
Abstract
Background
Kuan-Sin-Yin (KSY) is a traditional Chinese medicine (TCM) decoction, which has been shown to have cytostatic effects on cancer cells and involved in the TCM theory of promoting yin-yang balance.Sonce many cancer patients suffer from autonomic dysfunction (AD), which correspond to yin-yang imbalance in TCM. The aim of this study is to evaluate the possible effect of KSY in metastatic colon cancer (mCRC) patients with AD.
Methods
We conducted a single-group experiment. Total 52 qualified patients were enrolled. Participants took the KSY daily for 2 weeks. The primary outcome was KSY efficacy as reflected in the heart rate variability (HRV) and electrical conductivity (µA) over 12 meridian points. Autonomic function was examined before and after the KSY intervention. The vagal and sympathetic tone were recorded by HRV; 12 meridian energies were measured using a meridian energy analysis device. Secondary outcomes were cancer-related symptoms and patient quality of life (QoL).
Results
The results showed that the KSY intervention improved AD via increasing the vagal tone (HF: P = .041), but not the sympathetic tone (LF: P = .154); total autonomic activity was significantly enhanced (HRV activity: P = .013). Intriguingly, energy increased more over the yin meridian (P = .010) than over the yang meridian (P = .015). Cancer-related symptoms and QoL were significantly improved (P < .05).
Conclusion
The safety and effectiveness of KSY in improving AD in mCRC patients are through regulating the vagal-sympathetic dynamic balance, which correspond to the TCM yin-yang concept of energy.
Keywords
Introduction
In recent decades, cancer has become one of the most important health issues because of its high prevalence and the associated death rate. Beyond the standard Western options of chemotherapy and target therapy, more and more natural compounds and traditional Chinese medicine (TCM) treatments have been accepted as a part of cancer treatment. TCM may enhance the physical energy (qi) and has a positive effect on organ function. Many cancer patients suffer from autonomic dysfunction (AD), a disturbance in the organ function regulated by the vagal and sympathetic nerve systems, a condition that corresponds to the TCM concept of an imbalance in the yin and yang energy forces within the human body. Studies have found AD to be highly prevalent in patients with advanced cancer, and it is associated with the worsening of fatigue and related symptoms as well as poor survival. 1 The autonomic nervous system (ANS) controls the blood vessels, airways, intestines, and cardiovascular system and is mostly under involuntary control. It regulates and coordinates bodily functions through glandular activity and the contraction and relaxation of smooth and cardiac muscles. 2 Many studies have shown that AD in advanced cancer, whether in the cardiovascular, digestive, or endocrine system, leads to lower quality of life (QoL).3,4 The TCM decoction Kuan-Sin-Yin (KSY) has been proved to be safe and effective in upregulating the qi energy and improving QoL in cancer patients.5,6 The design of KSY is based on the classic decoction si jun zi tang, which has been used in TCM for thousands years with the effect of qi promotion and immunity enhancement.7,8 In regard to the composition of the KSY, it is a TCM decoction that is composed of 7 herbs in a specified ratio (Codonopsis pilosula 6 g; Atractylodes macrocephala 6 g; Glycyrrhiza uralensis 3 g; Poria cocos 6 g; Astragalus membranaceus 6 g; Ligustrum lucidum 3 g; and Agastache rugosa 6 g; net weight of 36 g of herbal medicine was extracted with 100 mL water in each pack). All herbs were soaked in water at a ratio of 1:3 (g:mL) and subsequently boiled at 1.5 atm,120°C, for 4 hours using an automatic Chinese herb boiling machine.5,9 We are intrigued by the effect of KSY on AD in cancer patients. Because the serum levels and tumor markers of biochemistry cannot represent the activity or balance of the autonomic system, we chose alternative tools to measure heart rate variability (HRV) and skin conductivity over specific acupoints to evalulate the effect of KSY on AD. The relevance of skin conductivity in AD was based on Ryodoraku theory.10,11 There are also some studies measuring the correlation of electroconductivity and the disease.12,13 According to a previous study, the skin conductivity measured by the meridian energy analysis device (MEAD) provides both reliable and significant results for analysis of the meridian energy and the index of the vagal-sympathetic balance; the reproducibility of the device is 93.2%. 10 Therefore, we checked the changes in the electrical conductivity to compare the severity of AD in patients.
Recent research has shown that HRV has good specificity and positive predictive value for the diagnosis of AD and can be used as a reliable diagnostic method in cancer patients. 14 Chien et al 15 also demonstrated that electrical skin conductivity may reflect the activity of the ANS, in concordance with the TCM meridian theory.
Patients’ self-reported QoL and cancer-related symptoms were also investigated in the study. The study was focused on patients with metastatic colon cancer (mCRC), a homogeneous group of individuals who received similar chemotherapy treatment. The study involved an intervention and measurements that were noninvasive, safe, and inexpensive. In this study, the TCM concept of keeping the physical function in hormony and elevating the meridian energy (qi) corresponded well with the Western notion of regulating the vagus/sympathetic nerve tone to treat AD.
Objectives and Hypotheses
In this study, HRV physiological parameters and meridian energy (qi) levels reflected in skin conductivity were measured across 2 weeks of KSY use in mCRC patients to objectively evaluate the effects of KSY on AD. We hypothesized that, after controlling for cancer type, disease status, and related chemotherapy regimens, significant differences in HRV parameters and skin conductivity before and after the KSY intervention would identify the improvements in AD and qi meridian energy levels.
Materials and Methods
Research Design and Participants
An experimental clinical research design was applied in this study. With the cooperation of the Chinese Medical and Oncology Department, the attending physicians, including TCM doctors and oncologists, assigned the participants to supervise interventions. The inclusion criteria were as follows: (1) cancer pathology confirmed with mCRC; (2) patients with Eastern Cooperative Oncology Group (ECOG) performance scores ≤2 and 20 to 75 years old; (3) patients who sufferred from more than 4 of 9 symptoms graded more than 1, identified as having at least moderate AD (we meaured 9 cancer-related and AD symptoms using the Common Terminology Criteria for Adverse Events [CTCAE] criteria, as shown in Table 1); (4) participants who completed chemotherapy with an oxaliplatin- or irinotecan-based regimen within the past 6 months and with at least moderate AD and cancer-related symptoms; (5) all participants who were able to understand the purpose and process of this study and signed the informed consent form.
Comparison of Cancer-Related Symptoms Before and After Kuan-Sin-Yin Intervention (n = 52). a

Abbreviations: CTCAE, Common Terminology Criteria for Adverse Events (grading: 0-4); ECOG, Eastern Cooperative Oncology Group.
Grade 0, no symptoms; grade 1, mild symptoms; grade 2, symptomatic and medical intervention or minor cauterization indicated; grade 3, severe symptoms, daily-life function disability; grade 4, life-threatening adverse event. *P < .05; **P ≤ .001; *** P ≤ .0001 with statistical significance.
Patients meeting the following criteria were excluded: (1) terminal disease or life expectancy <3 months; (2) presence of psychiatric problems; (3) completion of the chemotherapy treatment course; (4) development of a major event (operation, acute myocardial infarction, severe infection such as pneumonia, or under ventilator use) causing withdrawal from the study; or (5) any other condition the physician-in-charge deemed would make the patient unsuitable for the study.
All participants were given the TCM decoction KSY (100 cc) every day after breakfast to relieve their AD and cancer-related symptoms for 2 weeks after the chemotherapy. The study protocol and design were reviewed and approved by the Taipei City Hospital Institutional Review Board (reference number: TCHIRB-1020127-E) and then implemented from July 2013 to December 2014 in Lin-Sen Branch, Taipei City Hospital. Verbal and written informed consent were obtained from all participants after they were informed of the study design, intervention, data collection, and the rights of participants. Figure 1 shows the flowchart of the research design and participant enrollment in this study.

Study flowchart.
Intervention
The TCM decoction KSY we used in this study was designed to enhance the qi meridian energy, which may regulate the autonomic function.
Quality Control and Safety of KSY
The KSY contained 7 Chinese herbs (Codonopsis pilosula, Atractylodes macrocephala, Poria cocos, Astragalus membranaceus, Agastache rugosa, Ligustrum lucidum, and Glycyrrhiza uralensis). Each of the components has been shown to have pharmacological activity in modulating the immune system and to have anti-inflammatory or antioxidant properties or both.16-22 The purity of the KSY was evaluated by screening ingredients for contamination by heavy metals and pesticides and by a microbial limit test. Standard contents and quality control were analyzed by Internal Transcribed Space (ITS) technology and high-performance liquid chromatography (HPLC) at the Industrial Technology Research Institute, Hsinchu, Taiwan.We used ITS to analyze each of the 7 component ingredients in KSY to establish their DNA sequence, then analyzed the final KSY decoction using HPLC-PCA.
23
ITS is a well-developed DNA technology used to authenticate Chinese herbal ingredients; it analyzes a piece of nonfunctional
Because KSY has been shown to safely suppress tumor growth in vivo and in vitro, 9 we used KSY in mCRC patients to observe the effect on AD.
Measurements and Study Settings
The primary outcomes were the efficacy of KSY as reflected in HRV parameters and electrical conductivity over 12 meridians. The secondary outcomes were improvements in cancer-related symptoms and QoL measurements after the KSY intervention. Because this is a pragmatic study, in the real world, patients may have some belief (or disbelief) of the benefit of TCM in relieving their cancer-related symptoms. However, except for the self-reported QoL assessment, the HRV and meridian energy measurement along with the cancer-related symptom grading (according to CTCAE) were recorded by an assistant who was not otherwise involved in the study. to minimize the bias.
Measurements of HRV and electrical conductivity (meridian energy, qi) were done by a well-trained technician before and after the participants received KSY treatment for 2 weeks. Both procedures were done with participants lying down, after a 15-minute rest, and in a quiet room with a constant temperature of 25°C and humidity of 55%. Self-report of cancer-related symptoms and the QoL questionaire were also administered before and after the KSY intervention.
Analysis of Heart Rate Variability
For each participant, both frequency-domain and time-domain HRV were measured according to the Task Force of the ESC and NASPE using the ANSWatch analysis system 26 (Figure 2). The following HRV parameters were calculated as hourly values: standard deviation of adjacent peak-to-peak intervals (SDNN), which reflect the total ANS activity index (ms), and square root of the mean of the sum of the squares of differences between adjacent peak-to-peak intervals (RMMSD). The power spectra of peak-to-peak intervals were obtained by means of fast Fourier transformation (Taiwan Scientific Corporation, Shin-Dian City, Taipei 231, Taiwan). The zero-frequency component was excluded before the calculation of powers. The area under the curve of the spectral peaks within the ranges of 0.01 to 0.4 Hz, 0.01 to 0.04 Hz, 0.04 to 0.15 Hz, and 0.15 to 0.4 Hz were defined as the total power (TP), very-low-frequency power (VLF), low-frequency power (LF), and high-frequency power (HF), respectively. The HF was used as the index of vagal tone and the LF as the index of sympathetic and vagal modulation; LF/HF was the index of sympathetic-vagal balance. 27

ANSWatch wrist monitor.
The accuracy of the ANS monitor was represented by the correlation between the HRV parameters and electrocardiogram results. 28 The findings of Fadul et al 29 suggest that HRV may provide a useful measure of AD in advanced cancer patients.
Meridian Energy
We checked the electrical conductivity in the 12 modified Yuan (source) acupoints over 12 meridians with a MEAD (MedPex, Taipei, Taiwan; Figure 3). The 12 modified Yuan source acupoints are near the wrist or ankle joins of the 4 extremities and may represent the vital energy of the 12 meridians (6 yin and 6 yang meridians) and the correponding organs (Figures 4A-4D). TCM uses the 12 modified yuan (source) points to treat diseases of the internal organs. MEAD has been shown in other clinical studies to provide both reliable and significant results for analysis of the meridian energy and the index of the vagal-sympathetic balance.6,15,30,31 The measurements were started with very low current and gradually increased to a maximum value of 200 µA. Recordings of the electrical conductivity of the meridians were entered directly into a computerized system. The conductivity values were calculated with voltage supplied by the device and currents measured in meridians and were expressed on a scale from 0 (zero conductivity) to 100 (maximum conductivity). The conductivity value of the 12 modified yuan (source) acupoints and the mean value of the yin/yang meridian of each patient were calculated once at each time point (before and after intervention).

Meridian energy analysis device (MEAD).

A. Acupoints in the yin meridian of the hand. B. Acupoints in the yin meridian of the foot. C. Acupoints in the yang meridian of the hand. D. Acupoints in the yang meridian of the foot.
Cancer-Related Symptoms and QoL
Cancer-related symptoms were graded using the Common Terminology Criteria for Adverse Events (CTCAE) Scale, a tool commonly used in clinical evalulation of the grade of cancer-related symptoms. 32 We also had participtants fill out 2 QoL questionaires: the Brief World Health Organization Quality of Life Questionnaire (WHO-BREF) and the 12-Item Short Form Health Survey (SF-12).33,34
Statistical Analysis
The data were analyzed using IBM SPSS 19.0 for Windows (IBM Corp, Endicott, NY). Demographic details and clinical variables were summarized using descriptive statistics. The results of HRV with distribution plot were calculated by MedCalc software version 15.2.
A paired-t and nonparametric 2-sample t test with Wilcoxon signed-rank test were used to compare the differences before and after the KSY intervention in HRV and meridian energy, cancer-related symptoms, and QoL. The statistical hypothesis tests were set with a significance level of .05.
Results
Participant Characteristics
After assessment for eligibility, 52 mCRC patients were included in the study. Table 2 shows the demographic characteristics of the participants. Their mean age was 51.42 years. All were well educated and communicated well, with ECOG scores ≤2.
Characteristics of the Participants (n = 52).

Abbreviations: SD, standard deviation; ECOG, Eastern Cooperative Oncology Group.
The Effect of KSY on HRV Parameters
Table 3 and Figure 5 show the analysis of HRV parameters before and after the KSY intervention. The nonsignificant P value of the test pressure (P = .154) indicates the stability of the HRV test before and after the intervention. We noted a significant increase in HF (P = .041), SDNN (indicating HRV activity; P = .013), RMMSD (P = .029), but no significant changes in TP, LF, or sympathetic-vagal balance (LF/HF) indexes. Even though both the vagal tone (HF) and sympathetic tone (LF) increased, the level of increase for the LF (P = .154) was less than for the HF (P = .041), so that the sympathetic-vagal index (LF/HF) did not change significantly. KSY had much greater effect on vagal tone than on sympathetic/vagal tone in this study.
Comparison of HRV and Electrical Conductivity Before and After the Kuan-Sin-Yin Intervention (n = 52). a

Abbreviations: HRV, heart rate variability; SEM, standard error of the mean; SDNN, standard deviation of adjacent peak-to-peak (NN) intervals; LF%, low-frequency component normalized; HF%, high-frequency component normalized; LF/HF, sympathetic nerve/parasympathetic nerve balance; VLF, very-low-frequency power; RMMSD, square root of the mean of the sum of the squares of differences between adjacent NN intervals; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Total power: variance of NN intervals in FFT analysis (ms2). LF: 0.04 to 0.15 Hz (ms2; measure of sympathetic function). HF: 0.15 to 0.4 Hz (ms2; measure of parasympathetic function). Variance: square of standard deviation of 5-minute NN intervals (ms2).b P < .05 with statistical significance.
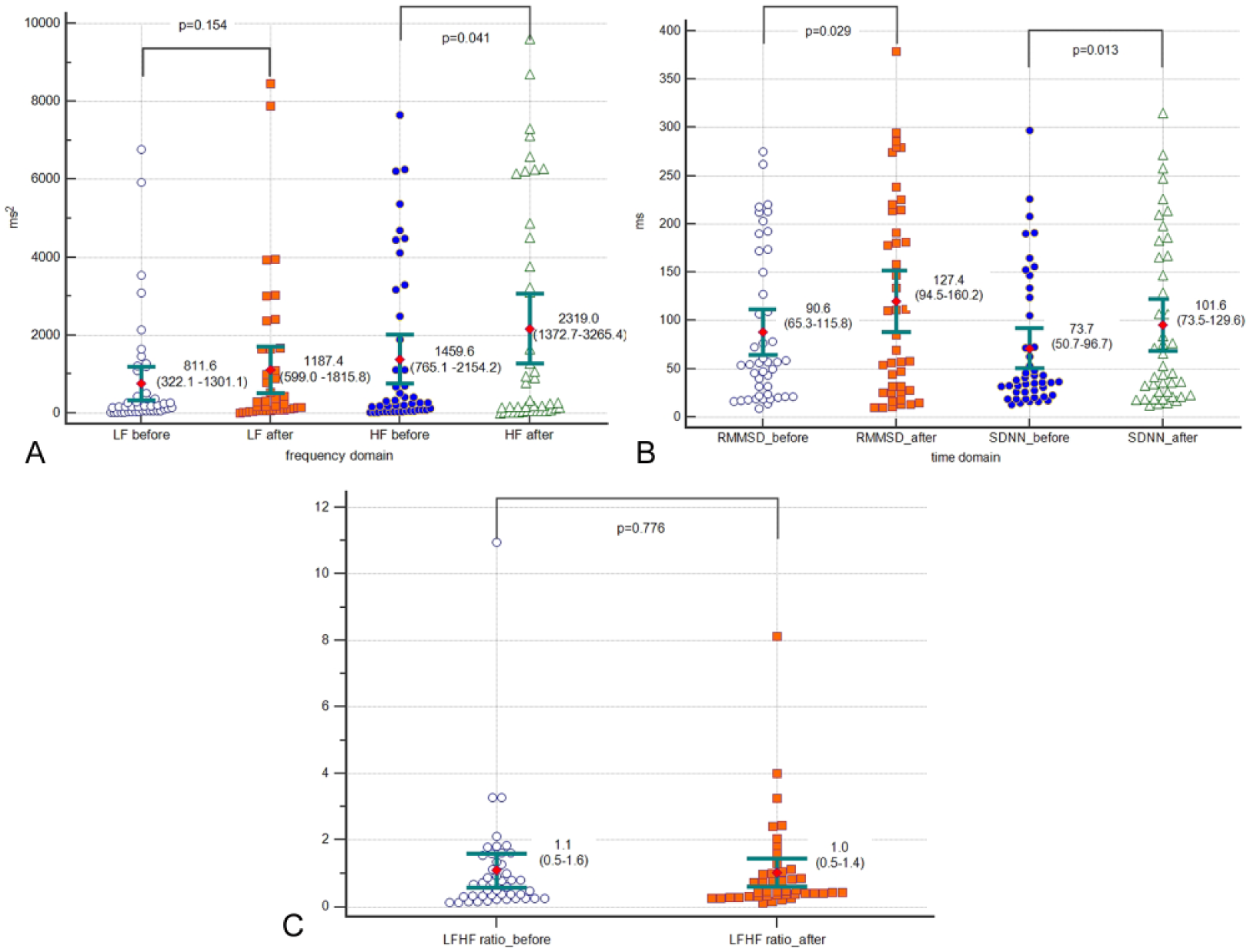
A. Comparison of the high-frequency component (HF), and low-frequency component (LF) before and after Kuan-Sin-Yin intervention in heart rate variability (HRV) analysis. B. Comparison of standard deviation of adjacent peak-to-peak (NN) intervals (which represent the total HRV activity) and the square root of the mean of the sum of the squares of differences between adjacent NN intervals before and after Kuan-Sin-Yin intervention in HRV analysis. C. Comparison of ratio of LF and HF before and after Kuan-Sin-Yin intervention in HRV analysis. Data are expressed as means and 95% confidence interval for mean.
The Effect of KSY on Electrical Conductivity as Measured With MEAD
Table 4 shows the qi meridian energy level as reflected in electrical conductivity (µA). The normal range of the meridian electrical conductivity is 30 to 64 µA. We found that the average of electrical conductivity of both the yin and yang meridians were lower than normal range, indicating abnormally low qi energy in mCRC patients; however, the mean electrical conductivity of the yin and yang meridians were not significantly different before the KSY intervention (yin meridian: 25.33 µA; yang meridian: 26.10 µA; P = .904). After the KSY intervention, we noted an obviously greater increase in the electrical conductivity in the yin meridians than in the yang meridians. Electrical conductivity increased significantly in all 6 of the yin meridians but in only 2 of the yang meridians.
Comparison of Yin and Yang Meridian Energy Before and After Kuan-Sin-Yin Intervention (Measured With the Meridian Energy Analysis Device); n = 52.

Abbreviation: SEM, standard error of the mean.
P < .05 with statistical significance.
The Efficacy of KSY in Relieving Cancer-Related Symptoms and Improving QoL
Table 1 shows the improvement in cancer-related symptoms and QoL measures after the KSY intervention. All cancer-related symptoms except anemia and diarrhea/constipation showed significant improvement. After 2 weeks of the KSY medication, the severity of fatigue, general performance, insomonia, and nausea/vomitting had improved significantly (P < .05). Unsurprisingly, participants reported great improvements in QoL, as shown in responses to both the WHO-BREF and SF-12 (Table 5). In the WHO-BREF questionnaire, scores improved significantly in the physical, psychological, and social scales. In the SF-12 questionnaire, the phycial health composite score also increased significantly.
Comparison of Quality of Life (QoL) Scores Before and After Kuan-Sin-Yin Intervention (n = 52).

Abbreviations: SD, standard deviation; WHO-BREF, Brief World Health Organization Quality of Life Questionnaire; SF-12, 12-Item Short Form Health Survey; PCS, Physical Health Composite Score; MCS, Mental Health Composite Score.
P < .05 with statistical significance.
Discussion
Our results confirmed the hypothesis that the KSY intervention may improve AD in mCRC patients, as reflected in improvements in HRV, meridian electrical conductivity, cancer-related symptoms, and QoL.
KSY Regulates the AD Via Promotion of the Vagal/Sympathetic Dynamic Balance
The ANS controls organ activity and is largely involuntary. Multiple conditions, such as advanced cancer status, may impair its function and lead to AD. 35 The ANS comprises the sympathetic system (which helps the body use energy) and the vagal system (which helps conserve energy and promotes healing); they operate together in a dynamic balance, as in the TCM concept of yin and yang energy. When the sympathetic system calls up more energy, as during severe illness or stress, the ANS is thrown out of balance. 36 A more active sympathetic system, which dominates the vagal system, has been linked with conditions such as cardiovascular disease and mortality. 37 Patients with advanced cancer have symptoms consistent with autonomical insufficiency. Previous studies report significantly higher norepinephrine and lower HRV levels in patients with cancer-related fatigue; lower HRV has also been linked to higher levels of chronic systemic inflammation.1,38
The results of our study showed that the KSY improved the HRV parameters of SDNN (HRV activity), HF, and RMMSD, which may indicate elevated vagal activity. Previous studies have shown that HF power reflects primarily vagal influences; LF power reflects both sympathetic and vagal influences. 37 Translated into clinical implication, the significant increase in SDNN (HRV activity), an index for total ANS activity, means that the participants’ autonomic activity and adaptability were greater after the KSY intervention. This phenomenon is also reflected in the increase in the HF (vagal nerve systemic activity), and RMMSD values. Because KSY is a complex decoction based on the TCM theory of promoting qi energy over the whole body and regulating the ANS dynamic balance, it not only stimulates the vagal tone but also positively affects the sympathetic tone. With the increase seen in the vagal system, the general energy (qi) increased, possibly reflecting the greater ability of the vegal system to conserve energy for healing. Therefore, patients benefit with more adaptability and vitality as a result of the improvement in AD.
The TCM Yin/Yang Theory Applied to AD
The TCM theory of yin/yang can be applied to the effect of KSY on AD. Many studies have measured the electrical conductivity over specific acupoints in TCM meridians and applied these results to activity of the autonomic nerve system.6,15,30,39 We observed a much greater increase in qi energy in the yin meridians than in the yang meridians, a finding that corresponds to the greater increase in vagal tone than in sympathetic tone, as shown by HRV analysis. This result suggests that the yin/yang concept may be compatible with the vagal/sympathetic systems. According to TCM, yin and yang can be characterized as polar opposites just like the vagal and sympathetic systems that control the organs. A more subtle interpretation of the yin/yang principle includes an acknowledgment of the crucial role of the interrelation of the opposites. As with the autonomic control of the heart or any other organ, the interaction between the vagus and sympathetic systems, classically characterized as opposite and reciprocal, can also be both synchronous and synergistic. 40 In fact, the studies of Paton et al 41 proved that the vagus and sympathetic inputs to the heart should no longer be seen as polar antagonists, but more like the yin and yang: different but often complementary. A general interpretation of the process of autonomic control made by Berntson et al 42 in 1991 coincides with the yin/yang theory. Only when the dynamic balance of yin/yang (which corresponds to the vagal/sympathetic system) was reached could the human maintain a healthy status. KSY enhances the qi flow, the so-called “energy,” which may promote the dynamic balance of yin/yang seen in the vagal/sympathetic system.
The Possible Mechanism by Which KSY Improves Cancer-Related Symptoms and QoL
KSY improved most cancer-related symptoms (insomonia, nausea/vomtting, anorexia, pain, fatigue, and performance status) except for anemia and diarrhea/consipatation. The ability of KSY to improve the nausea/vomiting, anorexia, and fatigue may be related to the increase in vagal activity and HRV, which is associated with modulation of the immune system and anti-inflammation. 43 The common mechanism seems to involve lower levels of proinflammatory cytokines such as interleukin (IL)-1 and IL-6 and tumor necrosis factor (TNF). Importantly, increased vagal activity and acetylcholine (the primary parasympathetic neurotransmitter) have been shown to attenuate the release of these proinflammatory cytokines, and sympathetic hyperactivity is associated with their increased production.44,45 We posit that changes in the cytokine levels may account for the improvements in nausea/vomiting, anorexia, and fatigue. Future studies should specifically investigate the mechanisms of microenvironment change associated with KSY in colon cancer.
Meanwhile, KSY may have improved insomnia via regulating vagal activity and increasing the HRV activity (SDNN), consistent with the study by Ter Horst. 46 He found that emotional arousal and physiological irritability were associated with a decrease in HRV attributed to a general inhibitory role of the medial prefrontal cortex via the vagal system. 46 Other studies have shown that SDNN (HRV) is an index of central-peripheral neural feedback and integration of the central nervous system-ANS through the regulation of the inhibitory neurotransmitter γ-aminobutyric acid. 37 KSY may have improved insomnia by stimulating hypervagal activity, reflected in the increase in HRV and yin meridian electrical conductivity.
KSY may have improved the cancer-related symptoms and QoL through the mechanism of regulating the AD but did not affect hematopoiesis. The irinotecan or oxaliplatin chemotherapy regimen in mCRC has side effects of marrow suppression and diarrhea, symptoms that KSY did not improve.
Pharmacological Explanation for the Effect of KSY
TCM pharmacopuncture or acupoint stimulation to regulate the meridian energy has been shown to be effective in reducing cancer pain, fatigue, chemotherapy-related nausea/vomiting, and anorexia.47,48 This is not the first study to show that TCM can be used as an adjuvant therapy to reduce chemotherapy toxicity and improve patient QoL. Other studies indicate that TCM may prolong survival, enhance immediate tumor response, and improve physical performance and energy in some cancer patients. 49 The pharmacological explanation suggests that the effect of KSY may be related to the association of low vagal tone with an exaggerated proinflammatory profile because of the cholinergic anti-inflammatory pathways of the parasympathetic nervous system. 38 KSY not only increased the vagal tone, but may also have reduced inflammation, thanks to the component Glycyrrhiza uralensis, 18 and stimulated the immune system, thanks to the component Poria cocos. 16 In fact, a recent systematic review found that advanced colon cancer patients receiving chemotherapy benefitted from adjuvant TCM ingredients such as Codonopsis pilosula, Atractylodes macrocephala, Poria cocos, or Astragalus membranaceus (including ingredients in KSY); they had improved tumor response rates, survival, and QoL, in addition to fewer adverse events. 50
The Mechanism of KSY in the Cancer Cell Microenvironment
Each ingredient of KSY has been shown to have anti-inflammatory and immune modulation effects via regulation of cytokine secretion.16,18,21,22 However, we do not yet know the possible synergistic or buffering interactions between these herbs in terms of the overall effect of KSY. A very recent study using a mouse tumor model indicated that KSY can impair tumor growth independent of its immune effect because neither the number of tumor-infiltrated lymphocytes nor the expression of anticancer-associated cytokines (TNF-α, interferon-γ, IL-2, and IL-12) were increased after KSY treatment. 9 KSY was shown to inhibit cancer more through the suppression of proliferation of cancer cells than through the enhancement of apoptosis. As the expression of the Ki-67 protein has been well demonstrated to be strictly associated with cancer cell proliferation, the effect of KSY on the cancer microenvironment is via inhibiting Ki-67 expression and increasing the expression of p53 and p21. 9 Moreover, p53 is a protein that serves as a tumor suppressor, and p21 is a known downstream gene of p53. The expression of p53 and p21 may contribute to the downregulation of cyclin-dependent kinases and impair the cancer cell cycle. 51 Becuase multiple molecular mechanisms have been proposed to regulate the p53-modulated pathway and determine the fate of tumor cells, 52 further explorations of these subtle mechanisms are worth exploration.
Limitations
The current study has some limitations. First, no control group was included to measure the possible bias and placebo effects. Second, although the improvement in the vagal tone (HF) was larger than that in the sympathetic tone (LF) in HRV assessment, we could not determine the relationship between HRV modulation and changes in the meridian levels. Even after controlling for the environmental temperature, test pressure, and contact acupoints in this study, skin moisture and the presence of sweat ducts may confound the results obtainable from current electrodermal devices. So far, we can only posit that the concept of yin/yang is relevant to the vagal/sympathetic system based on the similarity of characteristics shown in this and other studies. Based on the tumor-suppressive effects of KSY, the results of this study certainly illustrate the effect of regulating AD in mCRC patients. A larger sample will be needed in a future study to draw stronger conclusions.
Conclusion
In this study, we found that KSY may promote an increase in meridian energy, regulate autonomic activity, and increase HRV to help mCRC patients regain dynamic balance and improve AD, cancer-related symptoms, and QoL. Clinically, KSY helps cancer patients have fewer symptoms and greater QoL. With regard to the future directions for research in the field of TCM in mCRC, because this study suggests the safety and efficacy of adjuvant KSY in mCRC patients, randomized trials should be conducted. We also encourage further studies into the mechanisms by which it works in the tumor microenvironment, which would provide more molecular, pharmacological, or relevant clinical evidence for TCM in mCRC.
Footnotes
Acknowledgements
The authors sincerely thank all patients who participated in this study and colleagues at Lin-Sen (TCM) branch, Taipei City Hospital, Taiwan, as well as all related colleagues who assisted in this study (Government IRB No. TCHIRB-1020127-E).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.