
Abstract
Introduction:
Type 1 gastric neuroendocrine tumors (g-NETs) have a good prognosis but a high recurrence rate.
Aim:
To observe the clinical efficacy of the treatment of type 1 g-NETs with the Chinese herbal decoction SMLJ01.
Materials and Methods:
A prospective and retrospective, clinical, controlled observation was conducted in 4 Chinese centers from 2012 to 2019. Patients with type 1 g-NETs were nonrandomly divided into treatment and control groups after endoscopic treatment based on herbal treatment administered according to their wishes. The treatment group received oral SMLJ01, with follow-up every 6 to 12 months, while the control group received follow-up alone. Patient follow-up (via telephone) from 2012 to 2017 was mainly retrospective. All patients after 2017 were followed prospectively. The recurrence times and rates were compared after treatment for at least 6 months. Symptom improvements were evaluated in the treatment group. The follow-up ended on October 31, 2019.
Results:
During a median follow-up of 22 months (range: 2-86 months), the survival rate was 100%, and no metastases occurred. Twenty-one of the 82 treated patients (25.6%) had recurrence after a median of 22 months, and 22 of the 54 control patients (40.7%) had recurrence after a median of 8 months (P = .063). The Kaplan-Meier curve analysis showed that the patients in the treatment group had a significantly longer median recurrence-free survival (RFS) time than those in the control group (P = .001). The risk of recurrence in the treatment group was 0.38 relative to that in the control group (95% CI: 0.20-0.70). The symptom score of the patients after taking Chinese medicine was 19.5 (10.3, 28.0), which was significantly lower than before treatment (31.5 (19.3, 38.0)). The difference was statistically significant (P < .01).
Conclusion:
SMLJ01, with the effects of soothing the liver, strengthening the spleen, increasing acid and harmonizing the stomach, may help reduce the recurrence rate, relieve symptoms and prolong the recurrence time in patients with type 1 g-NETs and is worthy of evaluation with further randomized research with large sample sizes and longer follow-up periods.
Introduction
Type 1 gastric neuroendocrine tumors (g-NETs), which derive from enterochromaffin-like cells (ECL cells), are the most common subtype of gastric neuroendocrine neoplasms. Generally, the prognosis of type 1 g-NETs is so good that the European Neuroendocrine Tumor Society (ENETS) guidelines only recommend regular follow-up after endoscopic treatment. 1 However, the recurrence of type 1 g-NETs is relatively common, and a prospective study found that the recurrence rate was as high as 63.6%. 2 However, the current measures to prevent recurrence are still controversial. To take full advantage of the TCM concept of “prevention of diseases” in the treatment of type 1 g-NETs, Professor Tan made many clinical observations. She found that the main clinical symptoms were postprandial fullness and belching, which are most common in the category of “liver depression and spleen deficiency.” The formula “SMLJ01” is based on soothing the liver, strengthening the spleen, increasing acid, and harmonizing the stomach. A previous study suggested that the formula could significantly prolong the recurrence time, reduce the recurrence rate, and reduce symptoms. 3 To further explore the effects of SMLJ01, a nonrandomized controlled observation was performed to provide a reference for the prevention of recurrence and improvement of symptoms in patients with type 1 g-NETs.
Materials and Methods
General Information
A prospective and retrospective, clinical, controlled observation was conducted in 4 centers from April 2012 to April 2019. After endoscopic treatment, patients were nonrandomly divided into the treatment group and the control group based on herbal treatment administered according to their wishes. Patients in the treatment group received oral SMLJ01, with follow-up every 6 to 12 months, while the patients in the control group received follow-up alone. Patient follow-up (via telephone) from 2012 to 2017 was mainly retrospective. All patients after 2017 were followed prospectively. This study was approved by the Clinical Research Ethical Committee of China-Japan Friendship Hospital (ethics approval number: 2017-115). The requirement for informed consent was waived (only verbal consent provided via telephone) in the retrospective part of the study.
Diagnosis and Recurrence Criteria
Diagnostic criteria
According to the 2006 version of the ENETS guidelines 4 and the 2016 version of the Chinese expert consensus on gastroenteropancreatic neuroendocrine neoplasms, 5 the major and minor diagnostic criteria were as follows: (1) patients were diagnosed with gastric neuroendocrine neoplasm (g-NEN) by gastroscopy, histopathology, and the criteria defined in the 2010 WHO classification; 6 (2) the detection of serum gastrin indicated hypergastrinemia (if the patients were taking PPIs or H2 blockers, the treatment was stopped at least 2 weeks before the laboratory tests were performed); (3) 24-hour gastric pH monitoring indicated achlorhydria; (4) parietal cell antibodies (PCA) or vitamin B12 deficiency was present; and (5) there was no acid reflux and no heartburn to rule out type 2 g-NENs.
Patients who met the first 2 criteria and 1 of the final 3 criteria were diagnosed with type 1 g-NETs.
Recurrence criteria
A criterion for recurrence was established by the experts in the Department of Pathology, Gastroenterology, and Oncology who were on the team at our neuroendocrine tumors center according to the ENETS guidelines and clinical experience. The definition of type 1 g-NET recurrence was as follows:
Endoscopic appearance (Table 1) combined with biopsy pathological results could be divided into the following cases:
For patients who had undergone a complete resection, once a new lesion (ie, the number of polyps and/or the maximum diameter increased) was found and confirmed to be g-NEN by histopathology, we judged that the tumor had relapsed;
For patients who had undergone an incomplete resection, if the number of polyps and/or the maximum diameter increased (such as an increase from Level A to Level B), and g-NEN was confirmed by histopathology, tumor recurrence was diagnosed, whereas if the number of polyps and/or the maximum diameter remained the same or even decreased, the tumor was considered to have not progressed.
The Evaluation of Gastroscopic Manifestations of Type 1 g-NETs.

Inclusion criteria
Inclusion criteria for the treatment group
The inclusion criteria for the treatment group were as follows: (1) patients who met the type 1 g-NET diagnostic criteria; (2) patients who had not received other medications after endoscopic resection (such as somatostatin analogue [SSA], etc.); (3) patients who were willing to participate, could take the Chinese herbal decoction, and adhered to regular follow-up (6-12 months); and (4) patients who signed the informed consent statement (no informed consent was signed in the retrospective part of the study).
Inclusion criteria for the control group
The inclusion criteria for the control group were as follows: (1) patients who met the type 1 g-NET diagnostic criteria; (2) patients who had not received any other treatments after endoscopic resection; (3) patients who were willing to participate and adhered to regular follow-up (6-12 months); and (4) patients who signed the informed consent statement (no informed consent was signed in the retrospective part of the study).
Treatment
The endoscopic manifestations after endoscopic resection (such as endoscopic submucosal dissection [ESD], endoscopic mucosal resection [EMR] or biopsy with forceps) were used as the baseline during follow-up assessments. The patients were divided into the treatment group or the control group according to their wishes. Patients in the treatment group received regular oral administration of SMLJ01 (interruptions of no more than 3 months per year and no more than 7 days per month) for at least 6 months and follow-up every 6 to 12 months, while the patients in the control group received follow-up alone. The SMLJ01 decoction was composed of raw hawthorn 30 g, Radix Bupleuri 10 g, Chinese Angelica 10 g, raw Radix Paeoniae Alba 12 g, Codonopsis pilosula 15 g, Rhizoma Atractylodis Macrocephalac 15 g, Poria cocos 15 g, pericarpium citri reticulatae 10 g, Pinellia ternate 9 g, Radix Aucklandiae 10 g, Amomi Fructus 6 g, chicken gizzard-membrane 15 g, fried Fructus Aurantii 10 g, roasted malt 15 g, vinegar curcuma zedoaria 10 g, Oldenlandia Diffusa 30 g, and baked Radix Glycyrrhizae 6 g. Professor Tan adjusted the SMLJ01 with some other Chinese herbs according to the patients’ symptoms, but the main herbs did not change. The prescriptions were dispensed in our hospital pharmacy to ensure uniformity of quality control. After the patients received the herbal medicine from our hospital pharmacy, according to their wishes, they could boil the herbs with water at home or ask the TCM decoction room staff in the hospital to decoct all herbs simultaneously. The administration schedule was as follows: 1 dose per day, divided into 2 servings given during morning and evening hours, 250 mL each time. Each follow-up visit involved gastrointestinal endoscopy and pathological examination. The clinical symptoms were recorded using a questionnaire which was devised especially for our study according to the common clinical symptoms of type 1 g-NET, referring to the symptom severity classification in the clinical guidelines for new drugs using traditional Chinese medicine. 7
Observation indexes
The primary outcome indicator was time to first recurrence following treatment; secondary outcome indicators were the recurrence rate and symptom improvement. Considering the common clinical symptoms of type 1 g-NET, the total symptom score was computed based on 15 symptom items, including postprandial fullness, belching, poor appetite, diarrhea, fatigue, and constipation, and so on. Each symptom was evaluated by the participant using the following score: 0 = no symptoms; 1 = mild symptoms; 3 = moderate symptoms; and 5 = severe symptoms. The higher the score, the more severe the symptoms are. The symptom questionnaire was completed by the patients once before the treatment and once after treatment for at least 6 months.
Data analysis and statistical evaluation
Data are expressed as the median (range or 25-75th interquartile range, IQR). Analysis of recurrence-free survival (RFS) was performed by the Kaplan-Meier method. Univariate and multivariate analyses for risk factors were performed with the Cox proportional hazards regression model. The P value was considered statistically significant when it was <.05. All statistical analyses were carried out using dedicated software (IBM-SPSS Statistics version 20.0).
Results
General Characteristics
A total of 136 patients were included in this study from 2012 to 2019; 7 patients were lost to follow-up in the treatment group, and 4 patients were lost to follow-up in the control group. The others completed the follow-up. Between 2012 and 2017, data on 57 patients were collected retrospectively, and from 2017 on, data on 79 patients were collected prospectively. The main reason for loss to follow-up was refusal to receive a regular follow-up. During the follow-up period, the survival rate was 100%. The follow-up period ranged from 2 to 86 months, with a median of 22 months. There were 82 patients in the treatment group (M:F = 32/50), and the average age of the patients was 51 ± 10.0 years (range: 29-71 years). The time of the treatment ranged from 6 to 86 months with an average of 32 months. There were 54 patients in the control group (M:F = 19/35), with ages ranging from 28 to 72 years and a mean age of 51 ± 9.9 years. There were no statistically significant differences between the 2 groups in terms of sex (P = .651) or age (P = .426). However, statistically significant differences regarding the depth of tumor invasion, histopathological classification and endoscopic therapy were found between the 2 groups, and mucosal infiltration and incomplete resection were more common in the treatment group than in the control group. Although the tumor grade was predominantly G1 in both groups, the proportion of G1 tumors was higher in the control group. The clinicopathological information of the 2 groups is presented in Table 2.
The Clinicopathological Characteristics of the 2 Groups of Patients.

Comparison of Recurrence
During the follow-up, 21/82 (25.6%) patients in the treatment group had tumor recurrence, and the median time to the first recurrence was 22 months. Of those 21 patients, 2 (9.5%) patients had a second recurrence. However, 22/54 (40.7%) patients in the control group experienced recurrence (median time to recurrence 8 months); 6 (27.3%) had a second recurrence, and 1 patient (27.67%) had 6 episodes. The recurrence rate in the treatment group was slightly lower than that in the control group (P = .063), but a Kaplan-Meier curve analysis showed that the patients in the treatment group had a significantly longer median RFS time than those in the control group (P = .001), and the median time to recurrence was also significantly longer (P = .015). The risk of recurrence in the treatment group was 0.38 relative to that in the control group (95% CI: 0.20-0.70). Related indices of recurrence in the 2 groups are shown in Table 3, and the RFS curves of the 2 groups are shown in Figure 1.
Recurrence-Related Indicators in the 2 Groups of Patients.

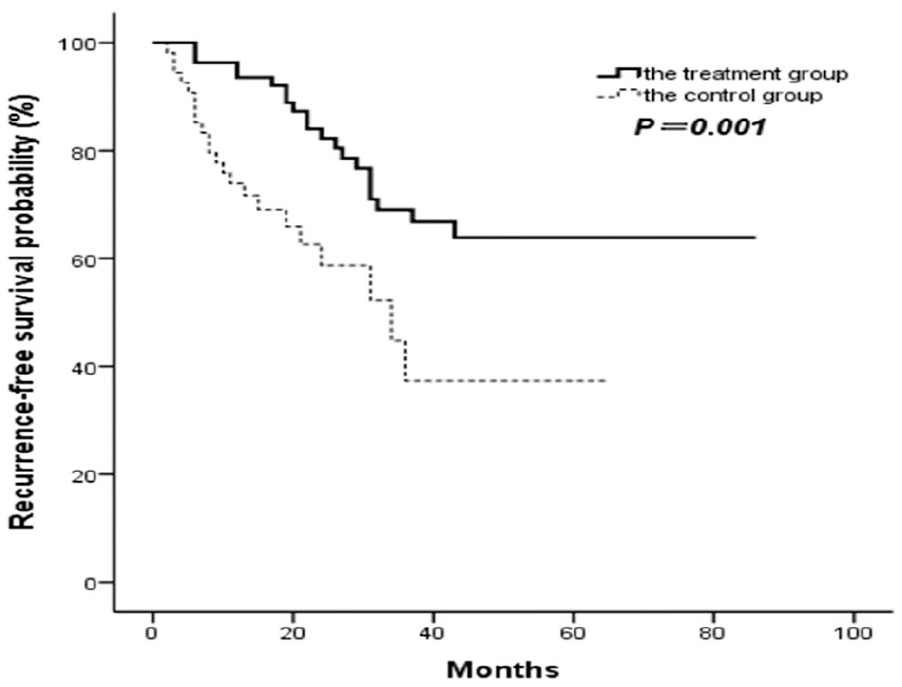
Recurrence-free survival curves of the 2 groups.
Symptomatic Response
The comparison of symptom scores before and after treatment with SMLJ01 was performed on 40 patients in the treatment group. The symptom scores of the patients before treatment were 31.5 (19.3, 38.0), and the scores after the treatment were 19.5 (10.3, 28.0). The situation is shown in Figure 2. The symptom scores significantly decreased after treatment, and there were significant differences in the symptom scores before and after treatment (P < .01), which indicated that the symptoms were alleviated effectively following treatment with SMLJ01.

Comparison of symptom scores of the treatment group.
Risk Factors for Recurrence
Table 4 shows the analysis of possible risk factors for type 1 g-NET recurrence using a Cox proportional hazards model. As shown in the table, univariate analysis identified that being treated with SMLJ01 was a protective factor against recurrence. The risk of recurrence in the control group was 2.64 times higher than that in the treatment group (95% CI: 1.43-4.86, P = .002). Multivariate analysis suggested that in addition to being treated with SMLJ01, age equal to or greater than 50 years was another protective factor against recurrence. Contrary to our original hypothesis, we found that the risk of recurrence at age ≥50 years was only 0.25 times as much as that at age <50 years (95% CI: 0-0.23, P = .009). However, no significant associations were found for sex, tumor size, number of lesions, depth of tumor invasion, histological grade, endoscopic therapy, or H. pylori infection (P > .05).
Analysis of Possible Risk Factors for Type 1 g-NET Recurrence.

Variables with P < .306 in univariate analysis were retained in multivariate regression analysis (available case analysis).
Discussion
With the development of endoscopic technology and the improvement of people’s awareness of disease, the incidence rate of g-NEN has increased from 0.031 per 100 000 people in 1975 to 0.49 per 100 000 people in 2014. 8 Among them, type 1 g-NET is the most common subtype, and most have a good prognosis. 5 Due to its relatively low degree of malignancy, the ENETS guidelines recommend endoscopic follow-up and lesion resection as the first choice for the treatment of type 1 g-NET in general, instead of surgical resection. According to this guideline, ECL cell carcinoids develop through the sequence of hyperplasia-dysplasia-neoplasia in hypergastrinemic conditions, leading to relatively common relapse. Antrectomy has been suggested to achieve gastrin suppression to prevent recurrent disease, 9 but a few cases of recurrence even after surgery have been reported. 10 Somatostatin analogues (SSAs) have been used to manage type 1 g-NETs, as SSAs can inhibit gastrin release and directly inhibit endocrine cell proliferation.11-13 However, SSAs cannot relieve symptoms. On the contrary, they may cause or aggravate gastrointestinal symptoms.
Thus, this study was designed to observe the clinical efficacy of the treatment of type 1 g-NETs with SMLJ01 with the goal of providing patients with a simple and inexpensive therapy. Our results show that after a median of 22 months of follow-up, the recurrence rate of patients in the treatment group was only 25.6%, which was lower than that in the control group (40.7%). The patients in the treatment group had a significantly longer median time to recurrence than those in the control group (14 additional months). Through the implementation of a controlled observation, SMLJ01 has been shown to be appreciably effective at preventing the recurrence of type 1 g-NETs. Moreover, the symptom scores of the 40 patients after treatment with SMLJ01 were significantly lower than those before treatment, suggesting that SMLJ01 has a good effect on improving the symptoms of type 1 g-NETs to some extent. Nevertheless, this study is a preliminary study, and the formula should be further investigated in larger randomized trials for reducing recurrence rates, relieving symptoms and prolonging recurrence time. Further analysis suggested that being treated with SMLJ01 and age equal to or greater than 50 years were protective factors against recurrence. However, none of the other factors analyzed had a significant effect on the recurrence, similar to the results of the study by Merola et al, 2 and we conjecture that the results were influenced by the presence of too many confounding factors and the small sample size. Future research with larger sample sizes is needed to confirm these associations.
In this clinical observational study, type 1 g-NETs were more prevalent in women and were usually small (less than 1 cm) and multicentric, similar to the results that have been reported in the literature.14-16 Type 1 g-NETs are associated with type A chronic atrophic gastritis (CAG), but only 79.5% of the patients in this observation were diagnosed with CAG through gastroscopy or pathology. One possible reason is that endoscopic gastric mucosal atrophy is atypical. Another possible reason may be related to incomplete biopsy. Therefore, the extensive experience of the endoscopy doctor is very important in the clinical diagnosis and treatment of type 1 g-NETs. In addition, a multipoint biopsy of the gastric antrum, body, and fundus should be performed to determine the presence of comorbid diseases. In contrast, according to the literature, only approximately 5% of patients with type A CAG eventually develop type 1 g-NETs. 17 Hypergastrinemia acts as an effective promoter of ECL cell proliferation but is unable to induce the hyperplastic changes of ECL cells to transform them into carcinoid tumors. There are also other contributing factors that may affect tumor formation, such as gene mutation, infection, diet, and environment.18,19 A multicenter, retrospective study showed that male sex, chromogranin A (CgA) > 61 U/L, and intestinal metaplasia were independent risk factors for type 1 g-NETs in patients with CAG. 20
The Chinese herbal decoction SMLJ01 is a modification of Xiaoyao San and Xiangsha Liujunzi decoction, and the acid (the “sour taste” among the 4 properties and 5 tastes in the concept of Chinese medicine) of hawthorn was added to relieve the deficiency in gastric acid secretion. Pharmacology studies and animal experiments have shown that Xiaoyao San has diverse functions in the gastrointestinal tract, including improvement of the impairment of gastric emptying and the regulation of gastrointestinal motility. 21 It has positive antitumor, antidepression, liver protection, endocrine regulation, and other effects. 22 Xiangsha Liujunzi Decoction can improve the function of cellular immunity, 23 and it plays roles in protecting the gastric mucosa, regulating stomach smooth muscle movement, inhibiting gastric mucosal edema, regulating endocrine activity, and promoting gastric emptying.24-26 The combination of the 2 formulas achieves the effects of soothing the liver, strengthening the spleen, increasing acid and harmonizing the stomach. Hawthorn, a traditional Chinese medicine and food, can not only regulate gastrointestinal motility, promote the secretion of digestive enzymes, and protect the liver but also exert antibacterial and antitumor effects in the digestive system. 27
There are multiple therapeutic targets during the occurrence and development of type 1 g-NETs. Dou et al 3 found that SMLJ01 might play a role in affecting ECL cell proliferation to prevent recurrence, that is, controlling the development of dysplasia and even tumor formation. Meanwhile, it can relieve atrophic gastritis and increase gastric acid levels to a certain extent. They also found that the expression of miR-202-3p (a tumor-regulating gene that is highly expressed in type 1 g-NET tumor tissues) was significantly reduced in the gastric mucosa tissue of patients who did not experience recurrence during treatment with SMLJ01. 28 Therefore, it can be speculated that the regulation of this molecule may play a corresponding role in the occurrence and recurrence of type 1 g-NETs and even the mechanism underlying treatment with SMLJ01. The specific molecular regulation mechanism is still being studied.
In this study, the recurrence rate of patients with type 1 g-NETs treated with SMLJ01 was lower than that of patients in the control group, and the recurrence time was significantly prolonged. At the same time, the symptoms of patients were effectively relieved. We have speculated that the traditional Chinese medicine SMLJ01 has a significant effect on the prevention of the recurrence of type 1 g-NETs to some extent and is worthy of further research in the clinic through controlled clinical observations. The shortcoming of this study is that the overall sample size is still small, although a multicenter study was conducted. Multicenter randomized studies with large sample sizes and longer follow-up periods are necessary in the future, and they may better investigate the effectiveness of SMLJ01 at preventing the recurrence of type 1 g-NETs and enable the exploration of the risk factors for the onset and recurrence of type 1 g-NETs. It is our hope that these studies may, in the future, serve as a guide to clinicians, leading to the prevention of the occurrence of these tumors.
Footnotes
Authors’ Note
This study was previously presented as an abstract and poster at the European Neuroendocrine Tumor Society (ENETS), March 11-13, 2020, Barcelona, Spain.
Author Contributions
YC collected, analyzed the data, and wrote the manuscript. DH collected and analyzed the data. JZ, JC, and HH provided data support. DD, XW, BY, CW, and ZQ helped with follow-up of patient. XZ provided support in the statistical analysis. JL performed endoscopy examination. JL reviewed the specimens for pathological diagnosis. HT designed the study, prescribed Chinese herbal medicine for patients, and critically revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (NSFC; grant number 81673763).
Ethical Approval
The study was approved by the Clinical Research Ethical Committee of China-Japan Friendship Hospital (ethics approval number: 2017-115).