
Abstract
Traditional Chinese medicine (TCM) herbs are commonly regarded to be safe with minimal toxicities in Chinese communities. Cancer patients who are receiving Western oncology therapy often concurrently take TCM herbs for anticancer and symptom relief purposes. We performed a literature review for current evidence on TCM herb–induced liver injury from an oncological perspective. A literature search on PubMed was performed to identify publications regarding TCM herbs and concoctions with hepatoprotective or hepatotoxic properties. Lists of commonly used herbs and their causality levels were compiled. In view of the wide range of evidence available, cases assessed by the well-established RUCAM (Roussel Uclaf Causality Assessment Method) algorithm were categorized as the highest level of evidence. More than one case of TCM herb–induced liver injury was confirmed by RUCAM in the following herbs and concoctions: Lu Cha (Camellia sinensis), Bai Xian Pi (Dictamnus dasycarpus), Tu San Qi (Gynura segetum), Jin Bu Huan (Lycopodium serratum), He Shou Wu (Polygoni multiflora), Ge Gen (Pueraria lobata), Dan Lu Tong Du tablet, Shou Wu Pian, Xiao Chai Hu Tang, Xiao Yin pill, and Yang Xue Sheng Fa capsule. Finally, TCM with anticancer or symptom relief uses were discussed in detail with regard to their hepatotoxic or hepatoprotective properties.
Keywords
Introduction
Multiple studies have shown that there is widespread use of traditional Chinese medicine (TCM) among Chinese patients as an adjuvant to Western medicine in cancer treatment.1-5 Another study revealed that the self-care of Chinese cancer patients has been heavily influenced by the TCM philosophy. 6 In addition to taking herbal medicines prescribed by Chinese medicine practitioners, it is also common for the general public to use proprietary Chinese medicine on their own or add herbs to meals and soups. A study found that over half of the Hong Kong cancer patients surveyed used at least one form of TCM. Furthermore, 60% of these patients who were receiving chemotherapy concurrently used TCM. 7 According to a Taiwanese survey, 69% of respondents thought that TCM is mild and has no ill effects at all. 8 TCM herbs and concoctions, like any drug, also have side effects and toxicities.
Many oncologists do not encourage the concurrent use of TCM due to the potential of having adverse interactions between Chinese and Western drugs that may lead to hepatotoxicity. There have been numerous reports of liver injury caused by TCM herbs and concoctions. However, the establishment of causality varies in these reports. A typical example of TCM-induced liver toxicity is He Shou Wu, which is a popular herb for preventing hair loss and aging. A study found that only 30.6% of literature case reports demonstrate a high probability of He Shou Wu–induced liver injury causality. 9 The causality between TCMs and drug-induced liver injury was ascertained by various methods, such as by patient recall, clinical suspicion, exclusion, and algorithms. It is important to note the complexity and difficulty in establishing causality for TCM herbs. One difficulty is due to polypharmacy as TCM is rarely used as a single herb, and TCM may sometimes be used concomitantly with Western drugs. Another difficulty is contamination by heavy metals. 10 Evidence available in case reports, case series, and reviews may not be complete. If these confounders are not excluded, misdiagnosis and overreporting may occur.
Hence, there is a need to categorize the cases in the existing literature into different evidence levels of causality. Focus should be given to hepatotoxic TCM for which clear evidence has been demonstrated by standardized causality assessment algorithms. RUCAM (Roussel Uclaf Causality Assessment Method), or its previous synonym CIOMS (Council for International Organizations of Medical Sciences), is the most commonly used causality instrument for drug-induced liver toxicity. 11 RUCAM is used to assess causality quantitatively, by applying numerical weighting to key features such as chronology and risk factors, and it generates an overall score to indicate the probability of causality. The RUCAM scale ranges as follows: 0, excluded; 1 to 2, unlikely; 3 to 5, possible; 6 to 8, probable; and ≥9, highly probable. 12
Furthermore, not all TCM herbs and concoctions cause hepatotoxicity. In fact, some of them have hepatoprotective effects against drug-induced liver injury, such as chemotherapy-induced hepatotoxicity.
In this article, we present a review of the current literature to identify potentially hepatotoxic or hepatoprotective TCM that cancer patients may concurrently use with Western systemic therapies, and stratify them using causality levels to offer easier interpretation.
Methodology
Data Sources and Searches
We carried out a systematic search of the PubMed database on March 11, 2019, to identify publications of laboratory findings, case reports, case series, and review articles of TCM-induced hepatotoxicity. By using Medical Subject Headings, English articles that were associated with the terms “Chemical and Drug-Induced Liver Injury” and “Medicine, Chinese Traditional” were selectively included. Our search yielded 64 results.
Exclusion of Publications
Publications were excluded by the following criteria. Publications were excluded if
They were unrelated to TCM-induced hepatotoxicity or hepatoprotection, or
Access to the full article could not be obtained, or
No specific TCM herbs or concoctions were named, or
No significant results were directly shown with specific TCM herbs or concoctions.
As a result, 14 publications were excluded from this review.
Data Analysis
Data Extraction
Fifty publications were analyzed. Individual herbs and herbal concoctions were identified. The scientific names of each herb and its corresponding Chinese name were determined. As a single TCM herb could have different scientific names (eg, Polygoni multiflori vs Polygonum multiflorum Thunb), results were grouped according to the Chinese name of the herb. The publications were then analyzed to yield the number of clinical cases and causality.
Duplication of Data
The references of these 50 publications were carefully inspected. There were case reports, case series, and reviews referring to the same event of hepatotoxicity caused by a certain TCM herb or concoction. In particular, 3 systematic reviews were published by the same author in 3 consecutive years, and each systematic review cited cases from the previous review. Duplicated data were discarded in this review.
Exclusion of TCM Herbs or Concoctions
If the publication failed to provide any of the aforementioned data (eg, number of cases), the reference lists of the primary and review articles were scanned. If the primary source could not be accessed, the data of the individual herb or concoction were also excluded.
Levels of Causality
Hepatotoxic herbs or concoctions
In view of the wide range of clinical causality ascertainment methods in the literature, as well as the fact that laboratory findings do not directly infer clinical significance, a stratified level of causality was devised in order to provide a clearer and more clinically oriented picture.
Entries of hepatotoxic herbs or herbal concoctions found from the publications were categorized into 1 of the 4 following levels according to the following description:

Hepatoprotective herbs or concoctions
After excluding uncommonly used hepatoprotective herbs and herbal concoctions, only nonclinical ones remained; hence, they were not graded by causality levels.
Results
Lists of herbs and concoctions that were hepatotoxic or hepatoprotective, their respective causality levels, and number of cases are compiled in Tables 1 to 5.9,13-46
TCM Herbs That Were Assessed by RUCAM to Demonstrate Clear Causality of Hepatotoxicity.

Abbreviations: TCM, traditional Chinese medicine; RUCAM, Roussel Uclaf Causality Assessment Method.
TCM Concoctions That Were Assessed by RUCAM to Demonstrate Clear Causality of Hepatotoxicity.

Abbreviations: TCM, traditional Chinese medicine; RUCAM, Roussel Uclaf Causality Assessment Method.
Single Herbs With Hepatotoxic Risks.

Herb Concoctions With Hepatotoxic Risks.

TCM Herbs Found to Have Hepatotoxic Properties in the Laboratory Setting.
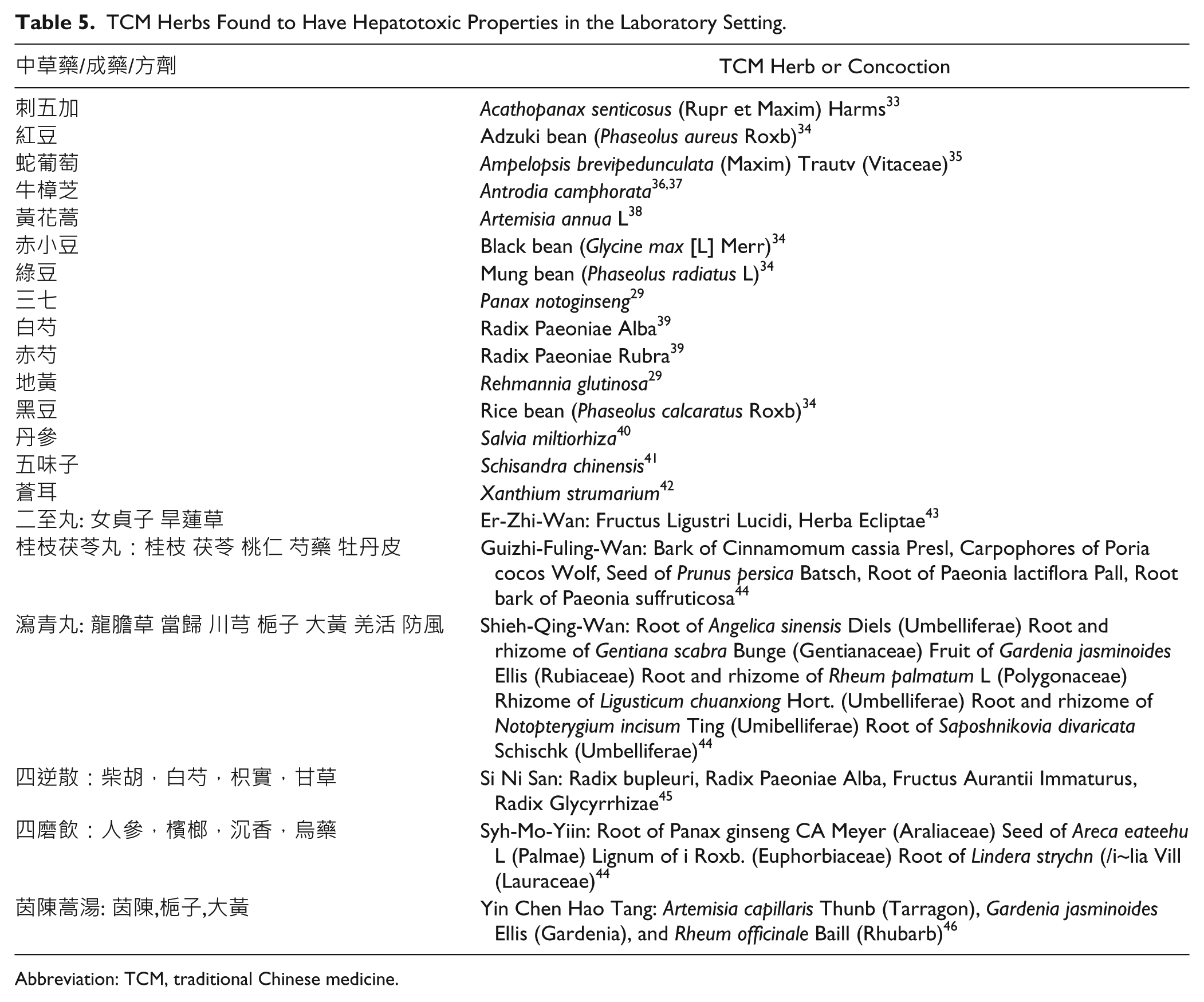
Abbreviation: TCM, traditional Chinese medicine.
We found 20, 17, 34, and 27 individual herbs that were graded level 4, 3, 2, and 1 for their causality toward liver injury, respectively. For herbal concoctions, we found 6, 10, 7, and 2 concoctions that were graded level 4, 3, 2, and 1, respectively. There were in total 21 herbs or concoctions that were hepatoprotective in laboratory settings. Using RUCAM, clear causality (level 4) was established in 194 cases of TCM-induced liver toxicity.
Discussion
TCM for Symptom Relief and Body Enhancement
He Shou Wu (何首烏, Polygoni multiflori) is traditionally used for treating premature whitening of hair, dizziness, and insomnia due to the insufficiency of essence and blood. 47 This makes He Shou Wu a popular choice among cancer patients to counter the side effects of chemotherapy such as alopecia. According to our results, there were 80 cases reaching level 4 (clearly established causality), 147 cases reaching level 3 (possible causality), and 516 cases attaining level 2 (clinical suspicion). Furthermore, when He Shou Wu was coadministered with other drugs as herbal concoctions, there were 37 cases that reached level 4. Therefore, there was clear evidence that He Shou Wu could cause liver injury.
In TCM, Chuan Lian Zi (川楝子, Melia toosendan) is used for relieving pain, 48 and it is often used by cancer patients for pain control and to “relieve liver Qi congestion,” which is common among breast and liver cancer patients according to TCM theory. However, Chuan Lian Zi is known to have a slightly toxic property. 49 Our search results in a case (level 4) of Chuan Lian Zi–induced liver injury.
Ren Shen (人參, Panax ginseng) has gained popularity in recent years. The annual world ginseng production was estimated to be 80 080 tons, and its global consumption has risen steadily over the years. Ginseng is being marketed as a natural health food and various forms are available. 50 Cancer patients take Ren Shen prepared in the form of tea, capsules, or as an ingredient in soup in the hope of increasing their “inner resistance.” 6 Ren Shen could be used for restoring Qi. It can treat severe vomiting, fatigue, diarrhea, shortness of breath, fatigue, feeble pulse, extreme weakness after severe disease, or prolonged illness. 47 During chemotherapy, patients might experience the above symptoms and may use this herb. Our review found a case of possible (level 3) hepatotoxicity caused by intravenous wild ginseng pharmacopuncture and 6 cases of suspected liver injury (level 2) caused by Ren Shen. Hence, further research should be done to confirm the causality of liver injury caused by this popular herb.
San Qi (三七, Panax notoginseng) is a herb used to arrest bleeding and remove blood stasis in TCM. It is also known to be helpful in reducing swelling and relieving pain. 48 Hence, this herb might be used to reduce the pain caused by the tumor. According to laboratory findings, it was suggested that it has hepatoprotective effects. Unfortunately, another similarly named herb named Tu San Qi (土三七), or Radix Gynurae Segeti, has been proven to induce hepatic sinusoidal obstruction syndrome/veno-occlusive disease. 51 Contrary to the hepatoprotective San Qi, Tu San Qi led to 4 cases of liver injury (level 4). Hence, caution must be taken to avoid misidentification.
Chai Hu (柴胡, Bupleurum falcatum) is an important component in Xiao Chai Hu Tang (小柴胡湯; XCHT). XCHT is a commonly used concoction to treat Shaoyang disease with symptoms such as chills and fever, nausea and dizziness, restlessness, fullness, discomfort at the chest, and dry throat. 48 Cancer patients may experience neutropenic fever, and XCHT is a common folk remedy that might be taken. Our results found that there were 4 cases of XCHT reaching level 4, while Chai Hu had 28 cases reaching level 2. On the other hand, Si Ni San, a concoction containing Chai Hu, is used to treat chronic hepatitis. 48 Si Ni San was found to be hepatoprotective in laboratory settings. We hypothesize that this could be due to the interaction between different herbs in concoctions. When herbs containing hepatotoxic constituents are boiled with other herbs, it is possible that new compounds that are nonhepatotoxic are formed.
Another herb that showed conflicting results was Yin Chen Hao (茵陳蒿, Artemisia capillaris). Our literature search found that this herb causes liver injury, with 1 case of level 4 and 7 cases of level 2. On the contrary, Yin Chen Hao is used to treat jaundice in TCM. Oncology patients may take this herb to reduce jaundice. A concoction that uses Yin Chen Hao as a major herb, named Yin Chen Hao Tang (茵陳蒿湯), is also used for treating jaundice and diseases such as acute infectious icterohepatitis, acute cholecystitis, cholelithiasis, and leptospirosis in TCM. Our literature search found that laboratory findings suggesting Yin Chen Hao Tang has hepatoprotective properties. We postulate that as TCM herbs are rarely prescribed as a single herb, the other herbs that are prescribed concurrently may mitigate the hepatotoxic effects of Yin Chen Hao. Thus, in the form of a concoction, Yin Chen Hao Tang demonstrates hepatoprotective properties.
Wu Wei Zi (五味子, Schisandra chinensis) is found to be hepatoprotective in our literature search. It is also known to be effective in lowering transaminase levels in those suffering from chronic hepatitis. 48 Hence, this herb may be taken by cancer patients to reduce the liver toxicity of systemic therapies and improve their liver function.
Bai Shao (白芍, Radix Paeoniae Alba) is known to nourish the liver and treat diarrhea, dysentery, and pain. 48 This herb may be taken by cancer patients in hopes of improving their liver function. The results of our review echoed with its TCM use, as it was found to have hepatoprotective properties in the laboratory setting.
TCM With Anticancer Properties
Bai Xian Pi (白鮮皮, Dictamus dasycarpus) has been found to contain chemical constituents with cytotoxic properties. 52 One study showed the inhibitory effect of one of its chemical constituents on human breast cancer cells. Thus, it may be prescribed by TCM practitioners to patients for anticancer purposes. 53 However, our review found that Bai Xian Pi could cause hepatotoxicity, which could probably be explained by its cytotoxic properties. We found 7 and 32 cases that reached level 4 and 3, respectively.
An interesting finding was Camellia sinensis (綠茶), commonly known as green tea, had 28 cases reaching level 4. In contrast, previous research has shown that green tea extract has antioxidant and antihepatotoxic properties. 54 Green tea was also reported to have anticancer properties. A review suggested green tea has anti–breast cancer activity by adjusting cell signaling pathways. 55 Its seeds were also found to have inhibitory effects on human ovarian cancer cells. 56 An extract also showed inhibitory effects on the growth of colorectal cancer cells. 57 We hypothesize that while there are certain chemical constituents that may be beneficial to health, green tea may also contain hepatotoxic constituents and may lead to liver injury when taken in large quantities.
Huang Yao Zi (黃藥子, Dioscorea bulbifera L) is traditionally used to treat goiter, hyperthyroidism, and tumors, 48 and it could be prescribed to patients with thyroid cancer. However, it is known that overdose or long-term usage could lead to liver damage. 58 Surprisingly, no clinical cases of related hepatotoxicity were found in our literature search, only laboratory findings showed the potential of liver injury caused by this herb. This could be explained by the decreasing popularity and cautious use of this herb in clinical TCM practice nowadays.
Our review found 1 case of Huang Qin (黃芩Scutellaria baicalnsis) that reached level 3 and 22 cases of level 2. This potentially hepatotoxic herb has been found to have anticancer properties, its chemical constituents were found to be cytotoxic to a broad range of human cancer cells, including brain tumor, 59 prostate cancer, 60 head and neck squamous cell carcinoma, 61 acute lymphocytic leukemia, lymphoma, and myeloma cell lines. 62
Topoisomerase inhibitors, like irinotecan and topotecan, are a type of chemotherapeutic agents that were derived from camptothecin from the bark of Camptotheca acuminata (Xishu, 喜樹). This TCM herb was found to reach level 2 of hepatotoxicity causality.
Causality Assessment
As demonstrated in the tables above, there are varying levels of evidence in the current literature. However, the clinical and histopathological features of herb-induced liver toxicity may mimic any liver injury histopathological model, 63 and expert judgement could be limited by subjectivity. Hence, a widely accepted and standardized algorithm is needed to confirm causality. RUCAM is a quantitative scale that has been used worldwide,17,64-66 allowing results to be comparable across countries. When compared with other general causality assessment algorithms like the Naranjo scale, it is more liver-specific and more relevant. 12 Among liver-oriented methods, RUCAM was found to be superior. Clinical Diagnostic Scale showed poorer discriminative power, whereas the Digestive Disease Week-Japan scale included an in vitro drug lymphocyte stimulation test evaluation criterion, which was not widely accessible. 67 RUCAM also addresses other alternative causes of liver injury like concomitant drug use. Therefore, RUCAM is by far the most preferred algorithm used in the field.
Future Implications
First of all, we should note the presence of different types of evidence in the literature. Without following established causality algorithms, problems like comedication and poor data quality may affect the establishment of causality; hence, it is unjustifiable to ascertain the causal relationship immediately. Furthermore, contaminants during production and processing may lead to liver injury. Hence, clear-cut causality is often difficult to achieve. Our review presented the stratification of causality of the current literature. RUCAM is an important tool that should be applied to all future cases to determine causality accurately. Further studies are needed to confirm the causality of herb-induced liver injury with RUCAM in order to clarify the hepatotoxicity of herbs that are suspected in the literature. The use of RUCAM should be encouraged among physicians to aid diagnosis, and RUCAM should be employed before publication of cases and inclusion in databases.
In Chinese communities, there is a common misconception that TCM is free of side effects and toxicities. Our review highlights the importance to evaluate the potential hepatotoxicity of TCM. We suggest that there is a fundamental need for raising the awareness of this issue among Chinese communities. Cancer patients should consult TCM practitioners before using TCM, instead of taking TCM without professional advice.
Also, TCM can have hepatoprotective effects. However, proving the hepatoprotective effects of a herb clinically can be challenging, and the therapeutic benefit of TCM is often questioned. TCM herbs are rarely used alone, as each patient receives a personally tailored concoction. Hence, the effectiveness of TCM is difficult to be proven in the Western-dominated setting based on a medical system that treats the same disease with the same drug on different patients.
In practice, oncologists are often uncertain of the efficacy and safety of TCM and therefore urge patients not to take any TCM during systemic treatment. TCM has been practiced for over 2000 years, and its ideologies and effectiveness have been deeply rooted and accepted in Chinese communities. A survey done in Hong Kong found that over two thirds of all interviewed Chinese cancer patients believed that integrated TCM and Western medicine was effective in treating cancer. 7 Hence, Chinese cancer patients are keen to use TCM. The total rejection by some oncologists may prompt patients to hide the truth. The aforementioned survey found that among patients who were concurrently receiving Western medicine treatment and TCM, nearly two thirds of them did not inform their physicians. This is not only harmful to the doctor-patient relationship but also unhelpful in monitoring and treating the patient.
Recent research has shown that certain TCM when used in combination with Western medicine can be beneficial. It was found that some TCM could act as effective chemosensitizers and radiosensitizers, and could be helpful in palliative care. 68 We have learnt from history that some modern anticancer drugs were derived from plants. The Pacific Yew, the Madagascar Periwinkle, and the Chinese happy tree have yielded valuable chemicals for chemotherapy. If TCM was excluded from treating cancer patients, the advancement of cancer therapy may be hindered. More research is needed to clarify the hepatotoxicity and hepatoprotectiveness of different TCM herbs and concoctions. This is crucial to aid TCM practitioners and Western medicine doctors in making clinical decisions, as well as paving the way for TCM and Western medicine integration in treating cancer.
Conclusion
This literature review compiled a list of hepatotoxic and hepatoprotective TCM herbs and concoctions, and highlighted some that are highly likely to be used by cancer patients as they either have anticancer properties or symptom relief purposes. They were then stratified according to their levels of causality, to provide a clearer and more clinically relevant picture of the current evidence. More stringent research with the use of RUCAM is needed to confirm the causality of herb-induced liver injury before publication and inclusion in databases. Cancer patients should note the potential hepatotoxic effects of TCM herbs and should not assume the absence of side effects of TCM herbs. More collaboration between TCM and Western medicine should be encouraged to establish effective and safe screening of drug-herb interaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.