
Abstract
Keywords
Introduction
Cancer is a major global public health concern and is the second leading cause of mortality in the United States of America. 1 Because of an aging population and population growth, there has been a 33% increase in cancer cases between 2005 and 2015. 2
The World Health Organization statistics provided about 12.7 million cancer cases in 2008, and this number is expected to increase to 21 million by 2030. Cancer patients are challenged with various side effects, including fatigue, chemotherapy-induced pain, and depression, which induce severe impairment in their quality of life (QOL). 3 According to the World Health Organization, one aim of cancer treatment is to considerably prolong the life of patients and ensure QOL for cancer survivors. 4 Complementary therapies have emerged as adjuvant therapies that are able to increase the QOL of cancer patients. In recent times, the use of complementary therapies is much more prominent and popular than previously considered, as an efficacious segment of cancer treatments. 5 Cancer patients use complementary therapies mainly for enhancing the immune system, relieving pain, and controlling adverse side effects caused by the disease or treatment. 6 Complementary therapies contain a broad range of therapeutic approaches. 7 Several studies state that complementary therapies promote the QOL of cancer patients during and after treatment by reducing adverse symptoms.6,8 Recent research has reported that 60% of cancer patients have used at least one type of complementary therapy after being diagnosed with cancer. 8 Furthermore, leading cancer centers in the United States offer evidence-based complementary therapies coupled with conventional medicine, a process known as integrative medicine. 9 In addition, systematic reviews (SR) and meta-analysis (MA) for evaluating the effects of complementary therapies are also increasing. This study, therefore, critically reviews the SR and MA of complementary therapies in cancer patients to appraise the evidence level and provides suggestions for future research and practice.
Methods
Protocol and Registration
The protocol of this review was registered on PROSPERO 2018 (Registration Number: CRD42018090318).
Search Strategy
Two databases, The Cochrane Library and MEDLINE, were searched from their inception through January 2018.
The Cochrane Library
#1 MeSH descriptor: [Neoplasms] explode all trees in Cochrane Reviews
#2 MeSH descriptor: [Complementary Therapies] explode all trees in Cochrane Reviews
#3 #1 and #2 in Cochrane Reviews
MEDLINE
#1 systematic[sb] AND (neoplasms[MeSH] or neoplasm*)
#2 systematic[sb] AND (Complementary Therapies[MeSH] or Complementary Therapie*)
#3 #1 and #2
Study Selection
Types of Participants
All cancer patients treated with complementary therapies were included. There were no restrictions with respect to age, sex, ethnicity, or type of setting.
Types of Interventions
This review included all types of complementary therapies. We classified the interventions according to the guidelines set by the National Center for Complementary and Integrative Health (NCCIH). These were natural products, mind and body practices, and other complementary health approaches. Since acupuncture belongs to 2 groups (mind and body practices and traditional Chinese medicine of other complementary health approaches), we added one more subgroup and classified it separately. Any control that is compared with complementary and alternative therapies is included.
Types of Outcome Measures
QOL, assessed by any validated instrument.
Overall survival, including survival rate or survival time or overall survival, assessed by any validated instrument.
Pain, assessed by any validated instrument.
Depression, assessed by any validated instrument.
Types of Study
SR and MA were included in this study.
Language Restriction
Only articles written in English were included.
Data Extraction and Quality Assessment
Two independent reviewers extracted data using standardized data extraction, and assessed the methodological quality of each included study by applying Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR2). Any discrepancies were resolved by consensus or consultation with a third reviewer. The data extraction form comprised the name of author, publication year, publication country, sample size, study conducted country, search period, study design, type of cancer, interventions, and outcomes.
AMSTAR2 comprises 16 items for assessing the methodological quality of SR. It rates the overall confidence of the review results as high, moderate, low, and critically low. 10 Appraisal is based on the number of critical or noncritical flaws: “critically low,” more than one critical flaw regardless of whether it has noncritical weaknesses; “low,” only one critical flaw regardless of the presence of noncritical weaknesses; “moderate,” more than one noncritical weakness with no critical flaws; and “high,” none or one noncritical weakness.
Results
Study Selection
A total of 601 studies were identified; 32 duplicated studies were deleted. After checking all titles and abstracts, 247 possible relevant studies were retained. After the second screening through full text review, 104 studies were finally selected for analysis (Figure 1).

Flow chart of study selection.
Study Characteristic
Of the 104 studies, 17 studies were published in 2012, and 23 studies were published in 2016 (Table 1). The affiliation country of corresponding author for SR and MA were China (30%), Republic of Korea (15%), the United Kingdom (14%), and the United States (14%) (Table 1). On the other hand, most clinical trials included in the SR and MA were performed in China (48%, 748/1559) and the United States (26.9%, 419/1559) (Table 2). The most researched cancer types included all cancers (56%), followed by studies on breast cancer (25%) Figure 2). In addition, the most studied complementary therapy was acupuncture (21%), followed by herbal medicines (14%) Figure 3).
The Number of Studies by the Year and Lead Authors’ Affiliation a .

Numbers in parentheses represent corresponding authors; those outside parentheses are based on first authors.
Countries Where Clinical Trials of the Included studies Were Conducted.


The cancer types of the included studies.
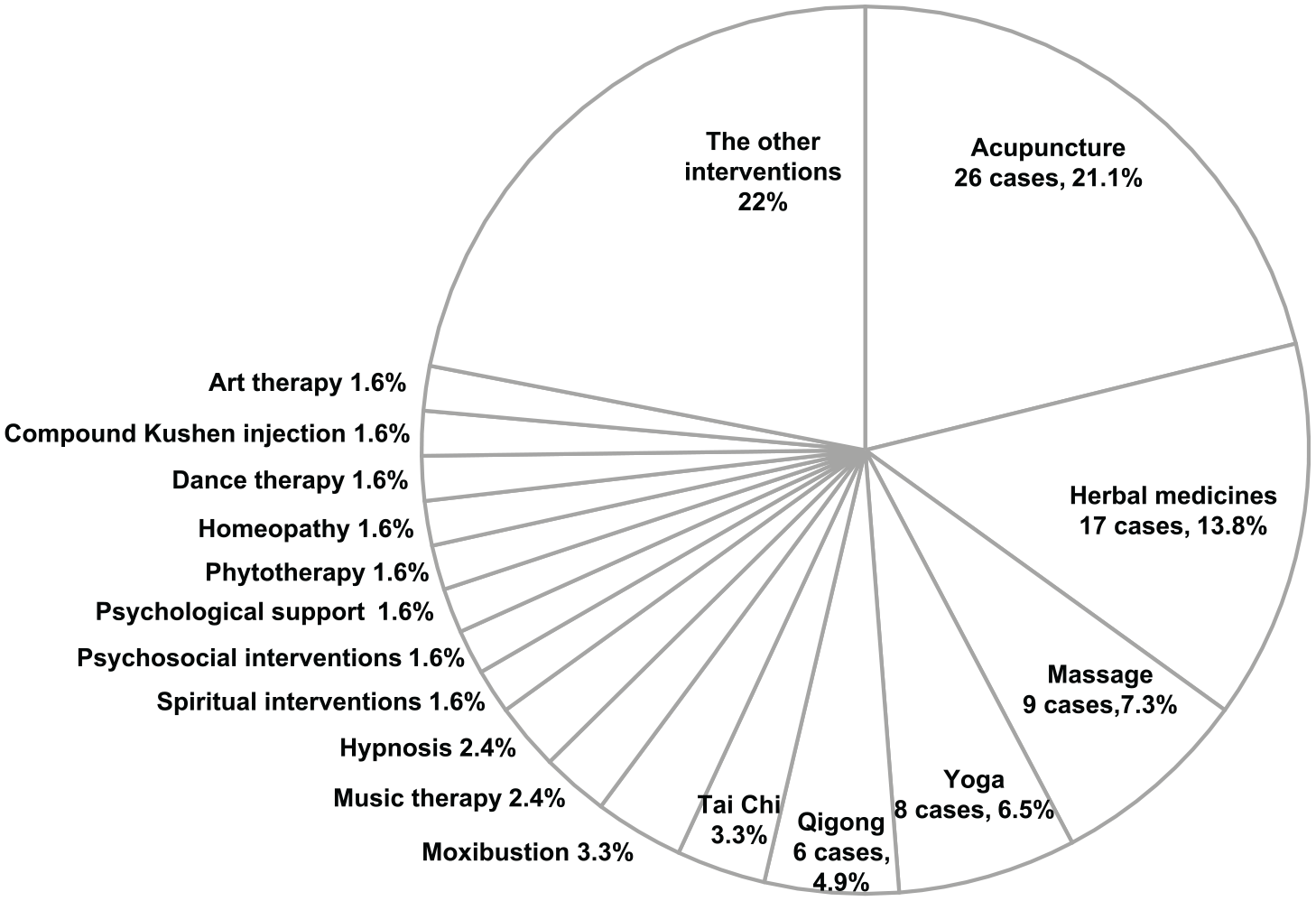
The type of CAM intervention of the included studies.
Methodological and Reporting Quality
Studies were not rated moderate or high confidence if there were more than just one weakness in critical domain and high percentage of studies had difficulty in achieving every critical domain of AMSTAR2 evaluation. As a result, only 17 (16%) studies were rated high. Failure to provide a list of excluded studies (Item 7) was the main reason for being rated critically low. Furthermore, several studies lacked explicit statements of review methods established prior to performing the research, and failed to explain any modifications from previously published protocols (Item 2). Only 23 cases (22.1%) met the requirement of Item 2, and 20 (19.2%) studies provided Item 7.
Confirming noncritical items was relatively easy as compared with critical items, resulting in the absence of moderate grade. Overall, although AMSTAR2 has been simplified, it is more demanding to mark a study as high in methodological quality, as compared with the previous version (Figure 4).
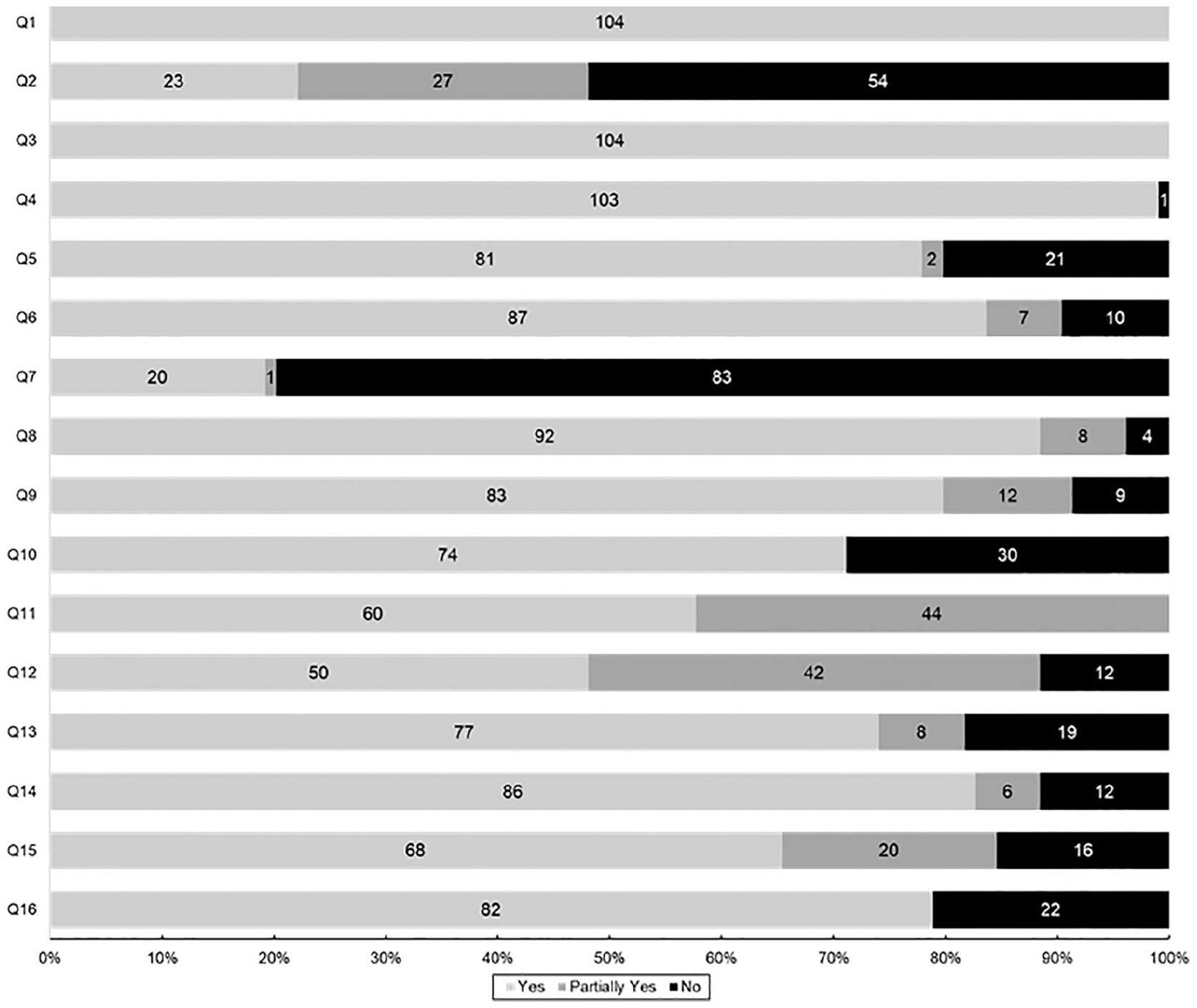
Methodological and reporting quality: evaluation results of each AMSTAR2 question of included studies.
The Items of AMSTAR2 are as Below, and the Bold Items (Q2, 4, 7, 9, 11, 13, 15) are Critical Domains.

Outcomes of Included Studies
Overall, the included SR and MA suggest potential encouraging effects for each outcome. However, the studies also reveal low evidences or low numbers of methodologically rigorous trials. We present below the result of each outcome measurement.
Quality of Life
Systematic review
Among 91 randomized controlled trials (RCTs) and controlled clinical trials (CCTs) in 21 SRs,11-31 58 reported beneficial aspects of complementary therapies on increasing the QOL for cancer patients (64%, 58/91). (Online appendix 1-1).
Meta-analyses
Among 33 MAs in 28 studies,32-59 22 reported significant effects of complementary therapies on increasing the QOL for cancer patients (72%, 24/33). (Online appendix 1-2).
Overall Survival
Systematic review
Meta-analysis
Pain
Systematic review
Meta-analysis
Depression
Systematic review
Meta-analysis
Discussion
This comprehensive review finally included a total of 104 SR and MA of complementary therapies for cancer patients. Considering the increase in number of studies, we could confirm the increased interest in application of complementary therapies for cancer patients.
Most of the SR and MA were published by lead authors affiliated to China, Republic of Korea, the United Kingdom, and the United States. Ironically, approximately 75% clinical trials, including in SR and MA, were performed in China and the United States. The Republic of Korea and the United Kingdom were somewhat lacking in efforts to generate evidence by conducting primary research (ie, clinical studies) and were more focused toward evidence syntheses, as compared with China and the United States.
Meanwhile, we found that complementary therapies were generally applied to all cancers and the most studied complementary therapy was acupuncture. Breast cancer was the most investigated single cancer type. It is assumed that the purpose of complementary therapies for cancer patients is not to eradicate specific cancer cells, but to manage side effects and improve the QOL with the aid of biomedicine.
Similar to our findings, acupuncture (55.3%) was the most frequently provided complementary therapy in a survey of cancer centers across 26 European countries. 87 If the disease was not limited to cancer, the most commonly used complementary therapy was herbal medicine (data collected from SR of surveys) in the United Kingdom, and natural products in the US National Health Interview Survey in 2007.88,89
The methodological and reporting quality of SR and MA were found to be low due to the absence of research protocols and failure to provide the list of excluded studies. Other articles assessed by AMSTAR2 were also rated critically low for similar reasons.90,91 Because there is a limitation for the SR and MA conducted before the AMSTAR2 was published, further studies are required to carefully consider methodology from the protocol stage for being appraised high quality. Conversely, of the 17 methodologically high research studies, yoga (17.6%, 3/17)32,33,84 and herbal medicines (17.6%, 3/17)11,34,92 were most widely studied, and were indicative of bestowing a positive effect on the patients’ QOL. However, several research studies deferred a definitive conclusion due to paucity of high-quality evidence.
Many cancer patients experience one or more adverse side effects during their treatment period; 86% of patients report chemotherapy-associated side effects. 93 Complementary therapies have been used in the management of side effects caused by cancer or cancer treatment. Similarly, the outcomes of included SR and MA reveal that complementary therapies can be effective for improving the QOL and managing side effects of cancer patients.
We acknowledge that there are few limitations to this study. First, in most research on complementary therapies, the definition and scope of complementary therapies remains unclear; hence, it is difficult to set the inclusion/exclusion criteria. We therefore applied the complementary therapies classification of NCCIH. Second, despite every effort to provide a comprehensive and systematic review, language restrictions of our study might have resulted in omission of several studies conducted in Asian or other countries. However, China has published the most articles despite English-language restriction.
Conclusions
In our overview, we found that SR and MA on complementary therapies in cancer patients have increased in China and the United States. Although there are methodological and reporting quality limitations based on AMSTAR2, several complementary therapy interventions were used to manage side effects such as pain, fatigue, and depression in cancer patients. Therefore, future studies must treat the risk of methodological bias with caution. High-quality SR in which selection of high-quality studies is combined with adequate methodology, are needed to clarify the true efficacy of complementary therapies for cancer patients.
Supplemental Material
Appendix_1-1._Quality_of_life_in_SR – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_1-1._Quality_of_life_in_SR for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_1-2._Quality_of_life_in_MA – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_1-2._Quality_of_life_in_MA for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_2-1._Overall_survival_in_SR – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_2-1._Overall_survival_in_SR for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_2-2._Overall_Survival_in_MA – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_2-2._Overall_Survival_in_MA for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_3-1._Pain_in_SR – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_3-1._Pain_in_SR for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_4-1._Depression_in_SR – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_4-1._Depression_in_SR for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Supplemental Material
Appendix_4-2._Depression_in_MA – Supplemental material for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients
Supplemental material, Appendix_4-2._Depression_in_MA for An Overview of Systematic Reviews: Complementary Therapies for Cancer Patients by Seong Min Lee, Ho Cheol Choi and Min Kyung Hyun in Integrative Cancer Therapies
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (Ministry of Science and ICT; No. 2016R1C1B3006806).
Supplemental Material
Supplemental material for this article is available online.
Appendix 1-1. Quality of life in SR
Appendix 1-2. Quality of life in MA
Appendix 2-1. Overall survival in SR
Appendix 2-2. Overall survival in MA
Appendix 3-1. Pain in SR
Appendix 3-2. Pain in MA
Appendix 4-1. Depression in SR
Appendix 4-2. Depression in MA
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.