18 In addition to these specific treatment effects, acupuncture also has non-specific components that include the context surrounding the delivery of treatment, which may produce non-specific treatment effects. 5 Expectancy is accepted as one of the key non-specific components. 3 However, acupuncture effect studies often fail to measure treatment expectations,12-16,18 which indicates that more research highlighting differences in treatment expectations and beliefs are needed.
Most patients with cancer experience multiple symptoms related to either the cancer itself or side-effects of the cancer therapies that may be effectively treated using acupuncture,8,18 for example pain, 12 nausea, 13 xerostomia, 14 menopausal symptoms, 15 anxiety, depression, and sleep disturbance.9,16 Patients may use acupuncture8,9,12-16,18 although there are also medications available for these symptoms. In line with integrative oncology, patients should share treatment decisions with the oncology professionals. 2 Some patients prefer non-pharmacological complementary and alternative medicine (CAM) therapies, as they reject medications due to side effects, negative attitudes to medications, or non-satisfactory effects. 19 However, in a study of 755 Swedish patients with cancer, just a third of 198 CAM users discussed CAM with their oncology professionals, mostly since they expected the oncology professionals to have a negative attitude. 20 Accordingly, health care may welcome a study conducted independently from the caregiver, to evaluate use of and interest in acupuncture therapy.
Researchers and clinicians often claim that patients with cancer, compared to general populations, 21 seem extraordinarily interested in complementary and alternative medicine,7,10,11,22 for example acupuncture therapy.10,11 Thus, they may be predisposed to experience positive effects from acupuncture. 23 Previous studies regarding acupuncture usage among patients with cancer show divergent prevalence of patients receiving acupuncture, ranging between 6% and 38% of the studied patients.10,11,20,22,24-28 However, to our knowledge, there are just a few previous studies that in addition to usage also explore beliefs and interest in acupuncture in patients with cancer.6,29 The participants in those studies were selected, and already planned for acupuncture treatment when reporting their beliefs.6,29 A study of 198 patients with cancer who were about to receive acupuncture for nausea found that the patients expressed positive beliefs in acupuncture effects, not only for nausea, but also for other symptoms, for example pain and hot flashes. 29 To our knowledge, there are no previous studies that report beliefs in acupuncture effects among patients with cancer who are not considered or planned for acupuncture treatment.
Since approved Western health care offers symptom-managing acupuncture, 7 and integrative oncology 2 aims to optimize health and to empower patients with cancer to share the decision-making 1 regarding their therapies, it seems important to study utilization of acupuncture in relation to interest and belief in acupuncture among patients undergoing cancer therapy. Since treatment belief may modify treatment outcomes,4-6 and characteristics such as age and education level have been shown to affect treatment beliefs,6,29 it seems important to study pre-existing beliefs about acupuncture in subgroups of patients with cancer. The aim of this study was to investigate the use of acupuncture, interest, and belief in acupuncture effects among patients with varying characteristics undergoing cancer therapy.
Methods and Materials
Design and Setting
In this cross-sectional study, we collected data from a cohort of patients from 4 Swedish oncology departments, located in southern, middle, eastern, and western Sweden. The data was collected between June 2016 and January 2017. The Regional Ethical Committees approved the study (Linköping 2015/101-31).
Inclusion
A number of 668 patients planned for radiotherapy were screened for participation in the study. The patients had varying cancer diagnoses, undergoing curative or palliative radiotherapy with or without concomitant chemotherapy. Radiotherapy nurses consecutively screened all patients scheduled for radiotherapy to determine if they met the study criteria. If they met the study criteria, they were given printed as well as short oral information about the study. Inclusion criteria: cancer regardless of tumor type, at least 18 years of age and physical, mental and linguistic capacity to give their informed consent. Exclusion criteria: patients who received a single radiotherapy session or their very first radiotherapy session on the day for data collection. By excluding the patients who received their first or only treatment on the study day, we accordingly excluded those who received palliative single fraction radiotherapy. In the end, 507 patients were included in the study (Figure 1).

Inclusion of participants.
Assessments
Procedure
The participants answered a study-specific questionnaire, developed and validated for the target population patients with cancer undergoing radiotherapy, according to the previously used 30 clinimetric methodology 31 described by Steineck et al. 32 The validated study-specific questionnaire had been feasibly used in a previous study (n = 198 patients with cancer). 29
The participants were instructed to answer the questionnaire in private, either in writing (“paper and pen”) or at the study’s secure, confidential database platform. The paper questionnaires were returned to the authors in assigned answer boxes, or by postal mail using pre-paid envelopes. In case of lack of returned questionnaires, study coordinators sent out 1 reminder by phone or by personal communication in about 2 weeks.
Questions regarding use of and interest and beliefs in acupuncture
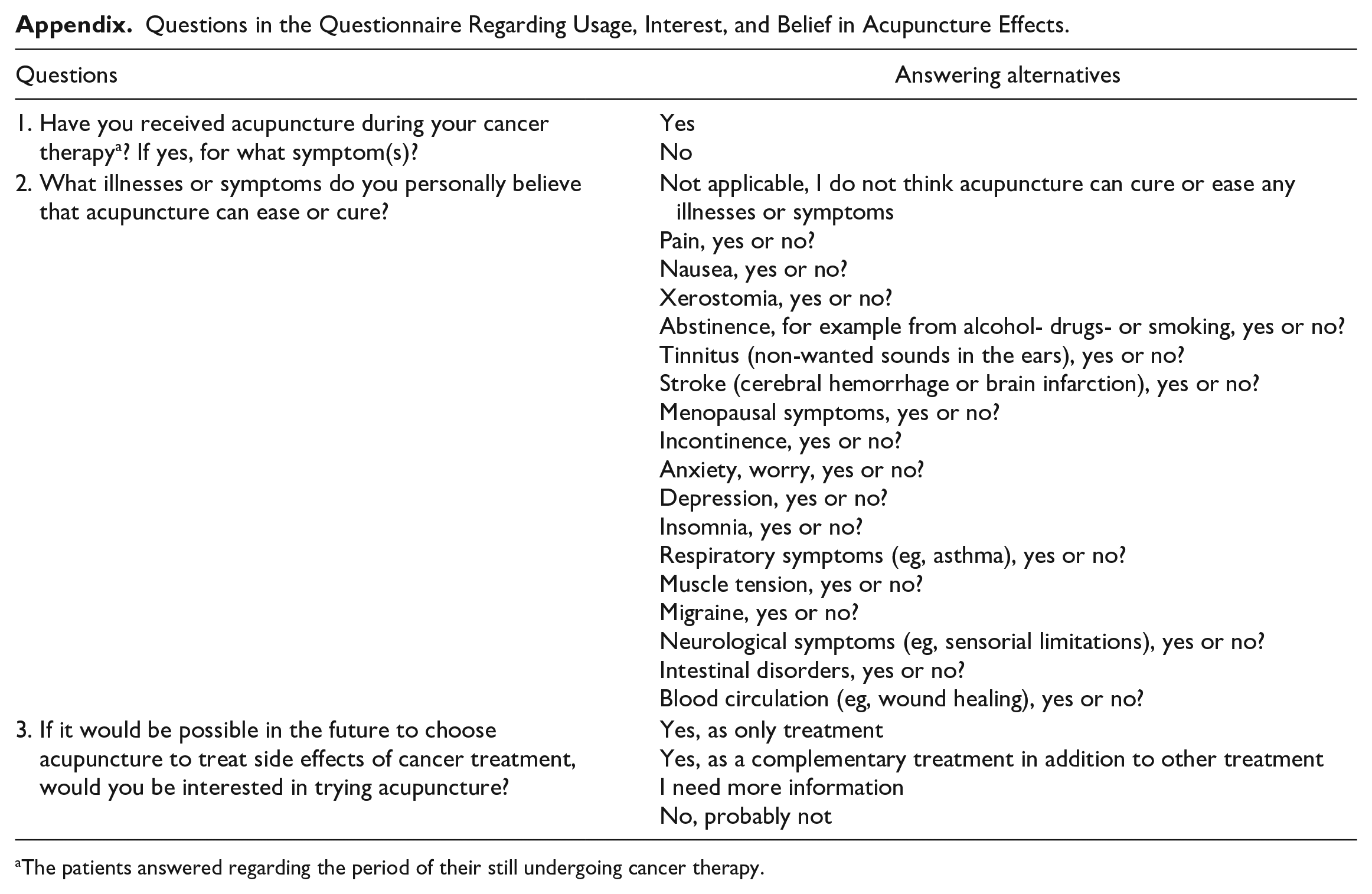
The patients answered the questions: “Have you received acupuncture during your cancer treatment?” (if yes, for what symptom(s)?) and “If it in the future was possible to choose acupuncture for the treatment of side effects from cancer treatment, would you like to try acupuncture?”. Further, they answered a question about their treatment expectations regarding acupuncture effects on symptoms commonly treated using acupuncture9,12-16 “What illnesses or symptoms do you personally believe acupuncture can ease or cure?” (regarding the 17 symptoms seen in Table 2) (See Appendix for complete questions and response alternatives).
Sociodemographic, occupational, clinical, and health characteristics
The patients provided characteristics regarding sociodemographic and occupational information as requested by the questionnaire. The questions included their highest educational level “Elementary school, High school, or College/University” and current occupational status. They also graded their health from 0; “worst imaginable health state” to 100; “best imaginable health state” using the generic valid and reliable EuroQol health barometer. 33 The coordinating radiotherapy nurses determined clinical characteristics, for example the type of cancer and type and dose of cancer therapy from the medical records.
Statistical Analyses
Data are presented as number (n) and proportions (%) for all variables, mean ± standard deviation (SD) for continuous variables, and median and percentiles for ordinal variables. We categorized patients who answered that they believed acupuncture to be effective (“Yes”) regarding at least 1 of the 17 symptoms asked for to “Yes, at least 1 symptom.” The number of symptoms for which each participant believed acupuncture to be effective was summed (number of “Yes” was summed, maximum 17). The sum was considered to be a proxy for the level of belief in acupuncture effects; the higher summed number, the more positive beliefs in acupuncture effects. The patients’ occupational status was categorized into “full-time sick-leave” or “part-time sick-leave,” leaving all other participants, including pensioners, in the category “not on sick-leave.”
The frequency of symptoms between the subgroups with different sociodemographic, occupational, clinical, and health characteristics were compared, using student’s independent t-test for 2 category variables (gender, and previous acupuncture experience) and ANOVA/GLM (General Linear Model) for more than 2 category variables (age, educational level, and occupational status), together with Tukey’s pairwise post hoc test in case of statistical significance. Further, multi-factor ANOVA with 2-way interactions between the subgroups was done. We obtained the regression coefficient from the ANOVA. The significance level was 5%. The data were analyzed with IBM SPSS Statistics Version 27.0, (Armonk, NY: IBM Corp).
Results
The Participants
Of the 507 included patients, data were provided for 457 participants, which is a 90% response rate (Figure 1). As seen in Table 1, the patients were mostly treated for breast cancer (n = 171, 38%) or prostate cancer (n = 145, 32%) The mean age of the patients was 65, ranging from 24 to 90 years. The patients older than 65 years were mostly retired. The patients 65 years or younger were mostly on sick leave if they were employed; 108 of the 151 employed patients (72%) were on sick leave. The study group had a rather equal distribution between men and women (48% vs 52%) (Table 1).
Characteristics of the Patients.
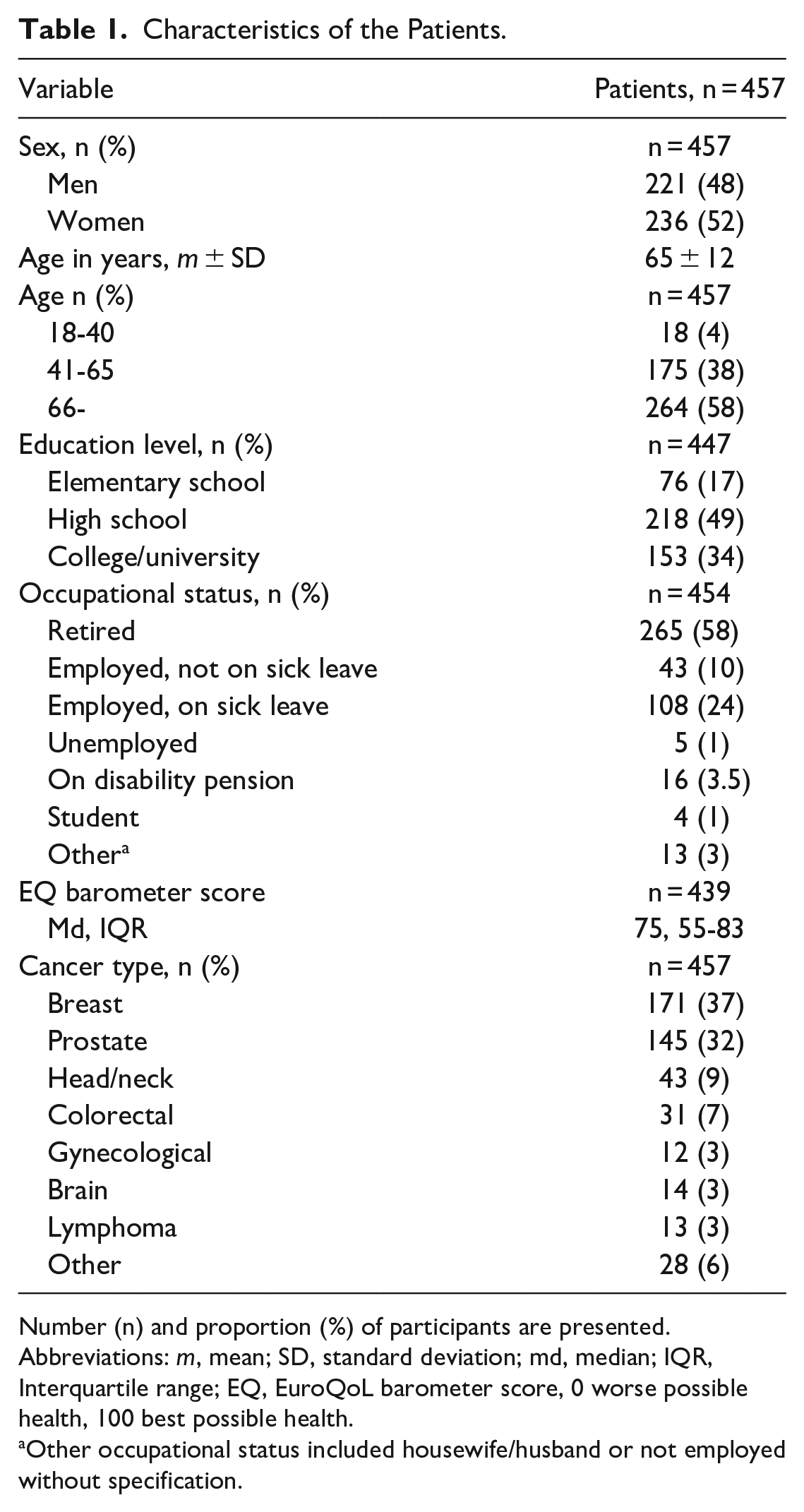
Number (n) and proportion (%) of participants are presented.
Abbreviations: m, mean; SD, standard deviation; md, median; IQR, Interquartile range; EQ, EuroQoL barometer score, 0 worse possible health, 100 best possible health.
Other occupational status included housewife/husband or not employed without specification.
The Use of and Interest in Acupuncture
Of the 457 participants, 444 patients reported data regarding usage of acupuncture. Four (1%) had used acupuncture at some time during their cancer therapy. The stated indications for this usage were to relieve pain, n = 2, or nausea, n = 2 (Table 2). Of 443 patients who replied to the question regarding interest in acupuncture, 368 (83%) expressed some kind of interest in acupuncture treatment for side effects during cancer therapy, either to receive the therapy or to receive more information on acupuncture (Figure 2).
Use of Acupuncture and Belief in Acupuncture Effects.

Number (n) and proportion (%) of participants are presented.
Abbreviations: m, mean; SD, standard deviation.
Of maximum 17 different symptoms.
Multiple choices were allowed.
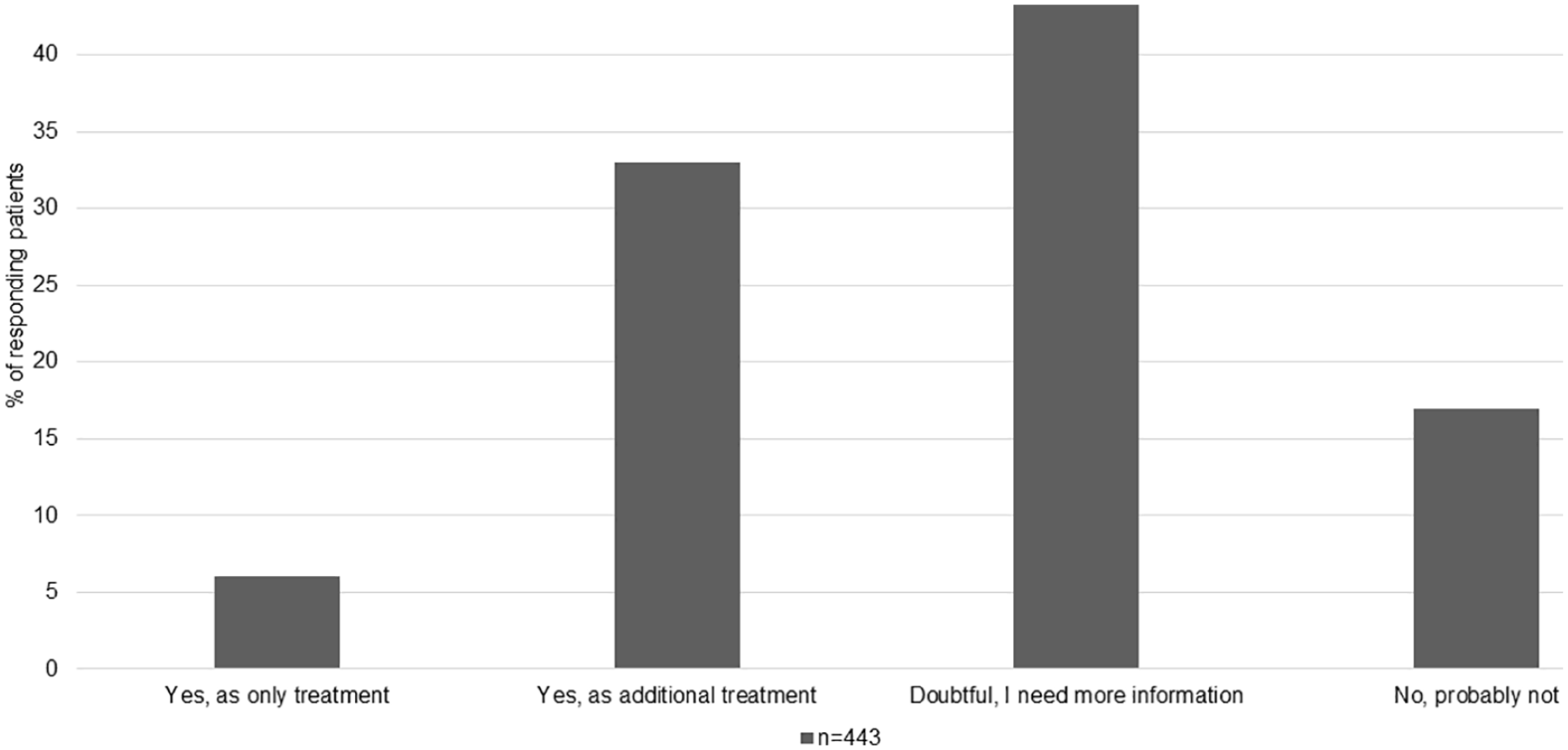
Patients’ interest in receiving acupuncture treatment.
Treatment Expectations: Belief in Acupuncture Effects
Of the 457 answering patients, 289 (63%) believed acupuncture to be effective for at least one of the requested symptoms. Of these, 56% believed acupuncture to be effective for pain and 40% for muscle tension. Few patients believed acupuncture to be effective for stroke (1%) and respiratory symptoms (4%). The patients believed acupuncture to be effective for a mean value of 3 out of 17 symptoms asked for (Table 2).
Differences in Treatment Expectations: Belief in Acupuncture Effects in Varying Subgroups
The univariable analysis suggested that women, patients aged 65 years old or younger, patients on sick leave, patients with gynecological cancer, and patients who had an experience of acupuncture usage during the cancer therapy had a stronger belief in acupuncture effects than other patients. The multivariable analysis confirmed that women had a stronger belief in acupuncture effects than men, and those aged 41 to 65 years had a stronger belief than those older than 65 years of age, while the other variables were not valid for explaining variations in beliefs in acupuncture effects (Table 3).
Belief in Acupuncture Effects in Subgroups of Patients With Different Sociodemographic, Occupational, and Clinical Related Characteristics.

Abbreviations: m, mean; SD,standard deviation.
Statistically significant difference between groups.
Of maximum 17 different symptoms.
Not in the analysis since cancer type was highly correlated to sex.
Reference category is the category with the lowest belief in acupuncture.
Tukey’s post hoc test showed age group 66- differ against the other groups.
Tukey’s post hoc test showed elementary school differ against the other groups.
Tukey’s post hoc test showed full time sick-leave and not on sick leave differ against the other groups.
m and SD was not appropriate for this category due to n = 4; median value with interquartile range was 8 and 9, 4 to 12 for “yes” and 2, 0 to 4 for “no.”
Not in the analysis since n = 4.
Discussion
This study found that two-thirds of patients undergoing cancer therapy believed acupuncture to be effective for a variety of symptoms. More than 80% stated any kind of interest in receiving acupuncture during cancer therapy but few of them reported any acupuncture usage. Women and middle-aged patients 41 to 65 years old believed acupuncture to be effective to a higher extent than men and those older than 65 years of age.
The observation that only a few patients received acupuncture during their cancer therapy in contrast to their high interest and belief in acupuncture effects raise questions regarding the degree to which shared decision-making 1 in integrative oncology 2 has been implemented. Further, the low utilization of acupuncture also raises questions regarding if the patients were not offered acupuncture for reasons related to the still rather low scientific evidence for acupuncture effects. There are still few well-conducted randomized controlled studies, using valid sham control methods to be able to control for non-specific effects, on symptoms commonly experienced during cancer therapy. 18 The finding that 83% were interested in receiving acupuncture or to receive more information on acupuncture treatment was in line with a previous study regarding specifically antiemetic acupuncture (n = 368 radiotherapy patients), where 79% were interested in receiving acupuncture, while none of the patients had actually used it. 19 Also Wode et al 20 observed that few (6%) of 755 Swedish patients undergoing cancer care reported usage of acupuncture since being diagnosed with cancer. Two German studies; 1 on 171 patients with cancer and 1 on 333 patients undergoing radiotherapy, presented that approximately 23% and 12% respectively, had used acupuncture during their cancer treatment.10,11 In another study, 72% of 497 patients with cancer were interested in receiving acupuncture during their cancer therapy. 29 Beside rather low scientific evidence for specific effects of acupuncture for cancer-related symptoms,9,12-16 other potential reasons for the low utilization of acupuncture, in contrast to the high interest and belief in acupuncture effects, may be a fear among the health care providers that acupuncture might have adverse effects, or that it is risky to combine complementary and conventional cancer treatments. 34 A negative or not open-minded attitude against integrative oncology in oncology health practitioners may potentially risk that patients do not ask for symptom-relieving acupuncture in contrast to their interest and belief in acupuncture effects. This has been exemplified in a study by Lettner et al, 11 where only 16% of 333 patients with cancer had discussed adding complementary treatment to their cancer therapy with their consulting physician. Suggested reasons for patients’ unwillingness to discuss complementary treatments with their physician are the doctor’s lack of inquiry; patient’s anticipation of the doctor’s disapproval, disinterest, or inability to help; and patient’s perception that disclosure of CAM use is irrelevant to their conventional care. 35
Two-thirds of the patients with cancer in our study believed acupuncture to be effective for a variety of symptoms during cancer therapy. This observation indicated a weaker belief among the patients with cancer in our study, compared to another study 29 where almost all (90%, 79%, and 80%) of 198 patients with cancer who were planned for acupuncture therapy believed acupuncture to be effective for cancer-pain, nausea, and vasomotor symptoms, respectively. In another study, three-quarters of 864 patients with either migraine, tension-type headache, low back pain or osteoarthritis of the knee believed acupuncture to be either very effective or effective. 6 Research has previously shown that higher expectancy is associated with a greater willingness to participate in acupuncture clinical trials, 36 which might explain the weaker belief among the patients in our study since they were not a selected population, recruited for any acupuncture trial.
The multivariate analysis showed 2 variables presenting a strong relation to the level of belief in acupuncture effects: a person’s sex (women had a stronger belief than men) and age (those of working age 41 to 65 believed more than those older than 65 years), in line with a previous study. 29 A previous study presented that being female increased the effects of sham acupuncture given by a therapist adopting an empathic and expectancy-strengthening therapist style. 37 Potentially, this was a finding driven by expectancy mechanisms, since positive expectancy and beliefs may produce positive treatment effects. 3 Previous research has also shown education level being strongly related to beliefs in acupuncture effects. 29 However, in our study education was highly correlated with age. Since age turned out to be such a strong factor in our study, the participants’ education level did not stand out as significant.
Experience of acupuncture usage during the cancer therapy was not included in the multivariable analysis due to low numbers of patients who had an experience in usage. According to our univariable analyses, the participants with acupuncture experience believed acupuncture to be more effective than the acupuncture-naïve respondents did, in line with previous observations. 29 Several studies have demonstrated the central role of learning from previous experiences, for shaping expectations and thus producing non-specific effects during treatments.3,38,39
In a previous randomized sham-controlled study (n = 200), patients with low treatment expectancy were more likely than other patients to experience diarrhea in terms of frequent stools during pelvic irradiation, irrespective of whether they received genuine or sham acupuncture. 40 Unfortunately, treatment expectations, that is, beliefs, were rarely measured in previous acupuncture studies.12-16,18 It seems highly important to measure treatment expectations and beliefs in studies evaluating effects of acupuncture, since beliefs have been seen to highly modify acupuncture effects.4,6,40 Since our study demonstrated age and sex-related variations in acupuncture beliefs, it is reasonable 3 that studies that are not sham-controlled lack internal validity to evaluate specific effects of acupuncture. If the women with strong beliefs in acupuncture effects in our study in the future would be randomized to either acupuncture or a control group receiving standard care, it seems reasonable that their positive acupuncture treatment expectancy may increase the effects of specifically the acupuncture therapy and not the effects of the standard care. Randomized controlled studies, without a sham-controlled design, thus do not seem to be enough to reveal specific effects of acupuncture.
Most patients in the study believed acupuncture to be effective for pain and muscle tension. More than half, 56%, believed acupuncture to be effective for pain and almost half, 40%, believed that acupuncture is effective for relieving muscle tensions. Fewer patients believed acupuncture to be effective for the other requested indications. This is in line with the experience in Swedish health care, where acupuncture has been an approved treatment specifically for pain since 1984 (the National Board of Health and Welfare SOSFS 1984:33). Almost 10 years later, in 1993, acupuncture was approved on the same premises as other medical treatments in Sweden; that is, it can be used on a variety of medical conditions, given that scientific evidence exists proving the effectiveness (SOSFS 1993:18). Still, the fact that acupuncture has been accepted and implemented within health care for pain and related symptoms, for example muscle tension, for a longer time than other symptoms, may be a contributing factor leading participants to believe acupuncture to be effective for pain and muscle tension symptoms in particular.
Treatment beliefs seem highly important to consider in the therapeutic context. Participants in our previous study 41 being treated by a therapist who emphasized the positive relaxing acupuncture effects increased their level of positive treatment expectations. Participants with a high baseline level of positive acupuncture expectations perceived almost doubled improvement in relaxation, compared to participants with low beliefs. 41 Overall, higher acupuncture treatment expectancy seems to lead to better results from the treatment.4,6 This exemplifies the importance of reinforcing expectations in those who are least likely to believe in a treatment, to secure positive prerequisites for positive treatment outcomes. The participants in our study were least likely to believe acupuncture to be effective for stroke and respiratory symptoms. Very few, just 1% and 4% of the patients, respectively, believed that acupuncture would be effective for these symptoms. In line with that result, there is only weak scientific evidence for beneficial effects of acupuncture on these particular symptoms.42-45
Regarding the methodology of this study, one strength is the high overall response rate of 90%, lessening the probability that non-participation influenced the results to such a degree that we would make erroneous interpretations. We used clinimetric31,32 single-item questions, previously seen to produce high answering rates.5,19,29,40 There are other acupuncture belief measurements available, often consisting of multi-items, not tested for validity and feasibility specifically in the target population of patients with cancer. 46 By excluding the patients who received their first or only radiation treatment on the study day, we excluded those who received single fraction radiotherapy, which mostly is given with palliative intention. We did not want to induce burden in patients undergoing their first day of radiotherapy, for ethical reasons.
To avoid potential therapist-induced bias, 34 the patients were asked to answer the questionnaire in private. In the data analysis, belief in acupuncture effects for a higher number of symptoms (continous data) meant a more positive belief in acupuncture effects. An alternative would have been to apply a dichotomized variable, based on whether the patients believed acupuncture to be effective for at least 1 symptom or not (nominal data). However, since so many patients believed acupuncture to be effective for pain, that alternative would not have contributed so much in providing knowledge on factors modifying beliefs in acupuncture effects.
The studied cohort consisted of rather equal proportions of men and women and there was a large variation in the types of cancer, indicating generalizability to both sexes and patients with different cancer types. The mean age was 65 years and all patients received cancer therapy in Sweden, where cancer care is primarily funded by the state. These characteristics may decrease the generalizability of the study findings to younger patients and patients from privately funded cancer care, since interest in a therapy may plausibly be related to willingness to pay for the therapy as well as invest in one’s health using CAM therapies. 47
The high interest in acupuncture treatment and positive treatment expectations, that is, beliefs in acupuncture effects, indicate that acupuncture treatment should be available for patients with cancer, for symptoms of which acupuncture has been shown to be effective in randomized sham-controlled studies. The strong beliefs in acupuncture effects and the age and sex-related differences in these beliefs, indicate the importance of collecting expectancy data in future randomized sham-controlled acupuncture studies to be able to treat expectancy as an effect-modifier. If health care professionals want to secure positive prerequisites for acupuncture treatment in terms of positive treatment expectations, an older, male patient with cancer may need more encouragement regarding positive expected outcomes of the acupuncture treatment than a younger female. We welcome further studies regarding the role of treatment expectations in maximizing the potential treatment effects of acupuncture.
Footnotes
Appendix
Questions in the Questionnaire Regarding Usage, Interest, and Belief in Acupuncture Effects.
| Questions | Answering alternatives |
|---|---|
| 1. Have you received acupuncture during your cancer therapy a ? If yes, for what symptom(s)? | Yes No |
| 2. What illnesses or symptoms do you personally believe that acupuncture can ease or cure? | Not applicable, I do not think acupuncture can cure or ease any illnesses or symptoms Pain, yes or no? Nausea, yes or no? Xerostomia, yes or no? Abstinence, for example from alcohol- drugs- or smoking, yes or no? Tinnitus (non-wanted sounds in the ears), yes or no? Stroke (cerebral hemorrhage or brain infarction), yes or no? Menopausal symptoms, yes or no? Incontinence, yes or no? Anxiety, worry, yes or no? Depression, yes or no? Insomnia, yes or no? Respiratory symptoms (eg, asthma), yes or no? Muscle tension, yes or no? Migraine, yes or no? Neurological symptoms (eg, sensorial limitations), yes or no? Intestinal disorders, yes or no? Blood circulation (eg, wound healing), yes or no? |
| 3. If it would be possible in the future to choose acupuncture to treat side effects of cancer treatment, would you be interested in trying acupuncture? | Yes, as only treatment Yes, as a complementary treatment in addition to other treatment I need more information No, probably not |
The patients answered regarding the period of their still undergoing cancer therapy.
Acknowledgements
We would like to thank all the participants in this study for their time and effort. We also thank the study coordinating nurses and physiotherapists for their valuable work collecting and entering data, and statistician Erling Englund for highly appreciated efforts to the statistical analyses.
Author Contributions
The authors have made substantial contributions to the conception and design of the study, and interpretation of data, drafting the article and have approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.