
Abstract
Hypothesis. Qigong exercise is a popular method for relieving the side effects of conventional cancer treatments in survivors of breast cancer, yet its effects are not empirically assessed. This study aimed to investigate the effects of qigong exercise on upper limb lymphedema, arterial resistance, and blood flow velocity in survivors with breast cancer and mastectomy. Study Design. This study was conducted as a prospective clinical trial. Methods. Eleven survivors of breast cancer with qigong experience (mean age = 58.3 ± 10.1 years) were assigned to the experimental group and 12 survivors of breast cancer without qigong experience (mean age = 53.8 ± 4.2 years) were assigned to the control group. They all had breast cancer–related lymphedema. All procedures were completed within one session. After baseline measurements were taken, the experimental group performed 18 Forms Tai Chi Internal Qigong for approximately 6 minutes while the control group rested for similar duration in a sitting position. Both groups were then reassessed. All participants were measured on their affected upper limb circumference (by using tape measures), peripheral arterial resistance, and blood flow velocities (using a Doppler ultrasound machine). Results. The between-group differences were not significant for all outcome measures at baseline (P > .05). The circumferences of the affected upper arm, elbow, forearm and wrist decreased after qigong exercise (P < .05). However, no significant difference was found in the circumference measures between the 2 groups posttest (P > .0125). In terms of vascular outcomes, the resistance index decreased and the maximum systolic arterial blood flow velocity (SV) and minimum diastolic arterial blood flow velocity (DV) increased significantly after qigong exercise (P < .05). The between-group difference was close to significant for SV (P = .018) and was significant for DV (P < .001) posttest. Conclusion. Qigong exercise could reduce conventional cancer therapy side effects such as upper limb lymphedema and poor circulatory status in survivors of breast cancer. However, such effects may be temporary, and further studies must be conducted to explore longer term effects.
Keywords
Introduction
Breast cancer is the most common type of cancer among women. 1 Conventional treatments for breast cancer (eg, surgery and radiotherapy) are aggressive and commonly result in many side effects such as chronic lymphedema and altered circulation in the affected upper limb.2,3 These side effects, in turn, present adverse psychological effects (eg, low self-esteem or body image) and functional inconvenience (eg, ill-fitting clothing) to survivors of breast cancer.2,4 It has been reported that 48% to 83% of breast cancer patients or survivors turn to complementary therapies (eg, mind–body exercise and herbal therapy), which they believe can assist them in managing the side effects of conventional cancer treatments such as persistent fatigue and hence improve their quality of life.5-7
Among these complementary therapies, qigong exercise is a rather popular self-help means of relieving the signs and symptoms related to conventional cancer treatments. Qigong is a mind–body integrative exercise originating from traditional Chinese medicine and is used to improve health and energy levels through regular training. 5 A recent review suggested that qigong can improve the microcirculation of fingernails in cancer patients. 8 Moreover, the upper limb movements during qigong exercise resemble the physiotherapeutic exercises used to reduce postsurgical lymphedema in breast cancer patients and survivors. 9 Therefore, we postulate that qigong may be a potentially beneficial exercise for survivors of breast cancer and could be used to regulate upper limb blood flow and decrease lymphedema. However, to our knowledge, there is no available evidence to inform health care professionals and patients of qigong’s efficacy in relieving the surgical side effects of breast cancer. Therefore, this study aimed to (a) investigate the immediate effects of qigong exercise on upper limb lymphedema, arterial resistance, and blood flow velocity in women with breast cancer and mastectomy and (b) explore whether the immediate effects of qigong exercise were related to the demographic and baseline characteristics of the participants.
Methods
Study Design
This study was conducted as a single-blinded non-randomized controlled trial. The assessor was blinded to the group allocation of the participants.
Sample Size Calculation
A previous study of postmastectomy patients showed that exercise training can result in a reduction of upper limb circumference, with reported effect sizes ranging from 0.16 to 2.46. 9 Moreover, based on a participant sample size of 15, Lu et al 10 reported that 16-week tai chi training in female seniors can result in significant improvement in arterial compliance, with an effect size of 0.80. In light of the existing scientific evidence, a medium to large effect size of 0.7 was expected for this study. Therefore, a total sample of 19 participants was necessary to achieve 80% power with an α value of 5%. Attrition was not anticipated because the pre- and postassessments were conducted within the same session (30-minute duration). As a result, the minimum sample size required for each group was 10.
Participants
All qigong participants were recruited from the Hong Kong Wushu & Art Service Centre, which provides qigong training classes for survivors of cancer, and the control participants were recruited from breast cancer self-help groups in the community. The inclusion criteria were as follows: the participants (a) had a history of breast cancer; (b) had a history of mastectomy with or without adjuvant chemotherapy/radiotherapy; (c) had completed conventional treatments of breast cancer and were medically stable; (d) had lymphedema, defined as a circumference difference greater than 2 cm at any point between the surgical-side upper limb and the contralateral upper limb 11 ; (e) had no known neurological deficit resulting from breast cancer treatment; (f) were Chinese females; and (g) were 18 years or older. Participants were also required to have trained in qigong for at least 6 months (3 training sessions per week, 1 hour per session) and be able to perform 18 Forms Tai Chi Internal Qigong independently. Participants were excluded if they (a) had significant neurological, musculoskeletal, cardiovascular, peripheral vascular, or kidney disorders; (b) received chemotherapy, radiotherapy, oral medication such as diuretics, acupuncture, herbal therapy, or other cancer treatments during the study period; (c) had recurrent breast cancer or cancer in another organ during the study period; (d) did regular exercises other than qigong; (e) were smokers; (f) received lumpectomy but not mastectomy; or (g) were pregnant during the study period.
Written informed consent was obtained from all eligible participants before the trials commenced. This study was approved by the administering institute, and all experimental procedures were conducted in accordance with the Declaration of Helsinki on human experiments.
Procedures and Qigong Exercise Program
Participants in the experimental group were qigong practitioners. The qigong style they learned is known as 18 Forms Tai Chi Internal Qigong, which is quite popular among Chinese cancer patients and survivors. It is a kind of physical and mental exercise (internal qigong) that focuses on relaxation, deep breathing, and slow and coordinated movements and uses the mind to guide these movements. There are a total of 18 upper and lower body movements, and all of the techniques are performed while either standing or semisquatting. 12 Details of this qigong form can be found in a book by Mak. 12 After the baseline assessment, an individual qigong practice session was initiated immediately and continued for about 6 minutes. Each participant in the qigong group performed 18 Forms Tai Chi Internal Qigong once and was assessed immediately afterward in sitting (to measure the vascular outcomes) and lying (to measure the upper limb circumference) positions. The control participants were given no specific exercise instruction after the baseline assessment. Instead, they were asked to rest (sit quietly in the laboratory) for 6 minutes and then participated in the postassessment directly.
Outcome Measurements
All assessment procedures took place in the Sports Training and Rehabilitation Laboratory at the Hong Kong Polytechnic University. The room temperature was set at 22°C. All procedures were standardized and conducted by a physiotherapist (who was blind to the subject group and responsible for all physical measurements) and a research assistant (who was responsible for the face-to-face interviews).
Demographic Data
Height and weight were measured to the nearest 0.1 cm and 0.1 kg, respectively, using the Health O Meter (Continental Scale Corp, Bridgeview, IL). Other relevant information (eg, gender, side of breast cancer, postmastectomy duration, and qigong experience) was obtained via face-to-face interview.
Upper Limb Circumference
Participants were instructed not to wear the elastic compression sleeve 1 day before the test and to avoid caffeinated drinks 8 hours before. During the test, participants lay prone with their arms alongside their trunks. The circumferences of both arms that represented the participants’ lymphedema status were taken at the level of (a) 10 cm proximal to the lateral epicondyle; (b) the elbow joint, right at the lateral epicondyle; (c) 10 cm distal to the lateral epicondyle; and (d) the wrist joint, just distal to the ulnar styloid process. 13 The upper limb circumferences were measured with a cloth measuring tape. Care was taken to avoid any slack or constriction of soft tissues by the tape. The difference in each circumference measurement between the ipsilateral and contralateral arms was calculated to detect a 2 cm between-side difference (ie, to fulfill the inclusion criterion). Only the affected side was measured twice, and the mean of the 2 girth measurements (at the 4 levels) was used for analysis. The interlimb girth difference was not used in the analysis because (a) some of our participants received bilateral mastectomy (ie, both upper extremities were involved), (b) qigong is a whole-body exercise that might have had generalized circulatory effects on both the affected and nonaffected upper limbs, 12 and (c) it is impossible to know if the cancer treatments such as radiotherapy and chemotherapy had any effect on the uninvolved arm. 14
Arterial Resistance and Blood Flow Velocities of the Affected Upper Limb
These outcome parameters reflect the circulatory status of the upper limb. They were measured at the resting state, during which each participant sat quietly on a chair with the assessed forearm supported on a plinth at about heart level. The peripheral arterial blood flow velocities during systole and diastole were assessed by a Doppler ultrasound machine (Sonovit SV-30, Schiller AG, Switzerland). The radial artery was selected because it is superficial and relatively parallel to the skin surface. 15 Measurements were made in the distal radius region, where the radial artery pulse could be palpated easily. The ultrasound transducer (probe), operating at 8 MHz, was fixed at 45° relative to the arterial axis and was opposite to the direction of blood flow. Ultrasound gel was applied between the probe and skin surface to facilitate ultrasound wave transmission. A real-time continuous display of the maximum systolic and minimum diastolic Doppler frequencies was monitored and documented when the values became stable over 4 consecutive Doppler waveforms.16,17 The maximum systolic and minimum diastolic Doppler frequencies were then fitted into the following Doppler equation to calculate the maximum systolic arterial blood flow velocity (SV) and the minimum diastolic arterial blood flow velocity (DV):

where FD can be the maximum systolic or minimum diastolic Doppler frequency, fo is the transducer frequency (8 MHz), v is either the maximum systolic or minimum diastolic arterial blood flow velocity depending on the FD, θ is the Doppler angle (45°), and c is the ultrasound velocity in the blood (1.54 × 105 cm/s). 18 Both the SV and DV were used in the analysis.
Apart from blood flow velocities, another outcome parameter representing peripheral blood flow resistance, that is, the resistance index (RI), was also documented. It was derived from the following equation:

An RI of 0 corresponds to continuous blood flow (little blood flow resistance) whereas an RI of 1 corresponds to systolic blood flow only (no diastolic blood flow; large blood flow resistance). 19
The Doppler ultrasound machine used in this study was validated and its reliability was checked by measuring the velocity of a starch solution flowing through a thin rubber tube16,17 before the actual test. The test–retest reliability of the flow velocity was found to be good (ICC3,1 = .76). 20
Statistical Analysis
Independent t tests were used to compare the demographic characteristics of the qigong and control participants. In our primary analysis, a 2-way repeated-measures multivariate analysis of covariance was performed, incorporating all the outcome measures within a specific domain (ie, girths of the upper arm, elbow, forearm, and wrist within the upper limb circumference domain and SV, DV, and RI within the arterial blood flow domain). The purpose was to test the overall effect of qigong exercise and to reduce the probability of committing a type I error due to multiple comparisons. The between-subject factor was group and the within-subject factor was time. The baseline outcome measures were entered as covariates if any significant between-group difference existed at pretest. The intention-to-treat principle was implemented in any dropout cases. Effect sizes (partial η2) were presented for all outcome measures. By convention, partial η2 values of 0.14, 0.06, and 0.01 are considered large, medium, and small effect sizes, respectively. 21
If the multivariate analysis of covariance demonstrated a significant effect overall, follow-up analyses using independent t tests (to detect between-group differences) and pairwise t tests (to detect within-group differences between the 2 time points) were carried out. The significance level was set at .05 (2-tailed) for all tests and corrected using an appropriate Bonferroni adjustment to maintain an overall type I error at 5% (ie, α = .0125 for comparisons of the girth outcomes, and α = .017 for comparisons of the arterial blood flow outcomes between the 2 groups).
A secondary data analysis was also performed to further explore whether the effects of qigong exercise were related to age, postmastectomy duration, and the baseline values of the outcome measures. For each outcome variable, a change score was calculated by subtracting the pretest score from the posttest score. The association between the change score of each outcome variable and the baseline characteristics of the participants was determined using a Pearson product–moment correlation coefficient (Pearson’s r; α = .05). All statistical analyses were performed using the Statistical Package for Social Sciences 20.0 software (IBM SPSS Inc, Chicago, IL).
Results
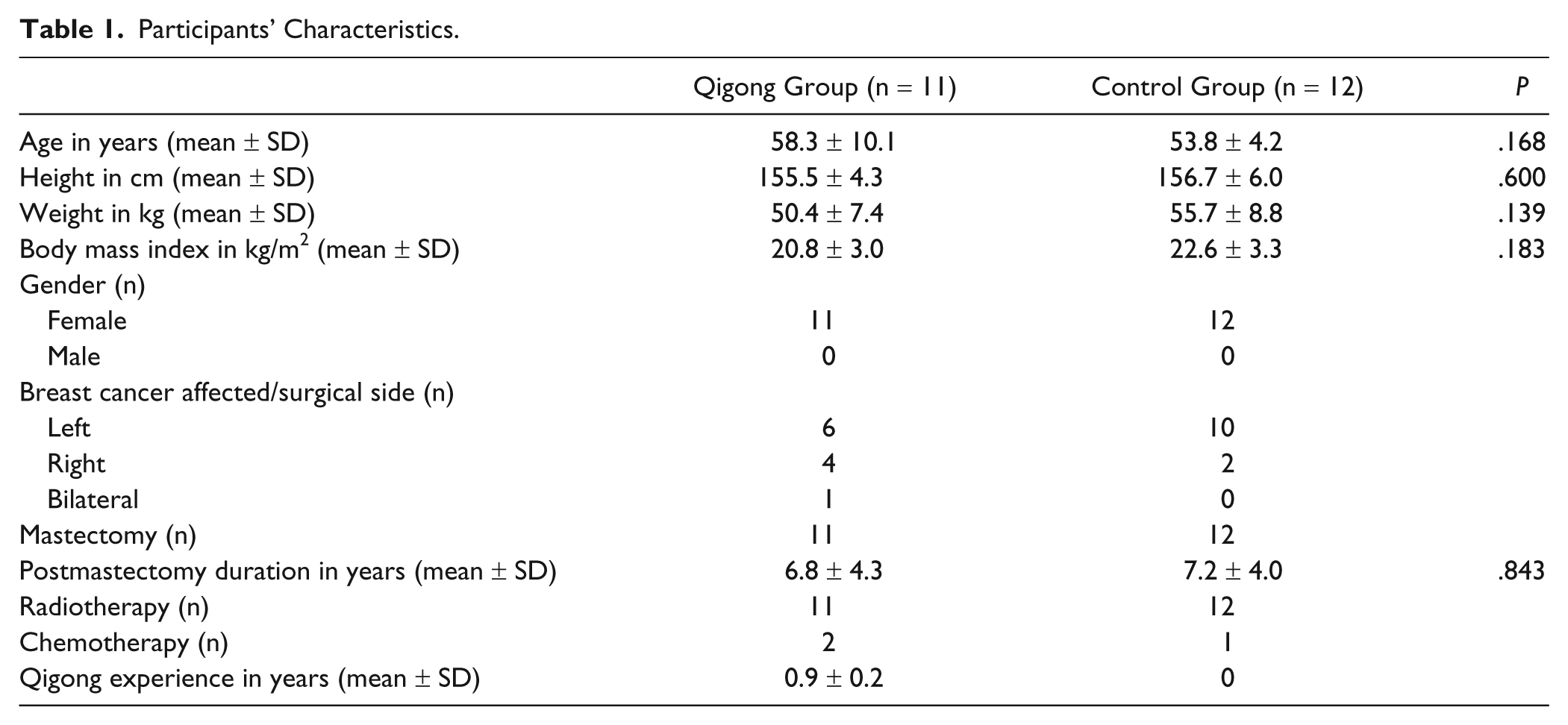
A total of 23 survivors of breast cancer with a history of mastectomy (11 qigong practitioners and 12 control participants) volunteered to participate in the study. All participants fulfilled the inclusion and exclusion criteria. Their demographic characteristics are presented in Table 1. No difference was identified in any of the demographic (Table 1) or outcome (Table 2) variables between the 2 groups at pretest. Thus, no covariate was added in the multivariate analysis. All participants completed the study within 1 visit. As there were no dropouts, an intention-to-treat analysis was not necessary. Moreover, no participants reported any adverse effects during qigong exercise.
Participants’ Characteristics.
Outcome Measures.

P < .05.
Within group: P < .05 when compared with preexercise values.
Between groups: P < .017 when compared with the control group.
Upper Limb Circumference
The group-by-time interaction effect was significant for all girth outcomes (P < .05) except elbow girth (Table 2). The independent t tests revealed no significant differences between the 2 groups on any of the girth variables at either pretest or posttest (P > .0125). However, girths of the affected upper arm, elbow, forearm, and wrist decreased by 4.1%, 3.1%, 3.9%, and 2.7%, respectively, after qigong exercise (P < .05) in the experimental group. On the contrary, girths slightly increased in the affected upper arm (1.6%) and forearm (1.9%) in the control group (P < .05) at posttest. Girths measured at the elbow and wrist joints did not change over time (P > .05; Table 2).
Arterial Resistance and Blood Flow Velocities in the Affected Upper Limb
Significant group-by-time interaction effects were identified for all vascular outcomes (P < .05). The RI decreased and arterial blood flow velocities increased significantly over time in the qigong training group compared with the control group. The RI dropped significantly by 33.3% (P = .002) after qigong exercise and became significantly different from the control group at posttest (P < .001). The RI of the control participants remained the same over time (P > .05). The qigong-trained participants notably demonstrated no difference in RI compared with the control participants before they performed the qigong exercises (P > .017; Table 2).
Dramatic increases in the maximum systolic arterial blood flow velocity (SV; 36.8%, P = .009) and minimum diastolic arterial blood flow velocity (DV; 54.5%, P = .001) were noted immediately after qigong exercise. No change was observed in the control group over the 2 test periods (P > .05). The between-group differences were not significant (P > .017) before qigong exercise but were close to significant for SV (P = .018) and significant for DV (P < .001) at posttest (Table 2).
Associations Between the Change Scores and Demographic and Baseline Variables
In the secondary data analysis, none of the change scores (ie, postscore/prescore) were correlated with age or postmastectomy duration (P > .05). Among the outcome measures, only the change scores for the maximum systolic (r = −0.655, P = .001) and minimum diastolic arterial blood flow velocities (r = −0.548, P = .007) had significant negative correlations with their respective baseline values. This indicated that participants with slower blood flow velocities at baseline tended to have greater blood flow velocity increases (during both systole and diastole) after qigong exercise.
Discussion
To our knowledge, this is the first study to evaluate the effects of qigong exercise on upper limb blood flow status and circumference (lymphedema) in postmastectomy females. In terms of vascular outcomes, our results revealed that blood flow resistance decreased and that there was a concomitant increase in blood flow velocities in the radial artery of the affected upper limb immediately after qigong practice. The decreases in peripheral blood flow resistance could be mainly attributed to 2 factors: decreases in vascular resistance and compliance, defined as the change in volume of a vessel with a change in pressure. 16 Because vascular compliance is affected by long-term alterations in blood pressure, age, medications and prolonged aerobic training,10,22,23 it was not likely to change within the study period (<30 minutes). The decrease in blood flow resistance demonstrated by our participants was therefore more likely due to a decrease in vascular resistance following qigong exercise. Why qigong exercise promptly decreased the vascular resistance of the affected upper limb remains in question. It could be explained by the qigong psychoneuroimmunology theory, which states that qigong training can integrate hypothalamic responses, resulting in the homeostasis of the sympathetic and parasympathetic nervous systems. 24 This could better regulate the vasoconstriction and vasodilation of the peripheral arteries, resulting in increased or decreased vascular resistance as necessary to maintain homeostasis. 25 Our secondary analysis indeed showed that participants with slower blood flow velocities at baseline (presumably because of higher vascular resistance) tended to experience greater increases in blood flow velocity (greater decreases in vascular resistance) after qigong exercise.
This study demonstrated that with a decrease in vascular resistance, blood flow velocities (during both systole and diastole of the heart) at the distal part of the affected upper limb increase drastically after qigong exercise. Our findings concurred with a previous study published in China. 26 Using a sample size of 19, Shen and Gao 26 reported that blood flow in the fingernail wrinkles accelerated after qigong exercise. The authors proposed that qigong therapy could adjust the microcirculatory function to an optimal state by accelerating blood flow. This may in turn increase the blood and oxygen supply to the tissues and cells, strengthen metabolism and return the body to a normal physiological state.26,27 This postulation is positively inclined and requires confirmation by further rigorous study. Nevertheless, evidence supports that qigong exercise could improve circulation in the distal parts of the upper extremities in survivors of breast cancer. However, the effect may be temporarily as blood flow velocities were similar between the qigong group and control group prior to qigong exercise (at resting state).
In spite of an old belief (lacking scientific support) that upper limb exercises increase blood flow and lymph production and thus lead to an increase in upper limb volume,28-30 increased upper limb circumference was not observed in our participants with an accelerated blood flow after qigong practice. Instead, arm circumference decreased by 2.7% to 4.1% postexercise. Our findings were in agreement with some previous studies.9,31,32 For example, Moseley et al 32 found that upper limb volume decreased by 5.8% immediately after 10 minutes of gentle arm and deep-breathing exercises in women with secondary arm lymphedema. To summarize, current scientific evidence suggests that a short period of upper limb exercises together with breathing exercises (eg, tai chi qigong exercise) could reduce arm circumference, volume, and very likely lymphedema in survivors of breast cancer.
There are several possible explanations for decreasing arm volume or circumference. First, qigong exercise may enhance lymphatic flow from distal to proximal because intrathoracic pressure is decreased during inspiration. 33 Second, it may also improve protein resorption. 34 Third, the gentle stretching movements involved in qigong exercise may reduce soft tissue contractures and so decrease obstruction in the upper limb venous and lymphatic systems. 33 Fourth, skeletal muscle contraction further enhances lymphatic clearance by propelling lymph fluid throughout the lymphatic vessels (ie, the pumping mechanism) 35 and stimulates the contraction of lymph vessels by resetting the sympathetic drive. 36 Indeed, from a physiological standpoint, increased blood flow velocity in the peripheral arteries could assist lymphatic return. Milking the lymph proximally along these valved vessels (lymphatic clearance) is possible because the deep lymphatic vessels would be compressed by their accompanying arteries when the arteries expand during systole of the heart. 15
In some contrast to our positive findings, Johansson et al 37 reported an increase in total arm volume immediately after upper limb exercises. This discrepancy could be because of the involvement of resistance training (lifting weights) in their exercise program, whereas our qigong exercise involved resistance-free active upper limb movements together with breathing control. 12 Further study is necessary to confirm the optimal training elements in such cancer rehabilitation programs. Qigong exercise may be more suitable than resistance exercises for survivors of breast cancer.
We also found that qigong practitioners and control participants showed no difference in girth outcomes prior to qigong exercise despite the qigong group having trained in qigong for about a year. This may hint that the immediate beneficial effects of qigong exercise may not sustainable over the long term. Indeed, some studies have reported that months of upper limb exercises had no significant effect on upper limb circumference in survivors of breast cancer.36,38,39 It is possible that these studies did not measure arm circumference immediately after exercise and therefore missed the short-term effects of exercise training. Moreover, our participants’ qigong training period (mean = 0.9 ± 0.2 years) might not have been long enough to elicit any long-term effects. Further study may fruitfully explore the qigong training threshold and investigate whether the benefits can be sustained over the longer term with continuous qigong practice.
Although the results of this study were quite promising, several limitations should be noted during their interpretation. First, our study population was quite heterogeneous in relation to their breast cancer diagnoses (eg, tumor staging) and treatment. Some of the participants could not recall the exact type of surgery (eg, mastectomy with or without axillary clearance) they had received, and the onset of lymphedema was unknown. We were also unable to retrieve their medical records. All of these factors may confound the results. Second, we used circumference measures to represent lymphedema instead of measuring the change in arm volume. Although circumference measures are correlated with a change in arm volume, arm volume measures may be more accurate and sensitive to change. 40 Third, this was a nonrandomized trial with a rather small sample size. The experimental group participants were volunteers that had prestudy qigong experience. Therefore, a self-selection bias and between-group variability (eg, different general physical fitness) at baseline might have existed. Nevertheless, the pretest values of all outcome variables were similar between the 2 groups. This pilot work definitely needs to be confirmed in future randomized controlled studies using larger samples. Further studies may also examine the associations between vascular status, lymphedema, and quality of life in survivors of breast cancer.
To summarize, the findings of this study provided preliminary evidence that qigong exercise is effective in improving circulatory status and limb circumference (lymphedema) in survivors of breast cancer. Physicians could advise former breast cancer patients on the potential benefits of qigong training. Moreover, our secondary analysis revealed that postmastectomy duration and age were not associated with the effects of qigong exercise. This means that survivors of breast cancer can start qigong training at any time and age and would still be able to gain the immediate benefits of improving blood flow velocities and decreasing affected limb circumference (lymphedema). However, these benefits may not be sustainable over a long period, and repeated practice of the qigong form may be necessary.
Conclusions
Qigong exercise could reduce the side effects of conventional cancer therapy such as upper limb lymphedema and poor circulatory status in survivors of breast cancer. However, such effects may be temporary and further studies are required to explore the longer term effects.
Footnotes
Acknowledgements
We would like to thank the Hong Kong Wushu & Art Service Centre for their recruitment of the participants and for providing free qigong training sessions, Dr. William Tsang for his advice on the abstract, and Mr. Ken Lee for his advice on oncology rehabilitation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.