
Abstract
Introduction. Compared with White breast cancer survivors, African American survivors are more likely to be overweight and obese. Differences in weight status may be attributed to differences in dietary intake; however, there is limited research pertaining to the dietary habits of African American breast cancer survivors. Methods. We compared baseline dietary intakes of 31 overweight and obese African American breast cancer survivors enrolled in a healthy lifestyle intervention to national dietary guidelines and also examined beverage intake habits. Dietary intake was assessed using the National Cancer Institute’s Diet History Questionnaire and beverage intake was assessed using 3-day food intake records. Results. Overall, the majority of survivors consumed the recommended daily servings of fruits and vegetables (71.0%) and red meat (83.9%); however, survivors exceeded national recommendations for energy intake from fat (64.5%), saturated fat (87.1%), and added sugars (77.4%). Few women met the guidelines for whole grain and fiber intake (6.5% and 35.5%, respectively). Additionally, survivors consumed ~10% of total energy intake from beverages alone and drank only ~3.5 cups of water daily. Conclusions. Current dietary guidelines for cancer survivors recommend consuming >5 servings per day of fruits and vegetables and broad guidelines regarding limiting discretionary fat and added sugars but do not specify beverage intake recommendations. Future dietary interventions in African American breast cancer survivors should focus on reducing intake from dietary fat and added sugar, as well as increasing whole grain consumption as a means for increasing daily fiber intake. Furthermore, substituting caloric beverages with water or noncaloric beverages may be a strategy to decrease caloric intake in African American breast cancer survivors. Nutrition information targeting these nutrients could be administered during treatments or doctor’s visits as a means to prevent weight gain that often occurs following diagnosis.
Introduction
Breast cancer survivors make up the largest group of cancer survivors (22%) in the United States. 1 Several lifestyle factors, including participation in physical activity and consuming a healthy diet have been deemed potential protective factors that may help to reduce a woman’s risk for breast cancer. Alternatively, obesity is considered a risk factor for developing postmenopausal breast cancer. Obesity is also associated with increased risk for breast cancer recurrence and increased cancer mortality,2-5 increased risk of comorbidities,6,7 and poor quality of life and physical functioning.8,9 Considering there have been substantial increases in the percentage of the US adult population who are overweight and obese over the years, with the greatest increases observed among African American women, 10 strategies to improve dietary habits among this minority population should be a priority.
Currently, there are few studies examining dietary intake in minority breast cancer survivors. Stolley et al 11 conducted a weight loss intervention in African American breast cancer survivors and measured dietary intake using the Block ’98 Food Frequency Questionnaire. At baseline, participants reported higher percentages of energy intake from fat and lower consumption of fiber than what is recommended by the dietary guidelines. 12 The WHEL (Women’s Healthy Eating and Living) study was a dietary intervention looking at the effects of a low-fat, high fruit, vegetable and fiber diet on breast cancer recurrence and overall survival in women. 13 Secondary analyses of this study have been conducted by Paxton and et al 14 found that at baseline, African American women consumed higher intakes from fat, lower intakes of fiber and fewer servings of fruits and vegetables compared with Asian American and White participants; over the 4-year follow-up period, African Americans were less likely than White, Asian American, and Hispanic women to maintain improvements in fiber intake, percentage of energy from fat and servings of vegetables. Saquib et al 15 reported differences in dietary energy density (food only; kcal/g) between racial/ethnic groups. Dietary energy density may be an indicator of diet quality; low energy-dense foods, such as fruits and vegetables, contribute few calories while providing greater bulk to the diet, whereas higher energy-dense foods contain greater amounts of fat and calories. 16 African American women had the highest dietary energy density (food only) compared with Whites, Asian Americans, and Hispanics at baseline, 15 which would suggest these women were consuming a diet higher in fat.
The American Cancer Society (ACS) recently released nutrition guidelines for cancer survivors. 17 These recommendations include achieving a dietary pattern that is high in fruits, vegetables and whole grains; these recommendations also include following the ACS Guidelines of Nutrition and Physical Activity for Cancer Prevention. 18 Some of the recommendations within these guidelines are specific (ie, consume ≥2.5 cups of fruits and vegetables daily), whereas others are broad (choose foods and beverages in amounts that help achieve and maintain a healthy weight) and do not provide recommendations for specific macronutrients (ie, fat or saturated fat). Additionally, the guidelines acknowledge the dearth of research related to nutrition behaviors among cancer survivors. We expand knowledge in this area by comparing the dietary intake of overweight and obese African American breast cancer survivors with national dietary recommendations for cancer survivors. Data are also presented on beverage consumption including amounts of drinking water and energy-containing beverages, and with these data we highlight potential targets for nutrition education and future weight maintenance or weight loss interventions in African American breast cancer survivors.
Methods
Study Design
This report is focused on dietary assessments from African American women who were enrolled into a randomized clinical trial, Stepping Stone (Survivors Taking on Nutrition and Exercise). Stepping Stone was an intervention that focused on improving healthy behaviors (ie, physical activity and nutrition) and quality of life among African American breast cancer survivors. The study protocol was approved by the institutional review board of Georgetown University. All participants provided written informed consent prior to study enrollment.
Participant Characteristics
Overweight or obese (body mass index [BMI] >25 kg/m2) African American women older than 21 years were recruited from the Washington, DC, metro area using flyers, e-mail listservs, newspaper advertisements, and referrals from medical providers. Eligible women, self-identified as African American/black, were diagnosed with nonmetastatic breast cancer and were at least 1 month beyond active treatment (eg, chemotherapy, etc).
Measurements
Anthropometrics
Measures of height, weight, and waist circumference were recorded by a trained exercise physiologist. Height was measured by a stadiometer to the nearest 0.5 cm without shoes; body weight was measured to the nearest 0.1 pound in light clothing without shoes using a standard digital scale (Seca 813, Hanover, MD). Height and weight were used to calculate BMI. Waist and hip circumference were used to assess abdominal obesity using a standard tape measurer. Waist-to-hip ratio was also calculated to assess abdominal obesity.
Dietary Intake
Dietary intake, including daily energy intake, percentage of energy from fat, saturated fat, grams of discretionary fat, fiber and added sugars, servings of fruits, vegetables, total and whole grains, and alcohol, and energy density was measured using the National Cancer Institute’s Diet History Questionnaire (DHQ). The DHQ is a 36-page, 124-item questionnaire that measures food frequency and intake amount over 12 months. The DHQ was self-administered but was reviewed by a trained nutritionist for errors. Reponses from questionnaires were manually entered into the database and analyzed using Diet*Calc (NCI Diet*Calc Analysis Program, Version 1.4.3. November 2005). Studies have shown that the DHQ provides reliable estimates of energy intake, and it has been validated.19,20
In a subset of the study group, 4-day food intake records were collected. Participants were instructed to record their food/beverage (including water) intake, and records were reviewed for accuracy and completeness by a trained nutritionist prior to analysis using the NDS-R nutritional analysis software (NDS-R, University of Minnesota, Minneapolis, MN). Habitual beverage consumption was assessed using 4-day food intake records that were manually reviewed to calculate mean daily amounts (kilocalories, grams) of water and other beverages consumed. Total water intake from all foods and beverages was also recorded. Total water intake and beverage data was calculated from 4-day food records because the DHQ does not provide these data.
Compliance to Dietary Recommendations
Compliance to the ACS guidelines was determined for each dietary component. “Eat 5 or more servings of a variety of vegetables and fruits each day”: Participants were categorized as compliant if they consumed ≥5 fruit and vegetable servings per day. To calculate variety of fruits and vegetables consumed, we determined the percentage of servings from the following fruit and vegetable categories: dark green vegetables; deep yellow vegetables; other vegetables; tomato; citrus melon berry categories. A participant was compliant if she consumed 10% or more servings a day from 2 or more of those fruit and vegetable categories. “Limit consumption of processed and red meats”: Weekly processed and red meat intake was calculated by combining the DHQ variables “Oz lean meat from beef pork lamb, etc,” “Oz lean meat from organ meats,” and “Oz lean meat from franks luncheon meats,” and multiplying by 7 days. Compliance was defined as consuming <18 oz/wk (American Institute for Cancer Research recommendations for oz/week 21 ). “Choose whole grains in preference to processed (refined grains)”: To calculate percentage of whole grain intake, we divided whole grain intake by total grain intake. Compliance was defined as consuming >50% of total grains from whole grains. “If you drink, limit consumption to 1 drink/day for women”: Compliance was defined as consuming <1 alcoholic drink per day. Given the associations with breast cancer and alcohol consumption, we also calculated compliance with American Institute for Cancer Research’s recommendation of consuming no alcohol (0 drinks/day; nondrinker). 22
When recommendations were not included in the ACS guidelines, we referred to additional guidelines from governmental and nongovernmental organizations for comparisons. Compliance for recommendations not included in the ACS guidelines were defined as follows: fiber, >21 g/d 23 ; dietary fat,<35% total daily energy24,25; saturated fat, <7% total daily energy24,25; added sugars, <6 teaspoons/d 24 ; total water intake from all foods and beverages, >2.7 L/d. 23
Statistical Analysis
Statistical analyses (SPSS version 20, IBM Corp, Armonk, NY) include descriptive statistics for participant characteristics. Data are presented as mean ± SEM, or as n (%) when applicable.
Results
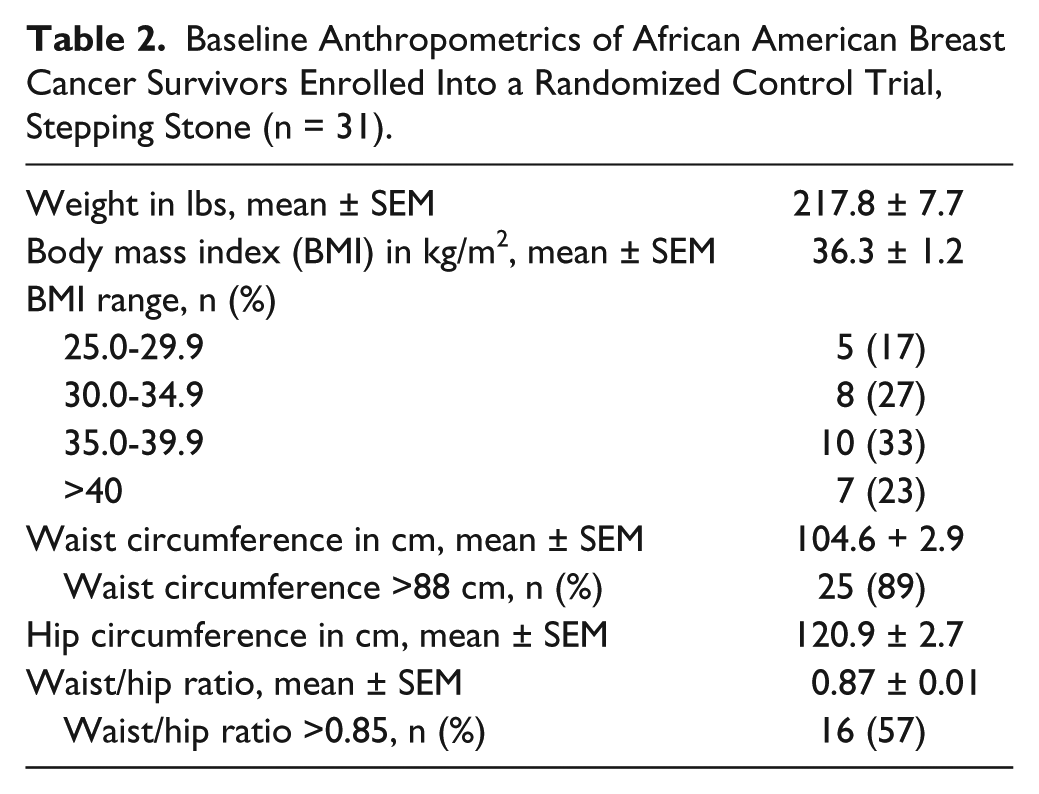
Overall, 31 participants completed the DHQ and were included in the analysis. Participant demographics and breast cancer treatment data are presented in Table 1. Participants were primarily older, educated women. Approximately two thirds of the women had at least a college degree, and the majority of women were married or single. Data regarding stage and treatment history were available for 14 women. Of these women, the majority received chemotherapy and/or radiation therapy, and few reported taking hormone therapy. Additionally, the majority of our sample was diagnosed with stage 1 or 2 breast cancer. Anthropometric measures are presented in Table 2. The majority of our sample had abdominal obesity and nearly 25% of our sample was classified as having extreme obesity (class III).
Baseline Participant Characteristics of African American Breast Cancer Survivors Enrolled Into a Randomized Control Trial, Stepping Stone (n = 31).

Baseline Anthropometrics of African American Breast Cancer Survivors Enrolled Into a Randomized Control Trial, Stepping Stone (n = 31).
Self-reported dietary intake and the comparison of the ACS cancer prevention guidelines to our sample’s self-reported dietary intake can be found in Table 3. The majority of participants consumed more than the recommended servings of fruits and vegetables and also consumed a variety of fruits and vegetables. Additionally, the majority of participants consumed fewer than 18 oz. of red and processed meat weekly, and the majority complied with the ACS alcohol recommendations. On the contrary, few participants consumed the recommended servings of whole grains.
Baseline Self-Reported Dietary Intake and Compliance to National Dietary Recommendations of African American Breast Cancer Survivors Enrolled Into a Randomized Control Trial (n = 31).

Four-day food records were used to calculate total water intake.
We also compared self-reported dietary intake with the dietary recommendations that are not included in the ACS guidelines but can be found through the Institute of Medicine (IOM), American Heart Association (AHA) and the US Department of Agriculture (USDA) 2010 Dietary Guidelines for Americans (Table 3). Fiber intake was lower than the generally accepted IOM recommendations for women of 21 to 26 g/d. Dietary fat intake was higher than the recommended 25% to 35% by the AHA and IOM, as was energy intake from saturated fats. Discretionary fat was also higher than previously reported intake in women between the ages of 50 and 59 years. According to the USDA Continuing Survey of Food Intake by Individuals, 1994-1996, average intake in this age-group was 44.5 g. 26 Women in our sample consumed more than 11 teaspoons of added sugar daily. This quantity exceeds the upper limit of added sugar intake recommended by the AHA (6 teaspoons for women) 27 and USDA Dietary Guidelines (8 teaspoons). 28
Of the 31 participants who completed the DHQ, 48% (n = 15) also completed the 4-day food intake records that were used to assess beverage intake data. Total water intake from foods and beverages was 1810 ± 234 g/d, and drinking water intake was 853 ± 242 g/d. Daily energy intake and added sugar intakes from beverages alone were 173 ± 48 kcal and 14.2 ± 3.1 g, respectively. Overall, participants consumed 10.3% of total energy intake from beverages; approximately 3.6 teaspoons of added sugars were from beverages alone.
Discussion
In our sample, the majority of women consumed the recommendations for fruits, vegetables, and red and processed meat, but failed to meet the recommended intakes for fat, saturated fat, whole grains, added sugars, or total water. The ACS guidelines recommend limiting foods and drinks high in calories, fat and/ or added sugars, but do not provide recommendations on specific intakes other than fruits and vegetables. The promotion of national campaigns to increase fruit and vegetables servings (5 a Day for Better Health Program, 29 Fruits and Veggies–More Matters 30 ) in conjunction with the specific ACS recommendations may explain the high intakes of fruits and vegetables in our sample. Considering that our sample also met the serving recommendations for red and processed meat, our results suggest these women are consuming their saturated fat intakes from nonmeat sources as evidenced by the high intakes of discretionary fats. Other than high-fat meats, common sources of discretionary fats in the American diet include grain-based desserts, regular cheese, pizza, fried foods, and dairy desserts. 31 Given the comorbidities associated with breast cancer (ie, cardiovascular disease and diabetes), it may be beneficial to educate women about the risks associated with consuming high amounts of solid fats and added sugars.
To our knowledge, no studies have reported data on added sugar intakes or beverage intake patterns of African American breast cancer survivors. This is important given that energy containing beverages, such as soft drinks and fruit drinks that provide energy but do not contain essential nutrients, are the largest contributors to beverage calories, 32 and may promote weight gain. 33 Furthermore, increased intake of nondiet soft drinks is positively associated with BMI, 34 weight gain, risk of type 2 diabetes,35,36 enhanced fat accumulation in the liver, muscle, and visceral adipose tissue,37,38 and risk factors for the metabolic syndrome.35,39 Our sample of African American breast cancer survivors consumed 173 calories from beverages daily. Because calories from beverages are not as satiating as calories from solid foods40-43; reducing energy-containing beverage intake may be an important topic to explore given the rates of weight gain and obesity in breast cancer survivors.44-49 Alternatively, higher intakes of energy-free beverages such as water, unsweetened tea and coffee, and diet sodas may reduce the risk of weight gain 36 and promote weight loss.50-55 Though there is no current recommendation for drinking water intake, the IOM Food and Nutrition Board determined an adequate intake for total water intake for adult females older than 19 years of 2.7 L/d. 23 This includes total water from all beverages, drinking water, and moisture from foods to promote euhydration. In our sample, participants were consuming nearly 1 L less than the total dietary water intake recommendations and consumed ~3.5 cups of drinking water per day. Strategies to promote increasing drinking water intake may be warranted to promote euhydration and weight loss within this population.51,53,54,56
There are a few limitations to our study that we should acknowledge. First of all, this was a relatively small sample. However, few studies have focused on the dietary habits of African American breast cancer survivors, and to our knowledge none have presented data on beverage intake in African American breast cancer survivors. Given the associations with breast cancer treatment and weight gain, reducing energy-containing beverage intake may be an important target for nutrition education within this population. Also, our sample size is similar to previous interventions targeting African American breast cancer survivors. 11 Another limitation is that we used self-reported dietary data. We tried to overcome this limitation by using 2 methods of dietary intake collection. Finally, the majority of women in our study were well educated and therefore our dietary reports may not reflect those of individuals with lower levels of education. Previous investigations have shown that higher levels of education may be associated with increased diet quality.57-59 This may be explained by increased nutritional knowledge and the ability to use this knowledge to make better dietary selections. However, the proportion of women with at least some college education in our study is similar to prior data we have collected from the Washington, DC, metro area. 60 Despite higher education levels among our participants, many women in our study failed to meet many of the dietary recommendations, which is consistent with overall dietary patterns of American adults.57,58,61 Though the results of this study cannot be extrapolated to the general population, we present nutrition education targets that could be incorporated into weight management programs or interventions for African American breast cancer survivors. African American breast cancer survivors have higher rates of obesity than survivors of other racial groups and are more likely to have comorbidities such as hypertension or diabetes. 62 Interventions to improve dietary behaviors are warranted in this population to reduce obesity and other related comorbidities.
Conclusions
According to our results, future interventions targeting nutrition education in African American breast cancer survivors should focus on decreasing fat intake as a means to reduce dietary energy density, increasing whole grain consumption, and reducing consumption of added sugars and energy containing beverages. Current recommendations suggest increasing fruit and vegetable intake; yet our sample was currently exceeding these recommendations. Providers may want to consider promoting the ACS guidelines for survivors in addition to other national guidelines such as the USDA 2010 Dietary Guidelines or the AHA dietary recommendations so that survivors have quantitative guidelines to follow as opposed to broader recommendations. Simple dietary interventions that focus on these nutrition education targets presented could be administered during treatments or doctor’s visits as a means to prevent weight gain that often occurs following diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funding in part with funds from the National Cancer Institute (R21 CA14996; VBS and LAC).