
Abstract
Dear Editor,
We read carefully the Letter to the Editor sent by M. Notter et al. and appreciated the interest that these eminent colleagues have shown in our work. 1 Our narrative review has been a great scientific effort to offer useful information to promote hyperthermia treatments (HT) in the daily clinical practice of medical oncologists, surgeons and radiotherapists who practice integrated oncology treatments and palliative medicine as well as that of physicians who do not practice hyperthermia.
In order to write the review for publication in Integrative Cancer Therapies, we selected the most important articles and unfortunately excluded others that would equally deserve to be mentioned, since it was not possible for reasons of space to assemble all the data available on hyperthermia. At the same time, we tried to select the most important information for the tables, often simplifying the data for reasons of exposure and clarity. Our work was not limited to breast cancer alone but reported also data on 8 other types of cancer and it was sincerely our goal to arouse interest in the application of hyperthermia in oncology and not only in a particular type of cancer.
As concerning the recommendation of HT in the treatment of breast cancer of M. Notter et al. we agree about the need to improve the way in which studies are carried out, in particular, the need for a careful stratification and analysis of disease stages. The suggestion to subdivide clinical results according to breast neoplasms (irresectable preirradiated locally recurrent breast cancer, irresectable primary and metastatic disease) is certainly useful for clinical classification and would acquire greater significance if integrated with the well-known classifications of Luminal A, Luminal B, triple-negative/basal-like, HER2-enriched normal-like breast cancer. We will be able to practice locoregional treatments of hyperthermia and radiotherapy in a disease such as breast cancer which is very frequently metastatic at its onset by knowing its clinical and biomolecular parameters.
Regarding the field of metastatic breast cancer, there is currently a growing interest in palliative treatment of both hepatic and other organ metastases, such as pre-irradiated bone metastases, by associating hyperthermia to the metastatic site with systemic chemotherapy and novel immunotherapeutic agents.
This combination can add to the well-known characteristics of blood flow modification, increase in local oxygenation and drug concentration and therefore the efficacy of treatment.
Low doses of radiotherapy and/or HT can increase surface tumor antigens due to immunogenic cell death, 2 and HT increases lymphocyte trafficking and lymphocyte response, creating new avenues of care.
About the inaccuracies contained in Table 1 (see revised Table 1) we would like to specify that we initially recorded the Oldenborg et al. 3 data correctly as “≥G3 toxicity in 24%,” but due to a typograpical error it appeared as “>G3.”
Breast Cancer.
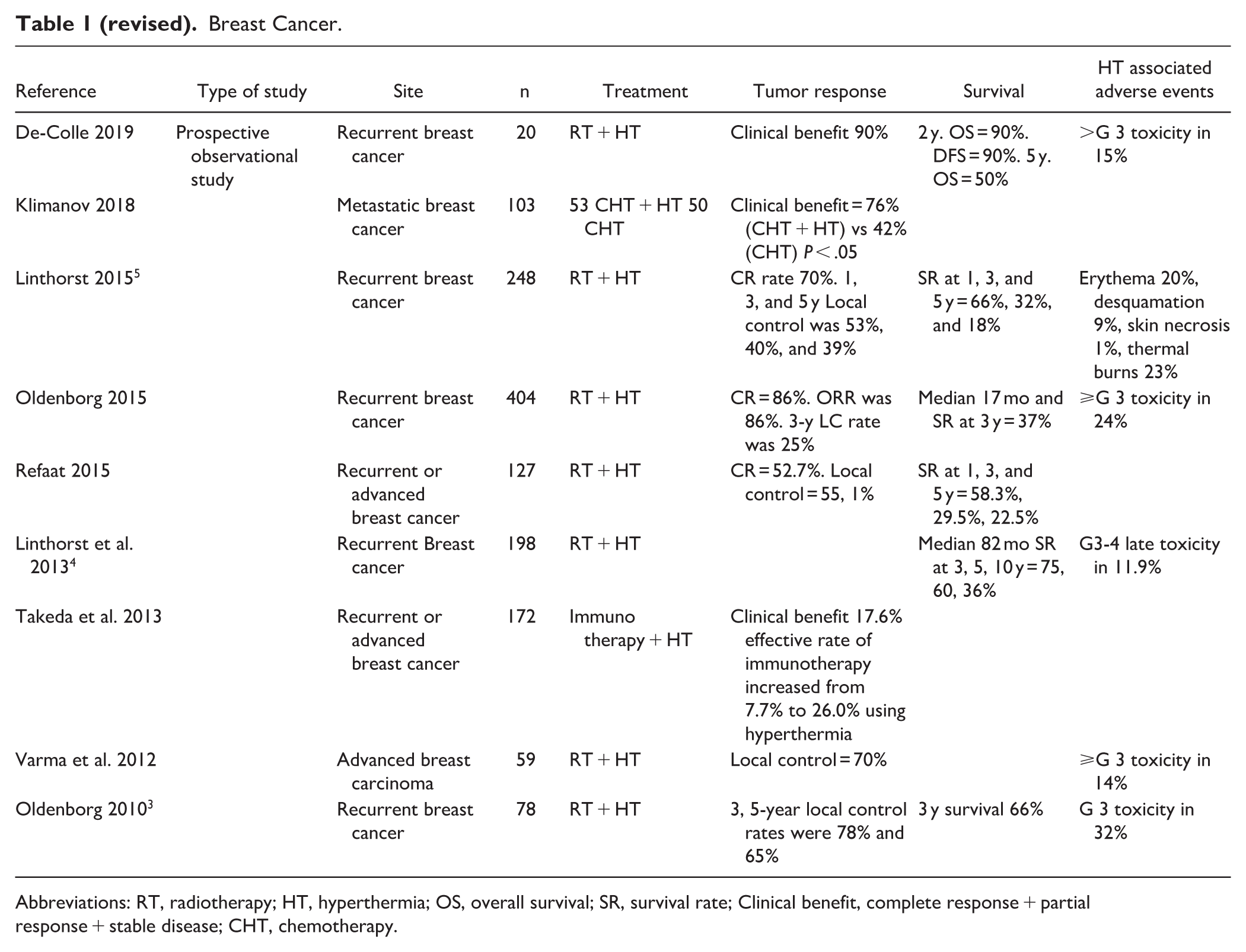
Abbreviations: RT, radiotherapy; HT, hyperthermia; OS, overall survival; SR, survival rate; Clinical benefit, complete response + partial response + stable disease; CHT, chemotherapy.
Linthorst et al. 4 wrote “Cumulative incidence of grade 3 and 4 late toxicity at 5 years was 11.9%,” yet we specify better the Linthorst et al. 5 data by adding details in Table 1.
We thank M. Notter et al. for their helpful comments, which add to the utility of our publication
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.