
Abstract
Small molecule receptor tyrosine kinase inhibitors (SM-TKIs) are among a group of targeted cancer therapies, intended to be more specific to cancer cells compared with treatments, such as chemotherapy, hence reducing adverse events. Unfortunately, many patients report high levels of diarrhea, the pathogenesis of which remains under investigation. In this article, we compare the current state of knowledge of the pathogenesis of chemotherapy-induced diarrhea (CID) in comparison to SM-TKI–induced diarrhea, and investigate how a similar research approach in both areas may be beneficial. To this end, we review evidence that both treatment modalities may interact with the gut microbiome, and as such the microbiome should be investigated for its ability to reduce the risk of diarrhea.
Introduction
Gastrointestinal toxicity, commonly manifesting as diarrhea, is a common side effect of a range of cancer treatments including chemotherapy and tyrosine kinase inhibitor targeted therapy. This toxicity is currently without a specific prevention or treatment strategy, and can affect between 50% and 80% of patients, depending on their treatment protocol. 1 Diarrhea, and associated intestinal ulceration, can lead to a host of severe issues including dehydration, malnutrition, fatigue, renal insufficiency, and increased risk of systemic infection. 2 In addition to the severe compromise in quality of life, for people experiencing one or more of these side effects, treatment breaks or dose reductions are likely, leading to less effective cancer care and compromised remission rate. 3 Available economic data suggest that each episode of severe diarrhea requiring hospitalization may cost up to US$6616; however, this may be accompanied by broader costs related to emergency medical procedures or loss of productivity from time out of work.4-6 As such, effective preventative and treatment strategies for cancer treatment–induced diarrhea are critically needed. By understanding the pathogenesis of this diarrhea, identification of appropriate treatment targets may be expedited.
Small molecule tyrosine kinase inhibitors (SM-TKIs) are used to treat a variety of solid tumor types including lung, breast, and head and neck cancers. 7 They are used in combination or as a monotherapy, increasingly as first-line therapy. 8 Most act by binding to the intracellular adenosine triphosphate (ATP) domain of the tyrosine kinase, preventing downstream signaling and subsequent cell division and growth. 9 While there are a large variety of targets, the most common are the epidermal growth factor receptors (EGFRs) and vascular endothelial growth factor receptors (VEGFRs). 8 SM-TKI diarrhea usually occurs in the first week of the treatment course and is typically managed with antidiarrheal agents such as loperamide.10,11 However, for many patients, loperamide does not sufficiently reduce diarrhea, and/or causes side effects including fatigue, constipation, and abdominal pain.11,12 Thus, there is merit in investigating new targets for this diarrhea.
Comparatively, the mechanism of diarrhea stemming from chemotherapy has had far more research than mechanisms of diarrhea from SM-TKI treatments. 13 This is, in part, likely due to the length of time these treatments have been available. Chemotherapy-related diarrhea occurs due to direct damage to the intestine, initiating a host of inflammatory pathways eventually leading to ulceration and potential bacterial translocation. 14 It was previously assumed that SM-TKI and chemotherapy toxicity had the same pathogeneses; however, recent research has posited that they have different initiating events and mechanisms, and are therefore specific, separate toxicities.13,15 While it is now clear that there are treatment-specific mechanisms that differ between SM-TKI–induced diarrhea and chemotherapy-induced diarrhea (CID; similarly to CID and radiation-induced diarrhea), there is a strong evidence base, explored here, to suggest that they share core mechanisms relating to direct mucosal damage, changes to chloride secretion, and upregulation of inflammatory processes.16,17 Given the variance in the literature surrounding the mechanisms of cancer treatment–induced diarrhea, we propose that taking a similar research approach to elucidate the causes of both chemotherapy- and SM-TKI–induced diarrhea may be beneficial in further building our understanding.
The gut microbiome is gaining momentum as a key research and therapeutic target in cancer therapy–induced toxicities. 14 Changes in the microbiome following chemotherapy have been clearly shown; however, we do not yet fully understand how to manipulate the microbiome, or determine the microbial-mucosal interactions that accelerate gut toxicity and diarrhea. 14 In SM-TKI treatments, initial indications suggest altered microbial composition in people experiencing more severe diarrhea. 18 While there appears to be differences in the mechanisms of SM-TKI–induced diarrhea and CID, these results suggest that both are underpinned by changes in the microbiome. Additionally, when the microbiome is compromised via antibiotics in both treatment modalities, diarrhea and treatment efficacy outcomes are altered.19-21 Given the suggestion that the microbiome may be a common and targetable mechanism of both SM-TKI–induced diarrhea and CID, we propose that similar to the research into the microbiome in CID, a similar research approach is taken with SM-TKI–induced diarrhea.
This review will focus on comparing the pathogenesis of diarrhea stemming from highly mucotoxic chemotherapies (5-fluorouracil [5-FU] and irinotecan) with diarrhea induced by EGFR and VEGFR inhibitors used for the treatment of solid tumors. The benefits and drawbacks of taking a similar research approach to determining the mechanisms of both of these types of diarrhea will be explored. Additionally, we will examine the potential of the gut microbiome to play a key role in both of these treatment modalities.
Diarrhea Incidence in Chemotherapy and SM-TKI Cancer Treatments
Chemotherapy
Cytotoxic chemotherapies irinotecan and 5-FU are 2 agents known to cause high levels of gastrointestinal toxicity, with up to 80% of patients developing at least some level of diarrhea. 2 The National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) classifies a diarrhea grading over 3 (increase of ≥7 stools per day over baseline; hospitalization indicated; severe increase in ostomy output compared with baseline; limiting self-care activities of daily life) as severe. 22 As single agents, 5-FU (bolus) has rates of up to 32% severe diarrhea, and weekly irinotecan has rates of up to 22% severe diarrhea. 2 Combination therapy, often in the form of FOLFIRI (5-FU, folinic acid, and irinotecan), is commonly used in a variety of cancer types (Table 1) and is also associated with high risk of gastrointestinal damage (severe diarrhea = 12% to 20%).23,24 Adverse effects of these highly mucotoxic chemotherapies are often managed with loperamide, octreotide, or nonpharmacological interventions, such as oral rehydration, but still commonly require treatment breaks and dose reductions.23,25
Comparison of Diarrhea Incidence in Highly Mucotoxic Chemotherapies and VEGFR and EGFR TKIs a ..
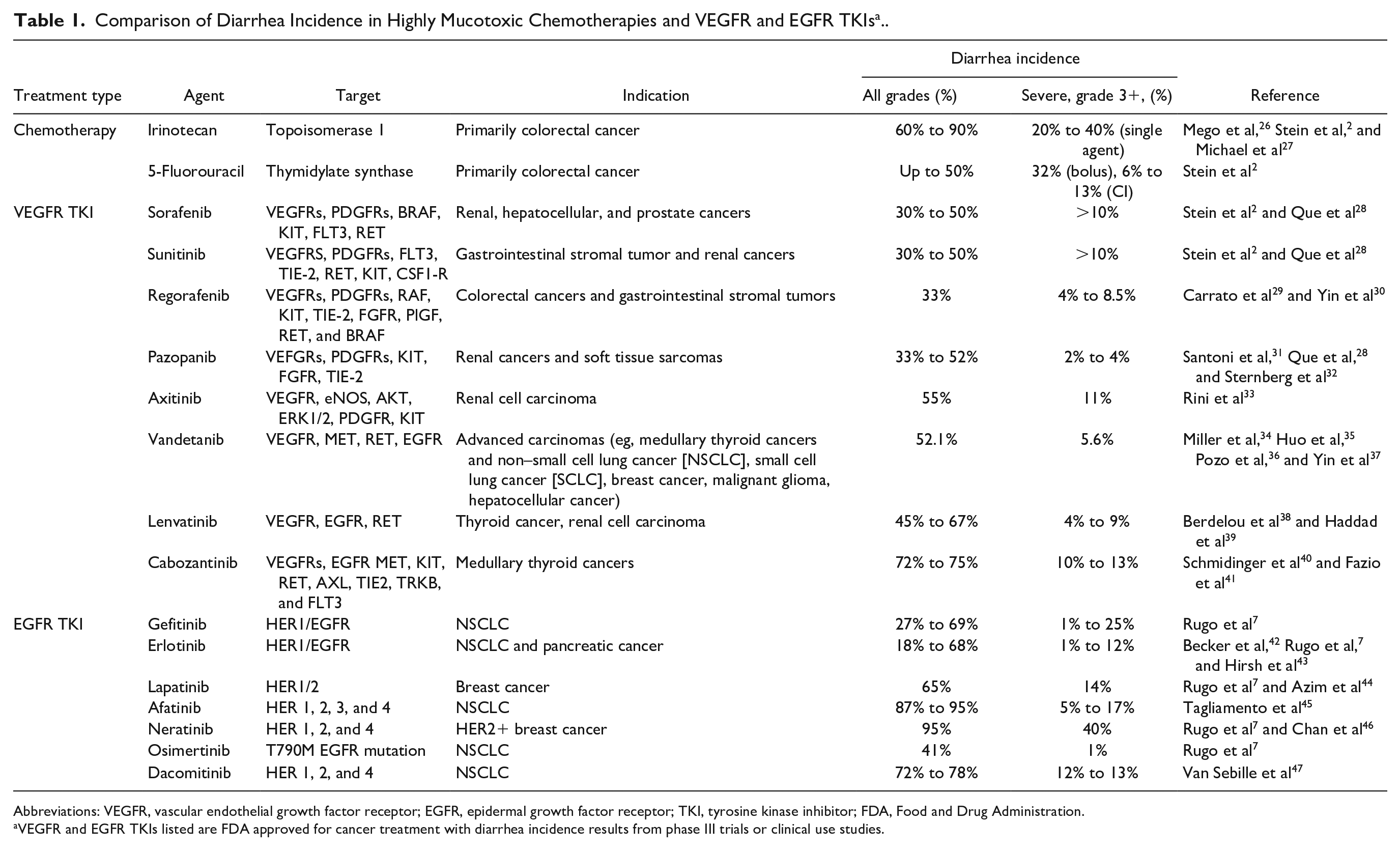
Abbreviations: VEGFR, vascular endothelial growth factor receptor; EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor; FDA, Food and Drug Administration.
VEGFR and EGFR TKIs listed are FDA approved for cancer treatment with diarrhea incidence results from phase III trials or clinical use studies.
SM-TKIs
SM-TKIs are growing in use as cost-effective, orally administered agents known to inhibit extremely important oncological targets in a range of cancers (Table 1).48,49 After dermatologic toxicity, diarrhea is the most common side effect of SM-TKI treatment, and it is often severe enough to require a break in treatment or a dose reduction. 7 Unlike chemotherapy, it is important to consider that SM-TKI treatments are often taken daily for long periods (months-years), meaning that even low-grade diarrhea can have significant impacts on patient quality of life. Therefore, proactive and clinically effective management of side effects is required to enable treatment to continue successfully and reduce the risk of chronic side effects that are less common in the relatively acute chemotherapy setting. 50
EGFR TKIs, a common group of SM-TKIs, are associated with diarrhea that typically occurs early in a treatment course (often within the first week), similar to chemotherapy. 7 Severe diarrhea is common, occurring in up to 25% of cases (Table 1), requiring individualized management (lowered dosing, diet modification, and intravenous fluids and electrolytes) to reduce the risk of hospitalization and treatment delays. 7 Clinical data have shown patients receiving second-generation multi-EGFR SM-TKIs, such as afatinib and dacomitinib, have a higher incidence of severe, grade 3 diarrhea compared with first-generation agents (eg, gefitinib), which are more target specific and less likely to inhibit other tyrosine kinase groups. 10 Diarrhea associated with VEGFR-TKIs in monotherapy is predominantly mild to moderate (Table 1) but needs to be managed as early as possible (with antidiarrheal agents including loperamide) in order to avoid symptoms progressing to more severe, higher grade diarrhea. 51 VEGFR-TKIs are also often given in combination with chemotherapy, which can cause a compound effect of more severe diarrhea. 51 For example, in the ICON6 trial of combination platinum-based chemotherapy and VEGF inhibitor cediranib, 39% of people in the intervention arm had to stop the trial early with highly toxic diarrhea and fatigue. 52 Anecdotal evidence has also suggested that diarrhea following cediranib treatment leads to a sustained reduction in health-related quality of life. 51
Chemotherapy Toxicity in Comparison to SM-TKI Toxicity
Chemotherapy
Currently, diarrhea from chemotherapy treatment is largely understood to follow the 5-phase model proposed in 2004, and updated in 2010 and 2019.14,53,54 Briefly, initiating events such as reactive oxygen species generation and DNA damage lead directly to transcription factor activation (eg, nuclear factor κB [NF-κB]) and pro-inflammatory cytokine release, leading to apoptosis and mucosal ulceration.14,55 This eventual thinning of the mucosal layer from activation of these inflammatory pathways can lead to bacterial translocation and an inability to properly absorb fluids from the intestine, eventuating in diarrhea. In this vein, indirect biological signaling is the basis of much of the damage, as opposed to direct tissue damage by chemotherapy itself. Current research is attempting to understand the connection of the microbiome to the host immune response underlying this signaling, specifically targeting the role of inflammation and the enteric nervous system. 14
SM-TKI: Direct Target Inhibition
SM-TKI–induced diarrhea is likely to be multifactorial, and there are multiple hypotheses currently under investigation. One such hypothesis surrounds the inhibition of the specific kinase targets in the intestinal epithelium. EGFR and VEGFR are both highly expressed in the gut, and inhibition in the intestine leads to lowered cell proliferation and reduced capillary networks in the intestinal villi, respectively.56-59 EGFR pathways also have stimulatory effects on enterocyte proliferation and nutrient and electrolyte transport, causing structural and functional changes when inhibited. 16 These changes in the intestinal architecture may lead to mucosal atrophy and thereby a reduction in the absorptive capacity of the gut. However, many SM-TKI agents have multi-targeted activity. For example, sorafenib is able to block tyrosine kinases in the VEGFR, PDGFR, BRAF, KIT, FLT3, and RET families. It is, therefore, challenging to determine how inhibition of which particular kinase targets affects diarrhea levels and how this could be used to reduce diarrhea without affecting treatment efficacy.7,60 In EGFR SM-TKIs, second-generation agents, which have a broader inhibitory profile, have more diarrhea of any level, and also more severe diarrhea compared with the first-generation agents. 7 Diarrhea is also the most frequent adverse event for the Food and Drug Administration–approved third-generation agent osimertinib, which targets the T790M mutation of EGFR, but has a low affinity for wild-type EGFR. 61 In a phase I escalation trial, diarrhea increased with escalating doses of osimertinib, suggesting that direct target inhibition by osimertinib may be involved in the development of diarrhea. 61 In a larger phase III clinical trial of 253 patients with non–small cell lung cancer, 47% of patients developed diarrhea.62,63 Similar to multi-kinase EGFR SM-TKIS, in VEGFR SM-TKIs, diarrhea is observed at higher levels in the more common multi-kinase inhibitors such as sorafenib compared with pure VEGFR inhibitors.51,64
SM-TKI: Chloride Secretion
Despite evidence that direct inhibition of EGFR and VEGFR may drive diarrhea following treatment, preclinical SM-TKIs have shown differing results around intestinal histopathological damage. Multiple SM-TKI studies have demonstrated a lack of this histopathological damage.17,65,66 As this damage is a hallmark of chemotherapy-induced gastrointestinal toxicity, this vast histopathological difference has been a driving factor for the hypothesis that SM-TKI–induced diarrhea has a distinctly different mechanism than CID. However, in a recent preclinical study, the EGFR-targeting SM-TKI dacomitinib caused significant blunting and fusion of the villi in the ileum, 66 challenging the notion that chemotherapy and SM-TKI–induced toxicities are unrelated. One recent hypothesis has theorized that diarrhea from SM-TKIs (in particular EGFR TKIs) had a secretory phenotype.13,16 In secretory diarrhea, activation of chloride channels including the cystic fibrosis transmembrane conductance regulator (CFTR) and calcium-activated channels increases fluid secretion into the lumen, and inhibition of intestinal sodium transport lowers fluid absorption. 67 In the intestine, EGFR has an inhibitory effect on chloride secretion, and it has, therefore, been hypothesized that SM-TKI inhibition of EGFR allows excessive chloride secretion into the gut lumen. 16 Studies have additionally shown that in ex vivo models, potassium channels as well as CFTR chloride channels are directly activated by EGFR TKI treatments including afatinib, gefitinib, and lapatinib. 68 Additionally, preclinical rat studies have suggested that EGFR inhibitor dacomitinib-induced diarrhea was of a secretory form, and clinical studies of neratinib show a fecal osmotic gap consistent with secretory diarrhea.66,69 Crofelemer is an anti-chloride secretory medication currently being trialed clinically to reduce diarrhea in HER2+ breast cancer being treated with EGFR targeting monoclonal antibodies (NCT02910219).70,71 However, targeting secretory changes in a dacomitinib rat model using crofelemer actually worsened diarrhea levels.16,66 In addition, preclinical studies of neratinib and lapatinib have both shown no changes in serum chloride levels.17,50 Collectively, this leaves the role of chloride secretion unclear and requiring further investigation.
SM-TKI: Inflammation
Inflammation is known to have a key role in the development of CID 72 ; however, it has only more recently been considered as a factor in SM-TKI–induced diarrhea. In chemotherapy, upregulation of inflammatory pathways is a key part of the 5-phase model. Inflammasome activation and pro-inflammatory cytokine release has been shown to mediate irinotecan-induced gastrointestinal damage and diarrhea.73,74 In addition, 5-FU treatment causes upregulation of a host of pro-inflammatory cytokines including tumor necrosis factor-α, interleukin-1β, interleukin-6, interleukin-17A, and interleukin-22. 75 Activation of the Toll-like receptor (TLR) signaling pathways leads to upregulation of many of these inflammatory mediators, and it has recently been implicated in irinotecan-induced diarrhea. 76 A mouse model demonstrated that TLR4 knockout mice had reduced diarrhea and other clinical indicators of gastrointestinal toxicity. 76 Similarly, a preclinical study of diarrhea from neratinib also showed potential for inflammation to be involved by demonstrating that budesonide, a locally acting corticosteroid, reduced levels of diarrhea and colonic injury, as well as increasing levels of anti-inflammatory interleukin-4 levels. 17 This result has been reflected in data reported by Liu and Kurzrock showing a marked alleviation in EGFR-TKI–induced diarrhea following budesonide administration. 77 Furthermore, the STEPP trial of panitumumab in colorectal cancer showed that patients receiving prophylactic doxycycline for skin toxicity developed less diarrhea than patients on a reactive skin treatment regimen (15% vs 32%, n = 95). 78 While panitumumab is an EGFR-targeting monoclonal antibody, its side effects display many similar features of SM-TKI treatment. 79 It has since been suggested that as doxycycline may have acted as an anti-inflammatory, the diarrhea may have had an inflammatory component. 43 Alternatively, it could be speculated that the antibiotic nature of doxycycline altered the gut microbiota to influence diarrhea development through other pathways. Together, these findings have suggested that while SM-TKIs and chemotherapies induce diarrhea via different preliminary mechanisms, initiation of inflammatory processes may be a key contributing factor to its development following both treatment types.
Potential Role of the Microbiome in Chemotherapy and SM-TKI Treatment Diarrhea
While it has been widely posited that chemotherapy and SM-TKI treatments induce diarrhea via different mechanisms, interventions targeting these hypotheses have so far been unable to definitively reduce diarrhea. Therefore, using similar research methods to that used to elucidate CID may be useful to rule out or more fully understand mechanisms underlying SM-TKI–induced diarrhea. The gut microbiome could potentially play a key role in both treatments due to its relation to inflammatory responses and chloride secretion (Figure 1).
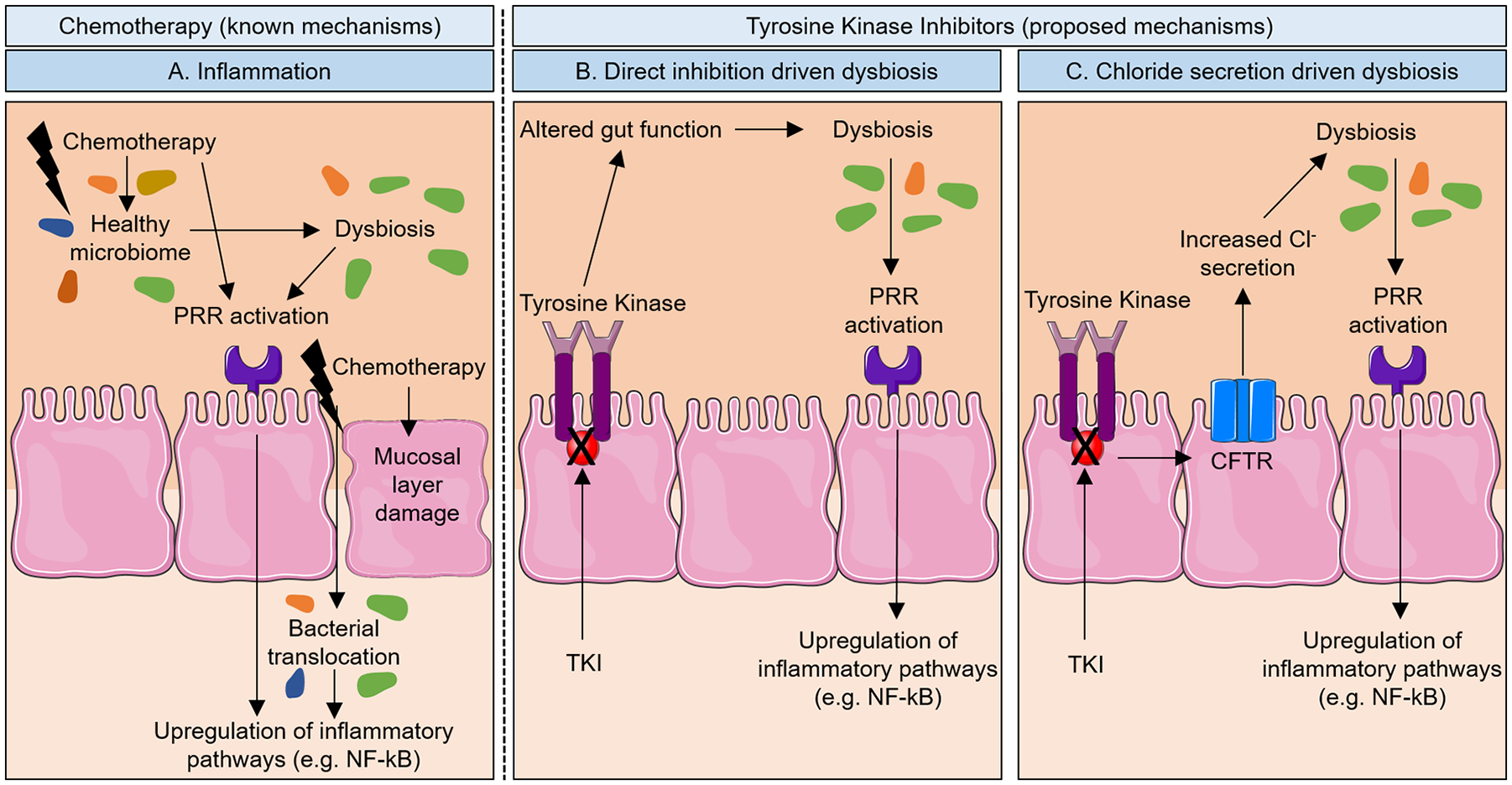
Potential interactions of the gut microbiome with tyrosine kinase inhibitor (TKI) treatments leading to diarrhea. (A) Chemotherapy causes vast changes to the gut microbiome,80,81 as well as activation of inflammatory pathways via pattern recognition receptors (PRRs), such as Toll-like receptor 4,53,76 that lead to ulceration and eventual diarrhea. TKI treatment also leads to diarrhea, but the mechanism is not well understood. We propose that the gut microbiome may play a key role. (B) Long-term TKI treatment may lead to a dysbiotic microbiome. 18 Additionally, direct inhibition of EGFRs or VEGFRs in the gut can lead to altered gut function (eg, changes in cell proliferation and capillary networks) that can alter microbial composition.56-59 This could lead to similar inflammatory outcomes as in chemotherapy. 17 (C) Alternatively, increased chloride secretion in the gut (causing diarrhea itself) 16 could lead to a significant shift in the microbiome that may lead to additive effect on the diarrhea.18,82,83
Intestinal Inflammation
The gut microbiome has been shown to play an integral role in mediating intestinal inflammation. This has been demonstrated in inflammatory bowel disease, where there is a marked decrease in microbial diversity and richness compared with healthy controls. 84 Similarly, in Crohn’s disease, the treatment-naïve microbiome is strongly correlated with disease status, with increased abundance of Enterobacteriaceae, Pasteurellaceae, Veillonellaceae, and Fusobacteriaceae occurring along with decreases in Erysipelotrichales, Bacteroidales, and Clostridiales in people with the disease. 85
The gut microbiome is proposed to mediate these inflammatory responses via the innate immune system and has a particularly important role in the development of this system. For example, preclinical studies have demonstrated that early life exposure to commensal bacteria is required to develop appropriate invariant natural killer T-cell tolerance. 86 Additionally, dysbiosis of the microbiome can alter levels of metabolites from the microbiome such as butyrate. Butyrate is a short-chain fatty acid produced by colonic bacteria by fermenting elements from our dietary intake. It can induce regulatory T (Treg) cell development to maintain immune tolerance and maintain the balance between Th17 and Treg cells. 87 This balance is highly important in modulating intestinal inflammation. Finally, the gut microbiome and innate immune system are intrinsically linked via many types of pattern recognition receptors (PRRs). TLRs are important in sensing molecular patterns originating from the gut microbiome, such as lipopolysaccharide (LPS), that cause activation of downstream signaling pathways of transcription factor (eg, NF-κB) upregulation and pro-inflammatory cytokine release.
Chloride Secretion
In addition, there is an emerging link between gut microbiome composition and intestinal chloride secretion, particularly via CFTR, which allows exit of chloride ions across the apical membrane. Two studies have investigated this link with lubiprostone, used clinically to treat constipation and known to stimulate electrogenic chloride secretion.88,89 Upregulation of chloride secretion with this agent caused large shifts in the stool microbiome, with an increased abundance of Lactobacillus spp in the stool of lubiprostone-treated mice. It was concluded that epithelial chloride secretion may have a key role in influencing bacterial-epithelial interactions. In addition, changes to the CFTR have also shown to cause significant gut microbial changes. In a mouse model, CFTR gene mutations were sufficient to alter the gut microbiome, 82 and in a clinical study of 31 patients aged 1 to 6 years with cystic fibrosis (who have mutations in the CFTR), it was suggested that gut microbiota enterophenotypes were direct expressions of altered intestinal function. 83 These studies show the close links between chloride secretion and the gut microbiome. As excess chloride secretion into the intestinal lumen may cause diarrhea in some SM-TKI treatments, this provides further evidence for SM-TKI–induced diarrhea to be influenced by gut microbial changes. However, while there is some evidence that probiotic bacteria or pathogenic bacteria can alter chloride secretion,90,91 there are low levels of evidence to suggest that the native gut microbiome changes are able to drive chloride channel dysfunction. Future work needs to be done to understand whether microbial dysbiosis is a direct driver of diarrhea, or whether the diarrhea itself causes dysbiosis as an outcome.
Microbiome Changes Due to Cancer Treatment
Preclinical studies have shown marked changes to overall microbiome composition in the gut following chemotherapy treatment, toward a dysbiotic state. The key finding has been a decrease in commensal bacterial species, along with a corresponding increase in pathogenic species.80,81,92-94 These pathogenic species were usually gram-negative species, which can release LPS known to initiate the inflammatory pathways that are key mediators in development of diarrhea.95,96 Clinical studies have shown similar findings, with a decrease in total bacterial abundance and diversity, as well as decreases in commensals such as Lactobacillus and Bifidobacteria, with increases in Bacteroidetes and Escherichia coli. In addition to these dynamic changes during chemotherapy, the TIMER (translocation, immunomodulation, metabolism, enzymatic degradation, reduced diversity) model proposed by Alexander and colleagues has outlined how the functions of the microbiome may itself have a central role in determining the extent and intensity of diarrhea. 97 Key to this model is the facilitation of inflammatory responses to chemotherapy by the microbiome. 72
Evidence of Microbial Changes in SM-TKI Treatment
More recently, there has been some direct evidence suggesting links between gut microbial changes and diarrhea following SM-TKI treatments. A preclinical study of the EGFR inhibitor lapatinib showed that lapatinib-treated rats had significantly lowered microbial diversity. 98 In addition, decreases in Betaproteobacteria were seen following lapatinib treatment. In contrast, chemotherapy studies have shown changes in Gammaproteobacteria, and this difference was suggested to be a key difference between chemotherapy- and SM-TKI–induced diarrhea outcomes. 99 A study of 20 patients receiving VEGF-TKI treatment for metastatic renal cell carcinoma (mRCC) assessed the microbiome via 16S sequencing of stool samples. Patients with diarrhea had higher levels of Bacteroides spp and lower levels of Prevotella spp. 18 However, it was inconclusive whether these microbial changes were simply due to the occurrence of diarrhea, or the drivers of this diarrhea.
Probiotics and Fecal Microbiota Transplant
Probiotics and dietary modification have also been suggested as a treatment or preventative measure for cancer treatment–induced diarrhea. In chemotherapy, probiotics have had varying levels of success in reducing diarrhea. 72 While some studies have shown lowered gastrointestinal damage levels and less diarrhea, others have shown no benefit. A meta-analysis recently found insufficient current evidence to support widespread implementation of probiotics after chemotherapy. 100 The authors noted the wide variety in probiotic types and dosing schedules, and stressed the need for rationally designed probiotic mixtures and trials. Probiotics are commonly used alongside some forms of SM-TKI treatment. 101 However, to date, there is no robust evidence for probiotic use during SM-TKI treatment. 64 One study of the EGFR inhibitor dacomitinib in 173 non–small cell lung cancer patients demonstrated that VSL#3 probiotics were unsuccessful in reducing diarrhea or intestinal damage. 102 Subsequent commentary on this article suggested some issues with the study, further highlighting the need for consistently designed probiotic studies.103,104 Currently, a clinical trial is underway to assess the use of probiotic yoghurt in reducing diarrhea following VEGF inhibitor treatment for kidney cancer (NCT02944617). 105 Another form of microbiome modulation under investigation for use in cancer treatment is fecal microbiota transplant (FMT). 106 Preclinically, FMT was able to reduce gut dysbiosis caused by 5-FU. 107 Clinically, a recent study of 21 patients having treatment with VEGFR inhibitors pazopanib and sunitinib for mRCC was completed. 101 Patients with diarrhea received FMT via colonoscopy or Lactobacillus casei DG probiotics as control. After 7 days, all patients in the FMT group had resolution of diarrhea compared with 54.5% of patients in the probiotic group. At a longer term 15- and 30-day follow-up, 90% of FMT patients had no diarrhea compared with 0% of patients in the probiotic group, demonstrating the potential of the microbiome to be a key part of SM-TKI–induced diarrhea.
While there is only a small amount of direct evidence suggesting that gut microbiome changes occurs in SM-TKI treatment, the close relationship of a dysbiotic microbiome with both inflammatory activation and chloride secretion processes is an incentive to further elucidate the use of the microbiome in treating diarrhea from SM-TKI treatments.
Predicting Toxicity and Treatment Response: Role of the Microbiome
In the future, individual microbial composition could be used as a predictor of risk of a range of gastrointestinal conditions. Recent reviews have summarized the initial work that has been done to characterize microbial profiles putting people at severe risk of diarrhea following radiotherapy 72 and how this work is now being translated into the chemotherapy setting. 108 In the past, toxicities have previously been used as an indicator of SM-TKI treatment response, 109 and moving forward, the microbiome may represent a unique opportunity to be able to predict both toxicity and response to treatment.
Aside from diarrhea, the other main side effect from SM-TKI treatment is skin rash. Patients receiving EGFR TKI treatment are at particular risk and may develop secondary skin infections. Multiple studies have suggested a correlation between incidence of rash and subsequent response to treatment, where occurrence of rash was associated with better response.77,110 Commonly, broad-spectrum antibiotics are used to treat this rash. These antibiotics have a deleterious effect on the gut microbiome, and importantly, their use has been shown to be a negative predictor of efficacy and toxicity of EGFR-TKI treatment in non–small cell lung cancer populations. 19 This study retrospectively grouped 102 patients into antibiotic and nonantibiotic-treated groups and found that people who took antibiotics had worse progression-free survival and more instances of severe diarrhea. 19 However, this retrospective study may not take into account the reasons for antibiotic use and whether the results may actually reflect that patients receiving antibiotics were a more vulnerable group overall. In immunotherapy settings, there is a growing link between antibiotic use and treatment response. 111 Similarly, antibiotic use during chemotherapy may also have detrimental effects on treatment efficacy. 20 In addition, chemotherapies including oxaliplatin and cyclophosphamide are reliant on an immune response to induce tumor cell death. A study showed that the antitumor efficacy of cyclophosphamide was reduced in germ-free mice or mice treated with antibiotics. 21 These results suggest that the gut microbiome is integral in shaping an antitumor immune response during both chemotherapy and SM-TKI treatment.
Finally, it has also been shown that occurrence of diarrhea relates to treatment success during SM-TKI treatment. 112 An analysis of 4 phase I trials (total 179 patients) showed that patients who had diarrhea with VEGFR inhibitor sorafenib treatment had a significantly increased time to progression compared with patients who did not develop diarrhea. 113 Another study of 223 patients showed that diarrhea from gefitinib (EGFR inhibitor) treatment was predictive of lowered risk of progression in multivariate analysis, 114 while increased progression-free survival was seen when patients receiving first line VEGF-TKI treatment for mRCC were given antibiotics that gave protection from Bacteroides spp. 115 This is contradictory to the results seen in EGFR-targeted treatment discussed above; and hence, these findings may be target, or antibiotic-specific. Also in mRCC, a small US study of 6 patients showed significant differences in the gut microbiome compositions of responders and nonresponders to sunitinib. 116
Taken together, these findings suggest that levels of diarrhea and antibiotic use could be predictive for a person’s positive and negative responses, respectively, to chemotherapy and SM-TKI treatment. Due to the widespread effects of antibiotics on the gut microbiome, and the proposed role of the microbiome in causing diarrhea in these treatments, future research should focus on connecting gut microbial composition with overall survival and treatment response. It should be noted that a potential drawback of taking a similar research approach is that current research provides evidence for overlapping mechanisms in both toxicity and treatment efficacy. This also suggests that exploiting the gut microbiome to enhance efficacy may lead to increased levels of toxicity. Recent research into microbial changes relating to diarrhea from Crohn’s disease has suggested that microbial dysbiosis drives clinical symptomology, despite a lack of mucosal injury. 117 This suggests that the microbiome is likely to govern the duration of symptoms via mechanisms independent of mucosal injury. As some SM-TKIs do not cause overt tissue injury, this is of potential importance.
Future studies should be careful to determine methods to manipulate the microbiome in a way to minimize toxicity while simultaneously enhancing efficacy. This may be via specialized pre- or probiotics that ensure the production of specific bacterial metabolites, or defined microbial modulation techniques including FMT that could be used prophylactically.
Conclusion
Diarrhea from any cancer treatment can have negative effects on a person’s ability to complete their treatment course, as well as affecting financial welfare and quality of life. Precision treatment and ideally preventative strategies are required to reduce the burden of diarrhea. In this article, we have compared gastrointestinal toxicity stemming from SM-TKI treatment with the more well-understood toxicity seen with traditional, highly mucotoxic chemotherapy treatment, in order to understand key commonalities. Although past research has shown differences in the mechanism of pathogenesis, we hypothesize that the gut microbiome may play a key role in the gastrointestinal response to both treatments. A common mechanism between the 2 would allow for a more rapid development of targeted treatments and prophylactic medications. In addition, as SM-TKIs and chemotherapy are often given in combination, a common way to target this diarrhea would be highly beneficial. Current research in SM-TKI toxicity has focused on the use of interventional treatments to reduce diarrhea severity; however, these interventions may be unable to reduce gut microbial changes and subsequent inflammatory responses. It may, therefore, be advantageous to alter this research direction to focus on how to predict toxicity and treatment efficacy using pretreatment microbiome profiling techniques.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kate R. Secombe is supported by a Lion’s Medical Research Foundation Scholarship.