
Abstract
Background:
Music therapy or sound interventions were shown to confer beneficial effects in patients with cancer for instance in terms of pain or fear relief and improvement of other patient reported outcomes. Cardiovascular parameters, especially heart rate variability (HRV) were found to have prognostic implications in cancer patients. In this trial we aimed to investigate the effects of a sound intervention on cardiovascular parameters compared to rest in patients with cancer.
Methods and results:
Using a randomized cross-over design, 52 patients (male 13, female 39) with cancer were recruited to receive both a 15-minute sound intervention and a 15-minute rest intervention within 4 weeks with at least a one-week blanking period. Cardiovascular parameters (among others HRV, aortic pulse wave velocity [PWV], augmentation index [Aix], aortic blood pressure [BP], heart rate [HR]) were assessed immediately before (pre) and after (post) the intervention had taken place. HRV (Root mean square of successive RR interval differences [RMSSD, ms]) significantly increased, during sound intervention (median RMSSD pre 24 [range 5-112] vs post 22 [range 9-141], P = .03). Likewise, median PWV, as a direct marker of arterial stiffness, was significantly reduced by sound intervention ([m/s] pre 8.5 [range 5.6-19.6] vs post 8.3 [range 5.6-15.6], P = .04). For both parameters no statistically significant change during rest was observed. HR was lowered by both, rest (P < .0001) and sound intervention (P = .02), with a more pronounced effect by rest. A significant increase in systolic aortic blood pressure was shown by rest ([mmHg] median 101 [range 78-150] vs post median 103 [range 71-152], P = .04) but not during sound intervention (P = .59), while rest intervention led to a decrease in resistance index (pre median 33 [range 13-92] vs post median 32 [11-84], P = .02).
Conclusion:
In comparison with rest, a single sound intervention in patients with cancer improved cardiovascular parameters commonly associated with increased stress levels. Studies with longer follow-up and multiple interventions are warranted.
Trial Registration:
ISRCTN registry 70947363.
Introduction
Music therapy is a practically based scientific discipline which interacts with various scientific fields, especially medicine, social sciences, psychology, musicology, and education. 1 The term “music therapy” describes the therapeutic use of music and sound addressing different aspects, such as physical (eg, pain, unpleasant sensations), 2 emotional (eg, depression, anxiety),3,4 cognitive (eg, neurological impairments, confusion),5,6 and social needs (eg, isolation, loneliness)7,8 of patients. Due to beneficial effects on quality of life and patient reported outcomes, music therapy has gained importance in the field of palliative care. 9 However, there is also a growing interest of music therapy as part of supportive care in cancer patients in general.10,11
The diagnosis of cancer represents a challenging situation that is accompanied by a high degree of stress and fear. For this reason, the treatment focus is nowadays placed not only on cancer alone, but also on the emotional health of the patient as part of a holistic approach. 12 Stress is a major complaint in cancer patients. It affects the patient’s quality of life, and directly influences cardiovascular parameters through an increased sympathetic tone that can be objectively measured. This autonomic imbalance is associated with reduced heart rate variability (HRV) and increased arterial stiffness.13,14 Positive effects of music therapy on HRV have been demonstrated in healthy individuals and patients with cancer.15,16 However, it is unclear (i) to what extent music therapy or sound interventions influence other cardiovascular parameters as an expression of arterial stiffness and increased vascular tone and (ii) how this compares to structured rest periods. Thus, the present randomized cross-over trial study sought to investigate effects of sound intervention on different cardiovascular parameters compared to rest in patients with cancer.
Methods
Study Design and Setting
This randomized cross-over study was conducted at the Interdisciplinary Tumour Center, University Medical Centre Mannheim, University of Heidelberg, Germany. It was designed as a head-to-head comparison of music and rest intervention in patients with cancer. Recruitment started in November 2019 and ended in May 2020. Patients were not followed up (Figure 1, flow chart).
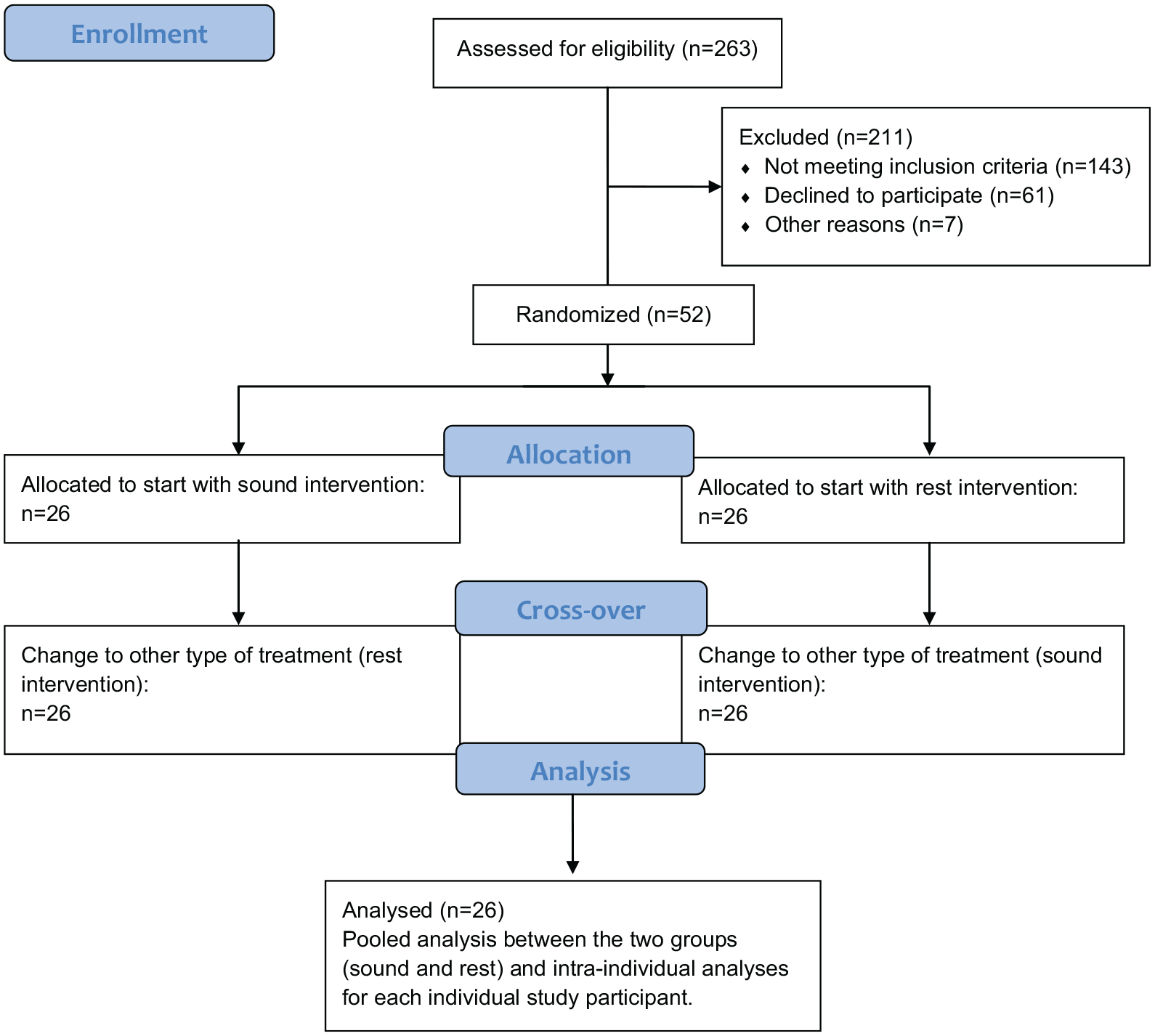
Flow chart depicting the different phases of the randomized controlled trial.
The study was conducted according to the principles of the declaration of Helsinki and was approved by the local ethical committee, Medical Ethics Commission II, Faculty of Medicine Mannheim, University of Heidelberg, Germany (2019-736N). Data protection was in accordance with the EU Data Protection Directive.
Study Population
Patients with histologically confirmed cancer aged >18 years were included in the study. Exclusion criteria comprised acute myocardial infarction or stroke (within the past 30 days), cardiogenic shock, indication for aortocoronary bypass operation, known minimal heart rate at rest below 50 bpm, need for pacemaker stimulation, hypotension with systolic blood pressure <80 mmHg or uncontrolled hypertension with systolic blood pressure ≥180 mmHg, bilateral axilla dissection, Parkinson’s disease or tremor of other origin, and atrial fibrillation. Treatment with cholinergic agonists/ antagonists or autonomic modulators (eg, betablockers) was not an exclusion criterion.
Variables
Patients characteristics
Baseline demographic and clinical characteristics were acquired using clinical charts, and patients were asked to fill in a questionnaire, which collected information about the emotional state, legal stimulants and especially about the musical experience. Patients were asked whether they liked listening to music and whether they played an instrument.
The use of concomitant medication with possible influence on vascular function, such as betablocker, antihypertensive drugs (angiotensin converting enzyme [ACE] inhibitor or angiotensin receptor blocker [ARB], calcium channel blocker) or statins was also documented, as well as treatment with analgesics or antidepressants.
Intervention
All patients received both, a 15-minute sound intervention and a 15-minute rest intervention as part of a cross-over design. Interventions were performed in lying position after a 10-minute resting period. In order to rule out a systematic bias, the sequence of intervention was randomized. The 2 interventions took place within 4 weeks with at least a one-week blanking period between the 2 interventions.
The sound intervention was performed with a body monochord called “Heaven and Earth” (http://klangkoerper.de/himmel-und-erde.html). 17 This instrument consists of a semi-open resonance body with 29 strings (24 of those in C1sharp, 2 in C2sharp, 2 C3sharp, and 1 in G3sharp) and is an established method in everyday clinical practice for music therapy.18,19 The monochord was placed on the chest during the intervention to ensure optimal transmission of the vibrations (Figure 2). The instrument was played for 15 minutes by one of the investigators in all patients (CR). Similarly, rest intervention was done in a lying position for 15 minutes after the 10-minute resting phase.

Demonstration of a music intervention with the body monochord “Heaven & Earth.” The proband (DW) is examined in a supine position with the instrument placed on the lower chest/abdomen. The strings are stroked with fingers by the examiner (CR). Written consent was obtained from the persons in the photo (DW and CR).
Cardiovascular parameters
Cardiovascular parameters were assessed non-invasively using the VascAssist 2 device (inmediQ GmbH, Butzbach, Germany) after a 10 minute resting phase before and after each (music or rest) intervention. The duration of VascAssist measurement is about 10 minutes. VascAssist is an established oscillometric medical device for determining arterial stiffness, with good correlation to invasively measured values.20-22 Four pneumatic cuffs were applied to both upper and lower arms. In addition to conventional vital parameters (heart rate [HR], blood pressure [BP]), the VascAssist provides aortic parameters, such as aortic pulse wave velocity (PWV) and aortic BP (both reflecting increased arterial stiffness up to end organ damage), and the augmentation index (Aix). Moreover, model-based parameters, such as resistance indices and systolic parameters are also calculated. An additional module provides HRV metrics (Root mean square of successive RR interval differences [RMSSD, ms]). HRV was also recorded in supine position over 10 minutes.
Analyses were performed offline with the VascViewer 2 software for Windows (iSYMED GmbH, Butzbach, Germany).
Of the described parameters, PWV and HRV are best established by substantiating data. PWV is a direct measure of arterial stiffness, whereby a value of >10 m/s is associated with an increased risk for cardiovascular events.23,24 RMSSD as measure of HRV shows a large age-dependent range.25-27 Higher values indicate increased HRV with better adaptability of the heart, whereby a value <20 ms is considered pathological.
Table 1 gives an overview of the cardiovascular parameters with an explanation of the characteristics that are measured.
Cardiovascular Parameters.

Outcomes
Improvement of HRV and reduction of PWV as an expression of direct stress reduction served as primary outcome measure. The secondary outcome was any change in vital signs (heart rate, blood pressure). All cardiovascular parameters were assessed non-invasively using the VascAssist 2 device at baseline and after the rest and sound interventions. Analyses are conducted as pooled analysis between the 2 groups (sound and rest) and as intra-individual analysis for each individual study participant.
Statistical Analysis
Analyses were performed using SAS 9.4. (SAS Institute Inc., North Carolina) by a statistician blinded to patient identity (IB). Demographic variables and computed variables are summarized by descriptive statistics (median and range). Categorical variables are analyzed using absolute frequencies and percentages. All patients received 4 measurements of cardiovascular parameters at 2 different times, 1 before and after rest intervention and 1 before and after sound intervention. Descriptive analyses of cardiovascular parameters were performed by measurement time point (pre and post) and by intervention (rest and sound). In addition, grouped boxplots were generated for illustration. Intraindividual differences between both measurement time points as well as between both interventions were compared using Wilcoxon signed rank test. P < .05 was considered statistically significant. All analyses are of explorative nature. A sample size calculation was therefore not performed in advance.
Results
The study group consisted of 52 patients (pts) with a median age of 59 years (range, 28-83). Thirty-nine (75%) of the patients were female. The most common tumor types were breast cancer (18 pts, 35%), gastrointestinal tumors (8 pts [15%] colorectal cancer, 4 pts [8%] gastric cancer), and lung cancer (6 pts [12%]). Forty-six patients (89%) were receiving chemotherapy and 1 pt (2%) radiochemotherapy during the investigations. Twenty-three percent (12 pts) were treated with curative intention and 75% (39 pts) received palliative treatment. Four patients (8%) received no treatment during the study period. Concomitant medication included analgesics (13 pts, 25%) and antidepressants (7 pts, 14%). Six patients (12%) received betablocker, 9 pts (17%) ACE inhibitor/ARB while calcium channel blocker or statins were used in 5 pts (10%).
Twelve patients (23%) indicated to be actual smokers, 15 pts (29%) regularly drank alcohol and 46 pts (89%) had daily intake of caffeine either with coffee or black tea. Fifty-one of 52 patients (98%) reported that they enjoyed listening to music, with 19 (37%) of them very often consciously listening to music, 22 (42%) occasionally and 11 (21%) rather seldom. Twelve patients (23%) reported to actively play an instrument.
Baseline characteristics are displayed in Table 2.
Baseline Characteristics.

Data are presented as median (range) or number (%).
Abbreviations: ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; n, number.
Cardiovascular Parameters
All parameters assessed are depicted in Table 3.
Cardiovascular Parameters.

Data are presented as median (range). Bold values mark statistical significance.
Aix@75, augmentation index standardized to a heart rate of 75 bpm (beats per minute).
Abbreviations: BP, blood pressure; LVET, left ventricular ejection time; LVPT, left ventricular plateau time; PRT, pulse raise time; PWV, pulse wave velocity; RMSSD, root mean square of successive difference.
Vitals
Neither rest nor sound intervention led to a change in brachial BP. A reduction in HR was observed, more pronounced for rest (P < .0001), but also for sound there was a median reduction of 2 beats per minute (P = .02).
HRV
In terms of HRV, we found that RMSSD was significantly increased during the sound intervention (P = .03). HRV remained unchanged during rest (P = .44).
Differences of RMSSD between rest and sound intervention for both total groups (a) and single individuals (b) are depicted in Figure 3.

Graphical illustration of RMSSD (ms): (a) for both rest and sound intervention (grouped analysis) with boxplots for pre and post intervention, as well as the difference (post-pre) and (b) individual values for rest and sound intervention marked as line with change from pre to post.
Resistance indices
Neither aortic impedance nor compliance index were affected by rest or sound intervention. Resistance index on the other hand decreased only during rest (P = .02), but not during sound intervention.
Aortic parameters
Aortic BP remained unchanged during the sound intervention, while there was a median increase in systolic BP of 1.5 mmHg during the rest intervention (P = .04). Aix (normalized to a HR of 75 bpm) was increased by both rest (P = .003) and sound intervention (P = .04). The aortic PWV on the other hand was only influenced by sound. Here, a significant median reduction of 0.2 m/s was observed after only 1 intervention (P = .04). Changes of the PWV are shown in Figure 4.
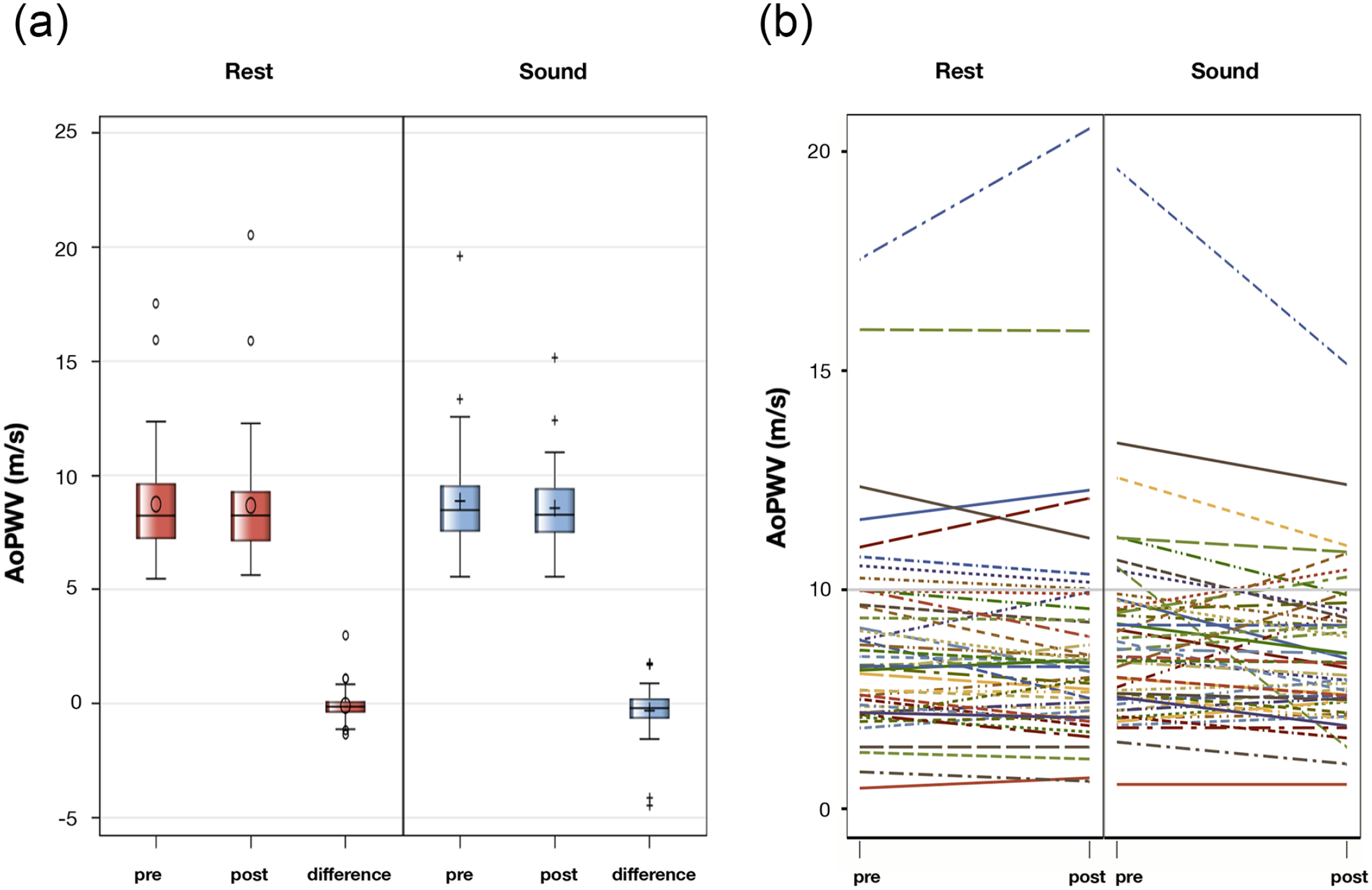
Graphical illustration of PWV (m/s): (a) for both rest and sound intervention (grouped analysis) with boxplots for pre and post intervention, as well as the difference (post-pre) and (b) individual values for rest and sound intervention marked as line with change from pre to post.
Systolic parameters
LVET as a measure of the systolic duration was extended by both rest (P < .0001) and sound (P = .0002), while extension of the LVPT was only observed during rest intervention (P = .007). Neither rest nor sound led to a change of the PRT.
Discussion
The present study investigated effects of sound intervention on cardiovascular parameters compared to rest in patients with cancer. Our main findings are:
1) Heart rate variability (HRV) metrics improved during sound intervention but not during rest periods.
2) Aortic pulse wave velocity (PWV) as a direct marker of arterial stiffness, was reduced only during sound intervention.
3) Heart rate (HR) was reduced by both rest and sound, with a greater effect during rest.
4) Rest intervention led to an increase in aortic BP and reduction of the resistance index.
The autonomic nervous system plays an important role, not only in a physiological setting, but also in various pathological settings, such as in cancer.28,29 HRV has become widely used to quantify cardiac autonomic regulation, 30 with different methods used for this purpose. The root mean square of successive differences (RMSSD) is used to quantify short-term HRV and reflects the vagal-mediated autonomic control of the heart, 31 while the low frequency-to-high frequency (LF/HF) ratio has been long considered as measure of cardiac sympatho-vagal balance, whereby an increase in LF/HF was assumed to reflect a shift to “sympathetic dominance” and a decrease corresponding to a “parasympathetic dominance.” 32 However, this assumption had to be put into perspective, which is why the RMSSD is primarily used to assess HRV as a more robust parameter. 33
The RMSSD reflects the normal rhythmic fluctuations of the heart and is an indicator of the ability of an organism to adapt the HR to physical and mental demands. A high RMSSD value reflects a good adaptability, with a balanced regulation by the autonomic nervous system, while a rigid frequency and low RMSSD value indicate an enhanced sympathetic tone in response to a higher stress level. 34 A reduced HRV was associated with a shorter survival time in an analysis of over 600 cancer patients. 35 Furthermore, a meta-analysis found a prognostic impact of HRV in terms of survival in cancer patients. 36 Thus, the determination of HRV in cancer patients is not only of scientific interest but may have prognostic implications. A single 15-minute sound intervention led to a HRV increase of a median 3 ms in our study. This is in line with other study results, which also showed an increase in HRV with a decrease in sympathetic nervous system activity.15,16,37 Since rest or a lying position could also influence the activation of the parasympathetic nervous system and thus HRV, all patients received both a rest intervention and a sound intervention, to rule out a systematic error. Although the rest intervention led to a more pronounced reduction in HR, no change in HRV was observed.
Whereas the stimulatory effect of the sympathetic nervous system on cancer initiation and progression has been well documented, the role of the parasympathetic tone is less well elucidated. 38 A possible protective effect of the parasympathetic nervous system was initially deduced from the reduced incidence of cancer in patients who received a vagotomy. 39 On the contrary, stimulatory effects have also been described, promoted by the cholinergic pathway. 40 However, the relationship between the sympathetic and parasympathetic nervous system is much more complex than previously supposed. The unidirectional idea that these are 2 antagonists has been largely abandoned. Instead, the ambiguity reflects the complex interplay. 41 HRV measurement is thus a simplified approach to translate this complex system into a single value, which can be easily obtained.
In addition, both rest intervention and sound intervention led to an increase in Aix in our cohort, which is physiological due to the reduction in HR and therefore no indication of increased arterial stiffness. 42 For the other parameters (LVET, LVPT) no clear trend was observed, whereas aortic BP was slightly increased by rest, while the resistance index declined. Whether this is actually an expression of increased tension (eg, due to ruminating thoughts in patients with cancer that could arise at rest) or a random observation cannot be answered on the basis of the available data. The median increase in blood pressure during rest therapy was only 1.5 mmHg in our cohort and is therefore not of clinical relevance. Whether this is a reproducible effect ought to be verified in a larger cohort.
In summary, a rest intervention does not seem to exert the same positive effects as a sound intervention does. This becomes particularly obvious when considering the PWV, which could be significantly reduced by the sound intervention exclusively. In cardiology, PWV is an important parameter in prevention and risk estimation. 43 A median reduction of 0.2 m/s, as achieved in our cohort, is therefore of clear relevance. An association between (emotional) stress and PWV as a cardiovascular risk factor and marker of arterial stiffness has been proven in several studies,14,44,45 as well as a reduction in PWV in healthy individuals by listening to music. 46 Interestingly, this effect was as strong for listening to classical music as it was for rock music, while the sham procedure (no music) showed no effects. 46
Above all, the observed significant changes in HRV and PWV seem to be of scientific interest. However, as this study is an exploratory investigation with no correlation of the results to actual physical and psychological outcomes of the patients, we can only speculate about the clinical implications. Therefore, further studies are needed to substantiate and verify our findings.
Strengths and Limitations
In order to rule out a systematic bias, all patients received an intervention with both rest and sound, whereby the choice of which intervention to start with was randomized. Thus, pairwise comparisons could be performed to take into account intra-individual differences. The VascAssist is a validated method for determining established parameters such as vitals, PWV, Aix, or HRV. However, the VascAssist also computes other, less well validated parameters. Due to the scarce available data, an interpretation is only possible in the context of already established parameters. Certain drugs are vasoactive and can therefore influence the results of the cardiovascular parameters. Although concomitant medication was recorded, treatment with drugs such as cholinergic agonists/ antagonists or other autonomic modulators (eg, betablockers) was not an exclusion criterion for study participation. We used a single intervention in this proof-of concept study and did not collect follow-up data. Thus, we are not able to determine a potential long-term benefit. Further trials with repeated interventions and measurements as well as randomized trials using patient-reported and/or survival endpoints are warranted.
Conclusion
A single sound intervention in patients with cancer exerted beneficial effects on cardiovascular parameters, especially HRV and PWV. Both parameters indicate an impaired vascular function, due to an enhanced sympathetic tone, as in the context of chronic stress exposure. In comparison, these effects were not observed during a rest intervention, which suggests that sound interventions are capable of significantly reducing stress levels. Our data suggest, that sound intervention may have the potential to benefit cancer patients in terms of reducing stress levels and beneficial impact on the course of tumor diseases, and should therefore be studied further as a complement to conventional anti-cancer therapies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.