
Abstract
Background. More than 50% of US adults, and an even larger proportion of cancer patients, use dietary supplements. Since many supplements require hepatic metabolism, they may be particularly likely to cause toxicities in patients with hepatocellular carcinoma (HCC). However, little is known about supplement use in patients with HCC. Methods. From 2008 to 2012, we gave newly diagnosed HCC patients at our institution a standardized questionnaire about dietary supplement use, demographic factors, and clinical characteristics. We then followed patients for four years or until time to death to examine the relationship with supplement use. Results. Of 146 patients, 71% had used vitamins and 45% herbal supplements. Most commonly used supplements were antioxidants (51%), multivitamins (46%), vitamin D (25%), and milk thistle (23%). People in mid-higher income brackets were more likely to use herbal supplements (19% of those earning <$30 000, 50% of those earning $30 000-60 000, and 34% of those earning >$60 000 used supplements). Hepatitis C (HCV) patients were more likely to use milk thistle than those without HCV (30% vs 13%, P = .03), and patients with hepatitis B (HBV) were more likely than non-HBV patients to use vitamin C (32% vs 14%, P = .01). Supplement use was not associated with overall survival. Conclusions. Like cancer patients in other studies, the majority of our HCC patients used dietary supplements. Supplement use was not associated with overall survival but should be studied in larger patient samples.
Keywords
Introduction
From 1975 to 2005, the incidence of hepatocellular carcinoma (HCC) tripled in the United States. 1 Although HCC patients diagnosed in early stages may receive curative therapy, treatment options are limited for those with advanced disease. 2 Many patients with cancer or liver disease take dietary supplements often without informing their providers, hoping to improve their health and/or quality of life.3,4
According to data from the National Health and Nutrition Examination Surveys (NHANES) III, dietary supplement use has increased from 42% in the period between 1988 and 1994 to 53% from 2003 to 2006 in the general population.5,6 Supplement use is common in patients with cancer (26% to 87%) and in patients with liver disease (27% to 43%),7-9 despite the lack of clear evidence regarding efficacy or safety.7,10,11
Our goal was to measure the prevalence of dietary supplement use in a prospective study of subjects with HCC and to determine demographic and clinical characteristics associated with supplement use. In this study, we also examined whether use of these agents was associated with overall survival. To our knowledge, this study is the first to assess supplement use and survival prospectively in a US HCC cohort.
Materials and Methods
Study Population
From October 2008 to November 2012, we recruited 146 HCC patients to participate in the study and followed them until December 2012. Patients were eligible if they were age 18 years or older and had an HCC diagnosis based on American Association for the Study of Liver Diseases (AASLD) guidelines, or biopsy. Previous resection or locoregional therapy were allowed as long as measurable disease was seen on imaging by Response Evaluation Criteria in Solid Tumors (RECIST). Exclusion criteria included a diagnosis of another malignancy within the last 5 years, decompensated Child-Pugh (CP) B or C liver disease, prior liver transplant, or prior systemic therapy for HCC.
Measures
On enrollment, subjects completed a questionnaire examining demographic factors (race, ethnicity, education level, employment, and income status), medications (including dosing, frequency, indication, and timing of usage), and social history (including drug, tobacco, and alcohol use [categorized as having consumed 2 or more standard drinks per day (28 g) for more than a year at any point in the patient’s life]). Subjects were asked about their use of supplements, specifically multivitamins, vitamins A, B-complex, C, D, and E, calcium, DHEA, gingko biloba, ginseng, glucosamine chondroitin, milk thistle, St John’s wort, and echinacea; participants were also asked for names of any additional supplements used. Baseline blood samples were drawn, including complete blood count, basic metabolic panel, liver function, coagulation function, and tumor markers (including α-fetoprotein [AFP] levels). We also checked a viral hepatitis panel, autoimmune serologies (antinuclear antibody, antismooth muscle antibody, antimitochondrial antibody), iron studies, ceruloplasmin, and α-1 antitrypsin levels to determine etiology of liver disease. Diabetes diagnosis was based on fasting glucose level, hemoglobin A1c, or clinical history obtained through the medical record system. Nonalcoholic steatohepatitis was defined as having an elevated body mass index or diabetes, with no other underlying cause of liver disease. Radiologic, pathologic, and laboratory reports were collected from the electronic medical record at the time of enrollment and were used to calculate CP score and Barcelona Clinic Liver Cancer (BCLC) stage. Survival data were obtained from hospital records and the Social Security Death Index. The protocol was approved by our university’s institutional review board, and written informed consent was obtained from all subjects.
Statistical Analysis
Associations between the use of different supplements and baseline clinical characteristics of study participants (all as categorical variables) were analyzed using χ2 tests. Each supplement was analyzed individually and in the following categories: vitamins (A, B-complex, C, D, E), antioxidants (vitamins C, E, and selenium), and herbal supplements (nonvitamin dietary supplements). Kaplan–Meier plots and Cox proportional hazard models were used to determine the associations between each supplement use and time to death. Variables that were clinically relevant and showed statistical significance in univariable analysis were included in the multivariable Cox proportional hazards models. Subjects contributed person-time to the study from the date of enrollment to the date of death/date of censoring. Subjects were censored if they were either lost to follow-up or at the end of the study period (December 2012). Baseline overall supplement use was not different for the 18 patients that were lost to follow-up compared with the rest of the cohort. All tests of statistical significance were 2-sided. All analyses were done using SAS, Version 9.3 (SAS Institute Inc, Cary, NC).
Results
Of 146 patients in our cohort, 115 (79%) were men. The median age at enrollment was 62 years. Many subjects had more than one underlying etiology of cirrhosis: 60% had underlying hepatitis C virus (HCV), 38% had hepatitis B virus (HBV), 27% reported significant alcohol use, and 33% had diabetes. Overall, 57% of subjects initially met the Milan criteria by imaging (disease limited to the liver without vascular invasion, with 1 lesion 5 cm or less or 3 lesions each less than 3 cm). Not all patient records had complete data in each category; we excluded patients from analyses who lacked relevant data.
Overall, 71% of subjects reported using vitamins prior to or at the time of their HCC diagnosis, and 45% reported using herbal supplements. Most commonly used were antioxidants (51%), multivitamins (46%), vitamin D (25%), and milk thistle (23%). Vitamin use overall and vitamin D use were more common in women than in men (82% vs 68%, P = .15, and 43% vs 21%, P = .02, respectively) (Table 1 and Supplemental Table 1; supplemental tables are available online at http://ict.sagepub.com/supplemental). Only 19% of patients earning <$30 000 per year, but 50% of those earning $30 000 to 60 000, and 34% of those earning more than $60 000 annually used herbal supplements (P = .04), as did 47% of employed, but only 27% of unemployed subjects (P = .02) (Table 1). HBV patients were more likely to take vitamin C than non-HBV patients (32% vs 14%, P = .01) (Supplemental Table 1), HCV patients were more likely to use milk thistle (30% vs 13%, P = .03) and less likely to take vitamin D (18% vs 36%, P = .02) or E (9% vs 25%, P = .01) than patients without HCV (Supplemental Tables 1 and 3).
Demographic and Clinical Characteristics of Vitamin and Herbal Supplement Users a .
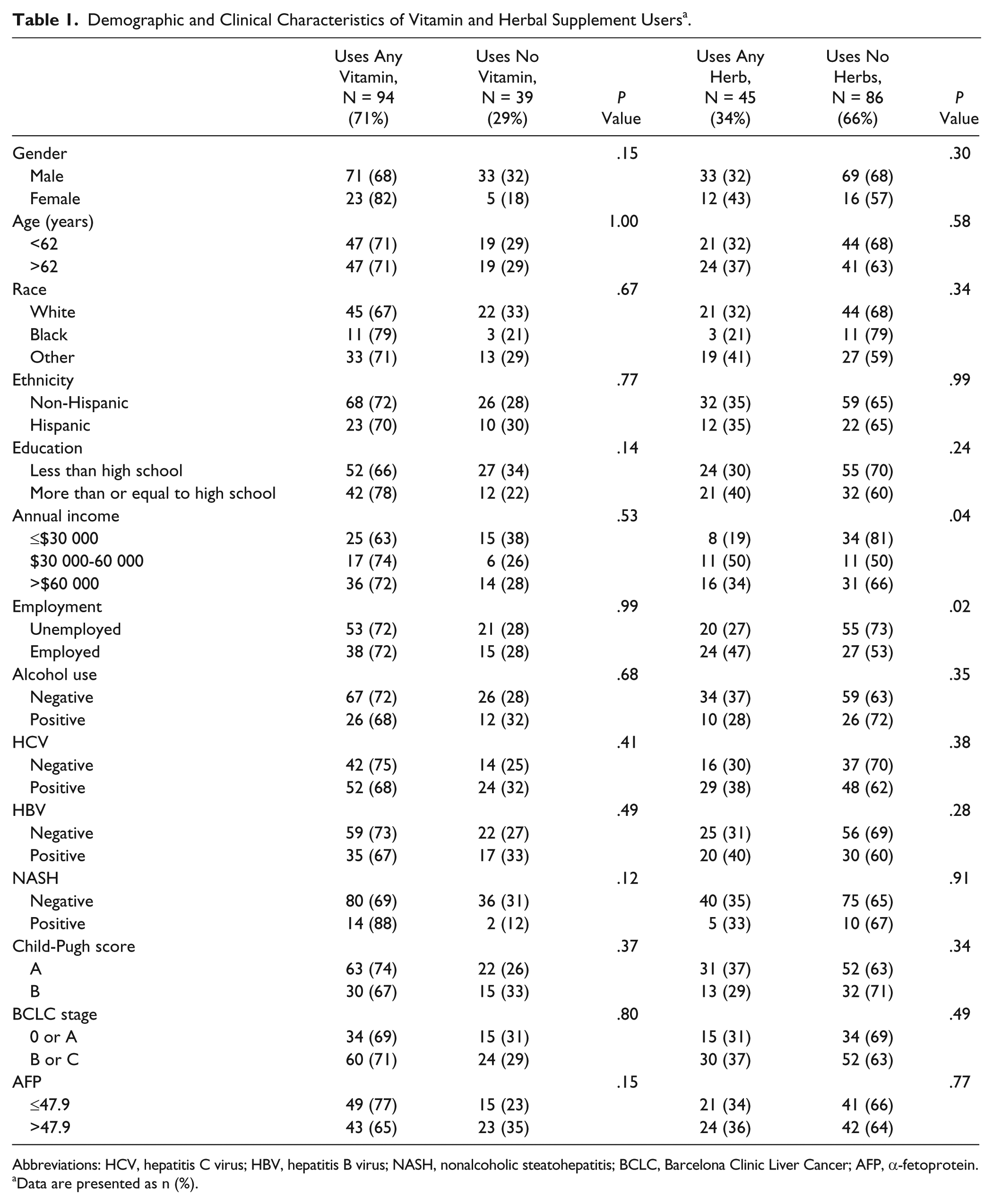
Abbreviations: HCV, hepatitis C virus; HBV, hepatitis B virus; NASH, nonalcoholic steatohepatitis; BCLC, Barcelona Clinic Liver Cancer; AFP, α-fetoprotein.
Data are presented as n (%).
Mean follow-up of our patients was 309 days. Only 40% of our patients survived 2 years or more. In our Kaplan–Meier analysis, patients who used milk thistle had marginally poorer survival than nonusers (Figure 1). However, after adjusting for alcohol use, AFP, CP score, and BCLC stage, supplement use was not associated with overall survival (Table 2). Though patients were asked to provide start and stop dates of all medications, most did not include information regarding timing of use.
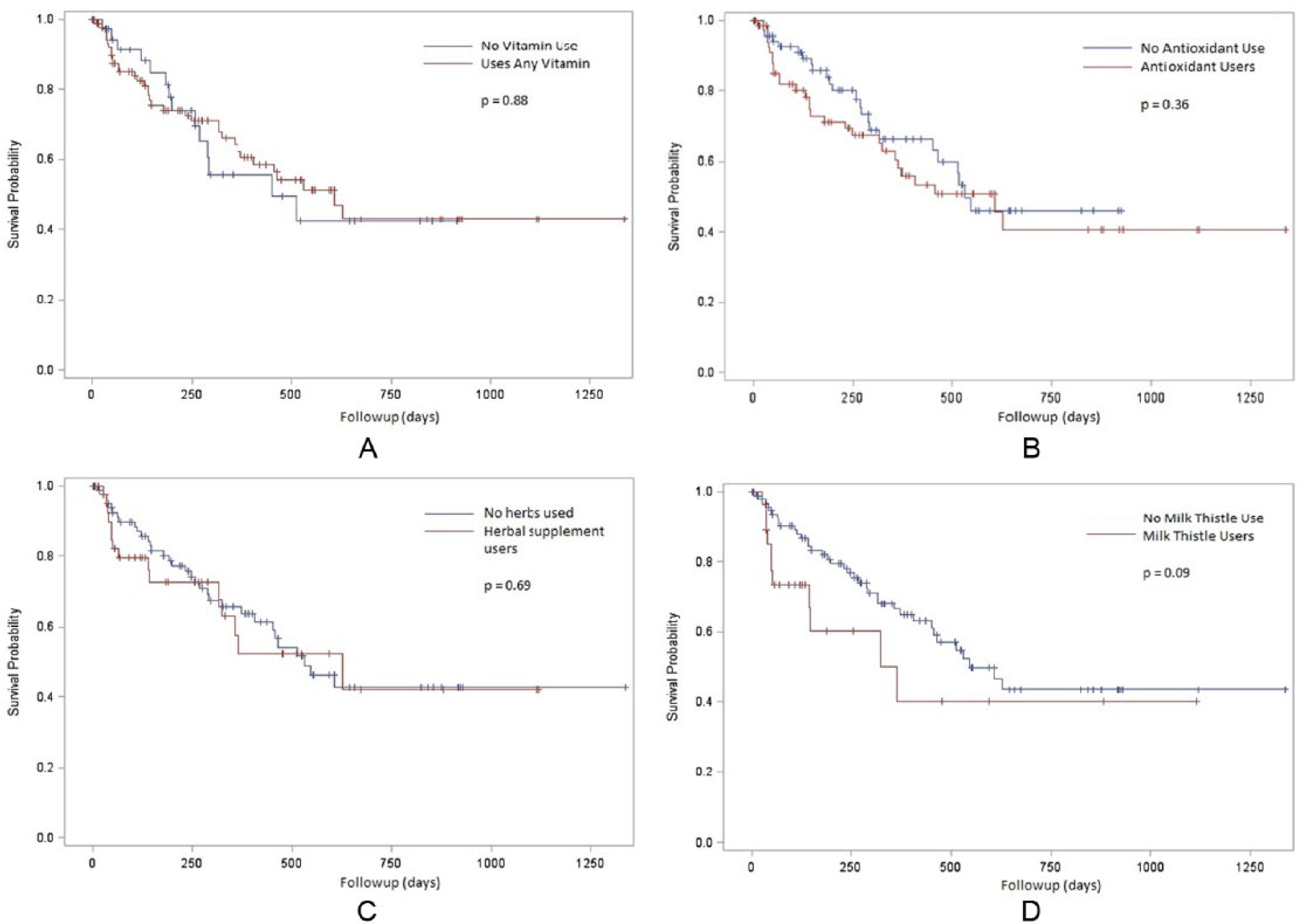
Kaplan–Meier survival curves for (A) any vitamin, (B) antioxidants, (C) herbal supplements, and (D) milk thistle.
Hazard Ratios for Supplements Use and Overall Survival as Adjusted for Known Risk Factors for Mortality in Patients With HCC.
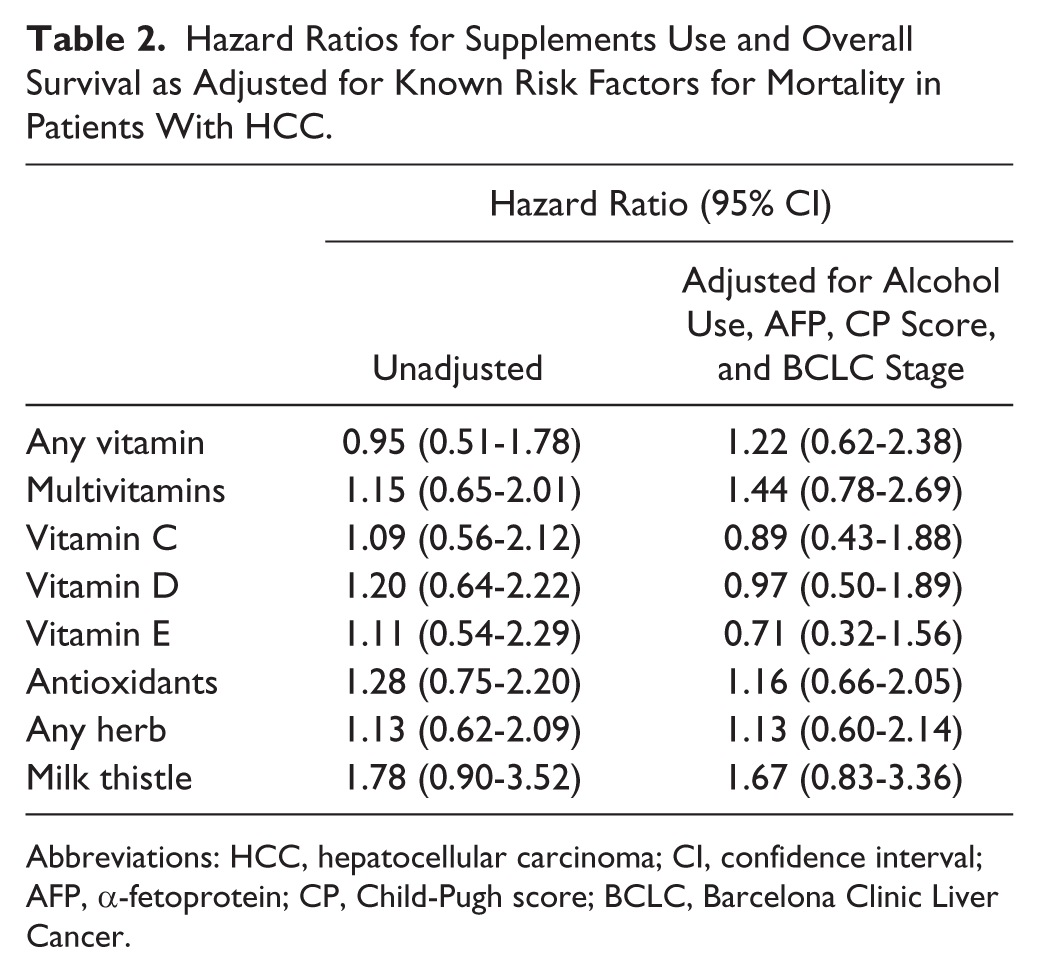
Abbreviations: HCC, hepatocellular carcinoma; CI, confidence interval; AFP, α-fetoprotein; CP, Child-Pugh score; BCLC, Barcelona Clinic Liver Cancer.
Discussion
The American Cancer Society recommends that patients not use dietary supplements, particularly while receiving radiation or chemotherapy. 12 In our single-institution study, at the time of diagnosis, 71% of patients reported prior vitamin use and 45% reported using some form of herbal supplement. Like other studies of cancer patients, ours found supplement users to be more educated and more often female than nonusers, 5 but the differences were not statistically significant.
Although dietary supplements have been popularized as preventive agents against cancer, the US Preventive Services Task Force has found insufficient evidence to support this use, and a recent editorial in the Annals of Internal Medicine recommended strongly against supplement use for this purpose.13-15 However, observational studies have shown that vegetables and fruits high in antioxidants may be protective against some cancers, and the Physicians Health Study II showed that use of multivitamins may provide a small, but significant, decrease in risk of cancer.16,17 In addition, the Vitamin D and OmegaA-3 Trial (VITAL) suggest that grapeseed extract may protect against prostate cancer, and fish oil may protect against breast cancer.18,19 In contrast, in the Alpha-Tocopherol, Beta-Carotene (ATBC) and the Beta-Carotene and Retinol Efficacy trials, high-dose β-carotene was associated with an 18% increase in risk of lung cancer (although in ATBC, vitamin E users had a 32% lower risk of prostate cancer than nonusers).20-22 A recent study using NHANES III data suggested a more complex relationship between various antioxidant levels and overall mortality, 23 as those with antioxidant insufficiency were at higher risk of cardiovascular and cancer mortality, but the benefit of higher serum levels of supplements plateaued. Similarly, in prior studies in Linxian, China, remediating some known vitamin insufficiencies helped decrease mortality from esophageal and gastric cancer; however, supplementation in well-nourished populations in Venezuela did not show as beneficial an effect in preventing gastric cancer.24-26 The idea that antioxidants might protect cancer cells from effects of cytotoxic chemotherapy or radiation is not yet clearly supported by evidence.11,27 However, the ability to study supplement use rigorously in both cancer prevention and treatment has been limited by the lack of standardization of supplement formulations and dosing.28-30
Despite the unclear benefits of supplements, use tends to increase after a cancer diagnosis.8,9,31 In 1998, Ernst and Cassileth reported a systematic review of 26 studies evaluating complementary alternative medicine (CAM) use in cancer patients, and they found that 40% of patients reported alternative medicine use. This review was limited as each individual study defined CAM differently, including both nonpharmacologic treatments and dietary supplements. 32 Subsequent meta-analyses through 2008 have showed the continued rise of supplement use to 64% to 81% among cancer patients. 9 Prostate cancer patients are generally the least likely to report supplement use (26% to 35%), while breast cancer patients tend to be more likely to report use (67% to 87%). 9 International studies confirm the increased use of alternative medicine among cancer patients worldwide.8,29,31,33 This use is also often not disclosed to treating oncologists, in part due to discordant beliefs of patients and healthcare providers regarding the benefits of supplements. 34
Gender differences may be partially responsible for the differences between prostate and breast cancer patients in reported use of supplements. However, although our sample was predominantly male (79%), many of our patients were supplement users, perhaps because of their concurrent or previously diagnosed liver disease. In studies of patients with chronic liver disease, 27% to 39% reported alternative medicine use, and among Canadian patients with hepatitis C, 46% reported using dietary supplements.35-37
Vitamin E and other antioxidants have been evaluated in treatment of nonalcoholic fatty liver disease, 38 and remedies such as milk thistle (Silybum marianum) have been used for centuries as treatments for liver disease. 39 A recent randomized controlled trial of 154 patients with chronic HCV showed no effect of high dose oral silymarin on hepatic function or viral load, although several smaller studies showed suppression of HCV viral load with high-dose IV milk thistle.40,41 Other herbal remedies marketed for patients with liver disease, such as licorice root, phyllanthus, or Liv-52, continue to be studied, but are used by less than 1% of the population of patients with liver disease, 37 and none of the participants in our study reported using these supplements.
Patients with HCC are at risk for drug–drug interactions that may be exacerbated by complications of cirrhosis (hypoalbuminemia, alterations of P450 systems, coagulation abnormalities, etc).42-44 Reassuringly, we found no significant adverse relationship between supplement use and survival. However, our observation that milk thistle users had slightly higher overall mortality than nonusers is potentially worrisome in light of a recent study of milk thistle use among patients with advanced liver disease. The study was closed early due to higher than expected early mortality. 45 These studies call for further study of supplement use among HCC patients. Our findings also reinforce recommendations that physicians discuss supplement use with patients to minimize potential risks and drug interactions.
Our study involved a relatively small cohort at a single institution. However, our institution is a quaternary referral center that also serves as a primary care center for a diverse patient population. Another limitation is that we were not able to collect data on time period, duration, and dosage of supplements for most patients. Future studies should attempt to elicit more specifics regarding both supplement use and the clinical features and outcomes of those using and not using supplements. Our study found that general supplement use was widespread among our HCC patients. Though we saw no overall survival benefit of supplements, subgroups with vitamin/supplement insufficiency may benefit more from supplementation than those who have adequate levels of micronutrients. Future studies might measure serum levels to examine that possibility. Further studies of the relationship of supplement use with outcomes among patients with HCC should provide a basis for more informed discussions between patients and providers.
Conclusion
Our study showed that the majority of patients with HCC use some form of dietary supplements. We found no clear association between supplement use and survival, but future studies may benefit from identifying subgroups that may be more affected by dietary supplementation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH K23 CA 149084-01 A1 and the Steven J. Levinson Medical Research Foundation (ABS).