
Abstract
Hypotheses. This study hypothesized that non-Hodgkin lymphoma (NHL) patients who used complementary and alternative medicine (CAM) would have higher health-related quality of life (HRQOL) and a greater perceived sense of control than nonusers. However, since CAM may predict HRQOL, and perceived control may be both associated with CAM use as well as being an independent predictor of HRQOL, the authors also sought to test whether perceived control mediated the relationship between CAM use and HRQOL. Study design. This was a cross-sectional study design. NHL survivors diagnosed between June 1, 1998 and August 31, 2001 were selected from the population-based SEER (Surveillance, Epidemiology, and End Results) cancer registry for Los Angeles County and were mailed a survey in 2003 that assessed CAM use and predictors of CAM use. The response rate was 54.8%; 319 provided complete data for analysis. Methods. Categories of CAM were defined according to the National Center for Complementary and Alternative Medicine guidelines. The authors measured survivors’ cancer-related control using the Perceived Personal Control scale, a 4-question scale that was adapted from previously validated scales. HRQOL was measured using the mental component summary and physical component summary scores from the SF-36 v2.0. Bivariate and multivariable logistic and linear regression models were used to assess factors associated with CAM use and the association of CAM use with psychosocial health outcomes, respectively. Results. Sixty-one percent of respondents reported using at least one CAM modality within the past 4 weeks, and 40% did so after excluding personal prayer and support groups. Younger age and higher education were significantly associated with greater CAM use as were higher perception of cancer-related control (P = .004) and more positive mental functioning (P = .016). Perception of control significantly mediated the association between CAM use and mental functioning (P < .001). Conclusions. CAM use may be related to more positive mental health–related quality of life by increasing patients’ perception of perceived control over their health; however, cause and effect cannot be determined. Physicians should be aware that cancer survivors have a need to take an active role in improving their health.
Keywords
Introduction
There are an estimated 12 million cancer survivors in the United States. 1 Studies of the survivorship experience are critical to understanding the needs and care requirements for these patients. One area that is receiving increasing attention is use of complementary and alternative medicine (CAM) by cancer survivors. Recent studies have indicated that the use of CAM is widespread and is increasing among survivors. 2 However, many of these studies have been limited to breast cancer, or have included a mixed sample of multiple cancers, and have not focused specifically on non-Hodgkin lymphoma (NHL), which has had an increase in both incidence and survival and is the sixth most common cancer among men and fifth most common among women in the United States. 3 With the exception of one small pilot study, 4 the use of CAM among NHL survivors has not been previously reported. Furthermore, there are no studies that have examined the relationship between CAM use and health-related quality of life (HRQOL) in adult survivors of NHL, which has been shown to be poor. 5
From previous studies, cancer survivors have been reported to use CAM to alleviate symptoms, improve their HRQOL, and enhance perceptions of control over their therapy, decision making, and course of illness.4,6-13 We obtained CAM-related data as part of a population-based study of NHL survivors that was designed to assess NHL survivors’ use of follow-up care and evaluate their long-term health outcomes. 14 Since the study also obtained measures of HRQOL, perceived control, and other psychosocial measures it provided the opportunity directly assess their relationship to use of CAM.
Despite the finding that patients may use CAM to improve their quality of life, previous studies with breast and other cancer survivors have shown that patients with lower quality of life were more likely to use CAM.15,16 However, within the context of a self-help model, it was found that CAM use was minimally effective in improving quality of life, but those who used CAM as a type of self-care had higher quality of life scores. 17 Thus the use of CAM by patients could be related to having a sense of control over their cancer and this may be the mechanism by which CAM use could be associated with improving quality of life. We hypothesized that NHL patients who used CAM would have higher HRQOL (at 2-5 years after diagnosis) and a greater perceived sense of control. However, since CAM may predict HRQOL, and perceived control may be both associated with CAM use as well as being an independent predictor of HRQOL, we also sought to test whether perceived control mediated the relationship between CAM use and HRQOL.
Methods
Case Selection
The study methods used to select the sample of NHL cases, administer the questionnaire, and assess response have been previously described.14,18 Briefly, survivors were eligible for the study if they (a) were diagnosed with aggressive NHL (intermediate and high grade) between June 1, 1998 and August 31, 2001 (ie, 2-5 years prior to enrollment in the study in 2003) and were identified through the Los Angeles Cancer Surveillance Program, the SEER (Surveillance, Epidemiology, and End Results) cancer registry for Los Angeles County; (b) were diagnosed at age 20 years or older; (c) were Los Angeles county residents at the time of diagnosis; (d) were alive at the time of the study; and (e) had no other cancer within a year prior to their NHL diagnosis or in the time period between their NHL diagnosis and the start of the study.
Selected patients were initially sent a study questionnaire by mail and asked to complete it and mail it back in a postage paid envelope. Extensive telephone contact was used to increase response. After contact with the patient, we also excluded those who were unable to speak English. For survivors who were unwilling or unable to complete the study questionnaire by mail, we conducted a telephone interview with a subset of the questionnaire items. A total of 744 questionnaires were mailed to eligible NHL survivors and 408 participated, for an overall response rate of 54.8%. In comparison with the total eligible sample, the nonrespondents who were categorized as lost because they were unable to be contacted because of incorrect addresses and telephone numbers were more likely to be younger, male, and Hispanic; however, those who refused participation did not differ by any sociodemographic or clinical factors from those who responded. 14 Among the 408 respondents, 89 were omitted from this analysis because they participated by telephone interview and were not asked the questions concerning CAM, leaving 319 respondents with complete data. There were no significant differences in age, race/ethnicity, or gender between the mail and telephone respondents. The study was approved by the Institutional Review Board at the University of Southern California.
Definition of Variables
CAM use
Survivors were asked about use of specific types of CAM during the entire time since their diagnosis as well as during the 4 weeks prior to completing the questionnaire. The latter definition was used in these analyses to be consistent with the reference time frame of psychosocial outcome variables. The respondents were asked if they had used any of 10 types of CAM that have been grouped into 5 major categories based on definitions that were consistent with the National Center for Complementary and Alternative Medicine (http://nccam.nih.gov/health/whatiscam/): biologically based therapies (“special diets such as mostly vegetarian or low fat” or “high dose or mega vitamins [not including 1-a-day multivitamins], nutritional supplements, or herbal remedies”); mind–body intervention (“mind/body therapies such as guided imagery/visualization, biofeedback, meditation, relaxation techniques, hypnosis/hypnotherapy, energy healing, therapeutic touch, or music therapy,” “faith healing, laying on of hands, or any other spiritual or religious group experience,” or “self-help or support groups [either face-to-face or on the Internet]”); manipulative and body-based methods (“movement or physical therapies such as yoga, tai chi, massage, chiropractic, or electromagnetic therapy”); and alternative medical systems (“homeopathy,” “oriental therapies such as acupuncture, acupressure, Qigong, or Shiatsu”). Since many studies have also included personal prayer as a type of CAM,19-21 we also obtained information on this practice (“personal prayer or personal spiritual healing”). Support groups have been both included as a type of CAM 22 and studied as a predictor of CAM use. 23 Thus, we created 2 definitions of overall CAM use, first including and second excluding use of personal prayer and support groups.
Patient characteristics
The following self-reported sociodemographic variables were used (with the specific categories defined in Table 1) gender, age at diagnosis, race/ethnicity, marital status, education, household income, and health insurance coverage.
Selected Characteristics of Aggressive Non-Hodgkin Lymphoma Survivors, 2 to 5 Years Postdiagnosis and Proportion Using CAM Within the Past 4 Weeks (Excluding Prayer and Support/Self-Help Groups): ECHOS-NHL Study

Abbreviations: CAM, complementary and alternative medicine; ECHOS-NHL study, Experience of Care and Health Outcomes of Survivors of Non-Hodgkin Lymphoma.
CAM defined as any CAM use in past 4 weeks excluding prayer and support/self-help groups.
Numbers may not total 319 because of missing data.
Percentages may not total 100% because of rounding.
P < .05 for differences in percentage using CAM in past 4 weeks by categories of variable.
Clinical variables
We included self-reported cancer treatment (chemotherapy with and without radiation, bone marrow/stem cell transplant), recurrence, and comorbidities occurring either before or after lymphoma diagnosis (none, 1-2, or 3 or more of the following: heart failure/attack, chest pain or angina, high blood pressure, blood clots in the veins of the legs or in the lungs, stroke or brain hemorrhage, chronic lung disease, liver disease, bowel disease, diabetes, osteoporosis, arthritis, depression or anxiety). Using SEER cancer registry variables, we calculated time since cancer diagnosis in years (2.0-2.9, 3.0-3.9, 4.0-5.9) and NHL grade (intermediate or high, based on ICD-O-2 histology).
Psychosocial health variables
Social support was measured by a 12-item scale that had been previously validated.24,25 We measured survivors’ cancer-related control using the perceived personal control scale (PPC), 26 a 4-question scale that was adapted from previously validated scales.27,28 The responses to the 4 questions ranged from 1 = no control at all to 5 = complete control. The specific topics in the 4 questions included (a) your emotional responses to cancer, (b) the physical side effects of your cancer and its treatment, (c) the kind of follow-up care you receive for your cancer, and (d) the course of your cancer (ie, whether your cancer will come back, get worse, or you will develop a different kind of cancer). Cronbach’s α was .71. Scores on the social support and perceived control scales were linearly transformed to a 0 to 100 scale such that a higher score represented more social support and greater perceptions of control. Optimism was measured by the Life Orientation Test-R (LOT-R), 29 which includes 6 statements related to optimism such as “In uncertain times, I usually expect the best.” The respondent is asked to indicate how much they agree with the statement using a 5-point scale. The 6 items on the LOT-R were summed to have a maximum possible range of 6 to 30 where a higher score represented greater optimism. To provide comparison to patients with other cancers as well as to those with other chronic conditions or those in the general population, HRQOL was measured using the mental component summary (MCS) and physical component summary (PCS) scores from the Short-Form Health Survey–36 (SF-36) v2.0.30,31 The MCS and PCS were scored on a T-score metric such that a mean of 50 represented the average score in the general US population, and the standard deviation was 10.
Statistical Methods
Correlates of CAM use
A bivariate P value of .10 or less with at least one measure of CAM use was the criterion used for inclusion as a covariate in multivariable models that examined the correlates of specific and overall CAM use. Bivariate comparisons were made using χ 2 tests (and Fisher’s exact test when cell sizes were ≤5) and 2 sample t tests. Variables tested in bivariate analyses but not included in multivariable models due to lack of significance were income, health insurance, social support, time since diagnosis, recurrence, comorbidity ever or since lymphoma diagnosis, NHL grade, currently taking medication or having received treatment for cancer in the past 6 months, satisfaction with doctor, and quality of care. Only 19 participants had used alternative medical systems (ie, homeopathy or oriental therapies) in the past 4 weeks so we did not estimate a separate multivariable model for this outcome measure.
CAM use and psychosocial health outcomes
We used multiple linear regression to examine the association between specific and overall CAM use as predictors of psychosocial outcome variables (MCS, PCS, and perceived control). In all models, we adjusted for a common set of potential confounders (gender, age, race/ethnicity, marital status, education, and optimism) that were significantly (P < .10) associated in bivariate analyses with at least one CAM measure and at least one psychosocial outcome variable.
Mediation analysis
To test whether perceived control mediated the relationship between CAM use and HRQOL we needed to determine whether the following conditions were met, based on Baron and Kenny 32 : (a) the independent variable (CAM) affects the dependent variable (HRQOL); (b) the independent variable (CAM) affects the mediator (perceived control); and (c) the mediator (perceived control) affects the dependent variable (HRQOL) controlling for the independent variable (CAM). A fourth criterion is also suggested—(d) the mediated effect is statistically significant.
To test whether these conditions were met we estimated the 3 following regression equations, where HRQOL was measured by the SF-36 PCS and MCS and CAM use included both specific and overall CAM use: (a) HRQOL regressed on CAM use, (b) perceived control regressed on CAM use, and (c) HRQOL regressed on both CAM use and perceived control. In Figure 1, path a represents model 1, path b represents model 2, and paths c and d represent model 3. We only estimated c and d (model 3) when a and b (models 1 and 2, respectively) were statistically significant. The mediated effect (a − d, or b.c) and its standard error provide a method to test the statistical significance of mediation. The standard error of the mediated effect (a − d) is the square root of (b2S c 2 + c2S b 2 − S b 2S c 2) where S b and S c are standard errors of the regression coefficients b and c, respectively, in Figure 1, which has been previously described. 33 Analyses were limited to those individuals with complete information for all 3 models. All models were adjusted for gender, age, race/ethnicity, marital status, education, and optimism. The number of cases with missing data was small (<8% for any variable); therefore, we used listwise deletion in analyses.

Test of mediation effects
Results
Respondent Characteristics
There were about equal numbers of males and females; 42% were aged 65 years and older, and about two thirds of the respondents were non-Hispanic white (Table 1). Over, 40% had income of less than $40 000, and 29% had no more than a high school degree. A little more than half the sample had received only chemotherapy, whereas another 36% received chemotherapy plus radiation and 11% received a bone marrow/stem cell transplant. About 20% self-reported progression or recurrence, and 25% had experienced 3 or more comorbidities.
CAM Use Within the Past 4 Weeks
Nearly 61% reported use of some type of CAM within the 4 weeks prior to completing the survey (Table 2). The overall prevalence decreased to 39.8% when personal prayer and self-help/support groups were excluded from the definition of CAM. The percentage using CAM, based on this definition, by patient characteristics is shown in Table 1. Respondents who were younger age at time of response (ie <50 years) were more likely to use CAM compared with those 65 years or older and there was also significant variation in use by treatment as those with transplant were the most likely to use CAM.
Percentage Using CAM in the Past 4 Weeks by Type of CAM: NHL Survivors 2 to 5 Years Postdiagnosis (Total N = 319)

Abbreviations: CAM, complementary and alternative medicine; NHL, non-Hodgkin lymphoma.
The proportion excludes missing (n ranges from 7 to 18).
Includes personal prayer or personal spiritual healing but does not include faith healing, laying on of hands, or any other spiritual or religious group experience.
Defined as “movement or physical therapies such as yoga, tai chi, massage, chiropractic, or electromagnetic therapy.”
The proportion of respondents using the specific types of CAM within the past 4 weeks varied from a low of 6% using some type of alternative health system (including Oriental therapies and/or homeopathy) to more than 50% using personal prayer (Table 2). More than a quarter used one or more types of biological based therapies (including special diets and high dose supplements). A fifth used a mind–body intervention (which included faith healing or other religious group experience or a mind–body technique and support groups), and 12.5% used manipulative or body based methods (including yoga, tai chi, massage, chiropractic, or electromagnetic therapy).
Predictors of CAM Use Within the Past 4 Weeks
Based on bivariate analyses, significant variables associated with any CAM use were selected for inclusion in a multivariable logistic regression model (Table 3). After adjusting for the significant factors, younger age remained significantly associated with greater overall use of CAM and for use of specific types. Those aged 50 to 64 years and <50 years were, respectively, 1.88 (95% confidence interval [CI] = 1.02-3.45) and 2.60 (95% CI = 1.37-4.95) times as likely to use any type of CAM within the past 4 weeks (excluding personal prayer and self-help/support groups) compared with those 65 years and older. This trend was strongest for the use of manipulative and body-based methods where those <50 years were 16 times as likely (P < .001) and those aged 50 to 64 years were 8 times as likely (P = .002) to use this form of CAM compared with those 65 years and older. This type of CAM was also 3 times as likely to be used by females as by males (P = .009), the only form of CAM with a significant difference in use by gender. In addition, those with a college degree or higher were over twice as likely to use any type of CAM (excluding personal prayer and support groups), compared to those with a high school degree or less, and higher education was similarly associated with use of biologically based therapies. There was a 10% increased likelihood of using CAM (of all types including prayer and support groups) for each higher increment in the optimism score; however, this variable was not significant for the other CAM categories.
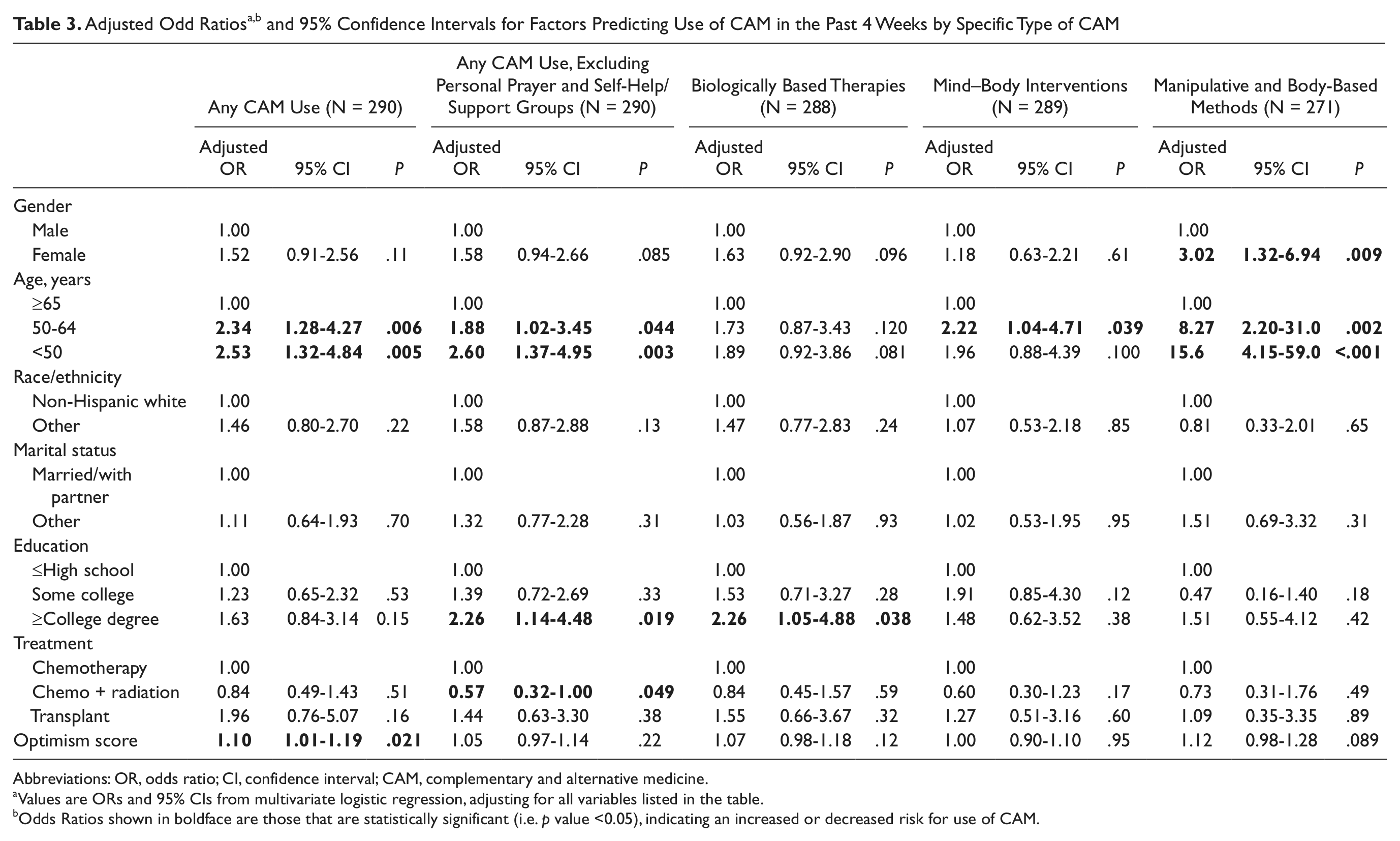
Abbreviations: OR, odds ratio; CI, confidence interval; CAM, complementary and alternative medicine.
Values are ORs and 95% CIs from multivariate logistic regression, adjusting for all variables listed in the table.
Odds Ratios shown in boldface are those that are statistically significant (i.e. p value <0.05), indicating an increased or decreased risk for use of CAM.
CAM Use and HRQOL and Perceived Control
In multivariable analyses, overall CAM use was significantly associated with a higher SF-36 MCS and greater perceived control; however, the SF-36 PCS was not associated with CAM use (Table 4). For CAM use excluding prayer and support groups, the adjusted mean score [standard error, SE] for MCS was significantly higher among individuals who reported using at least one type of CAM (51.7 [0.99]) than among those who did not use CAM (48.7 [0.77]), (B = 3.06, P = .018). Similarly, the adjusted mean [SE] score for perceived control was significantly higher among CAM users (70.6 [1.68]) than among nonusers (63.9 [1.3]), (B = 6.79, P = .002). Although not statistically significant, similar adjusted means were seen for the MCS and specific types of CAM use. In addition, use of mind–body interventions was significantly associated with greater perceived control (P = .001).

Abbreviations: SF-36, short-form health survey; CAM, complementary and alternative medicine; B, unstandardized regression coefficient; SE, standard error.
Values are adjusted for gender, age, race/ethnicity, marital status, education, and optimism.
Adjusted means shown in boldface are those that are statistically significant (i.e. p < 0.05 for difference between CAM users and nonusers)
Mediation Analysis
To evaluate whether perceived control mediated the relationship between CAM use and mental functioning, the MCS score was regressed on both CAM use and perceived control (Table 5). The analyses were limited to any CAM use (using both definitions) and mental functioning (adjusted for gender, age, race/ethnicity, marital status, education and optimism) since these were the only significantly associated variables. A higher perception of control was significantly associated with higher scores for MCS (B = 0.26, P < .001; for both definitions of CAM). Once perceived control was included in the model, the regression coefficient for CAM use decreased (compared with the coefficient obtained from model without perceived control, see Table 4) and was no longer significant. Additionally, we estimated that the mediated effect was statistically significant for both definitions of CAM.
Mediation of the Relationship Between Use of CAM in the Past 4 Weeks and Health-Related Quality of Life by Perceived Control a
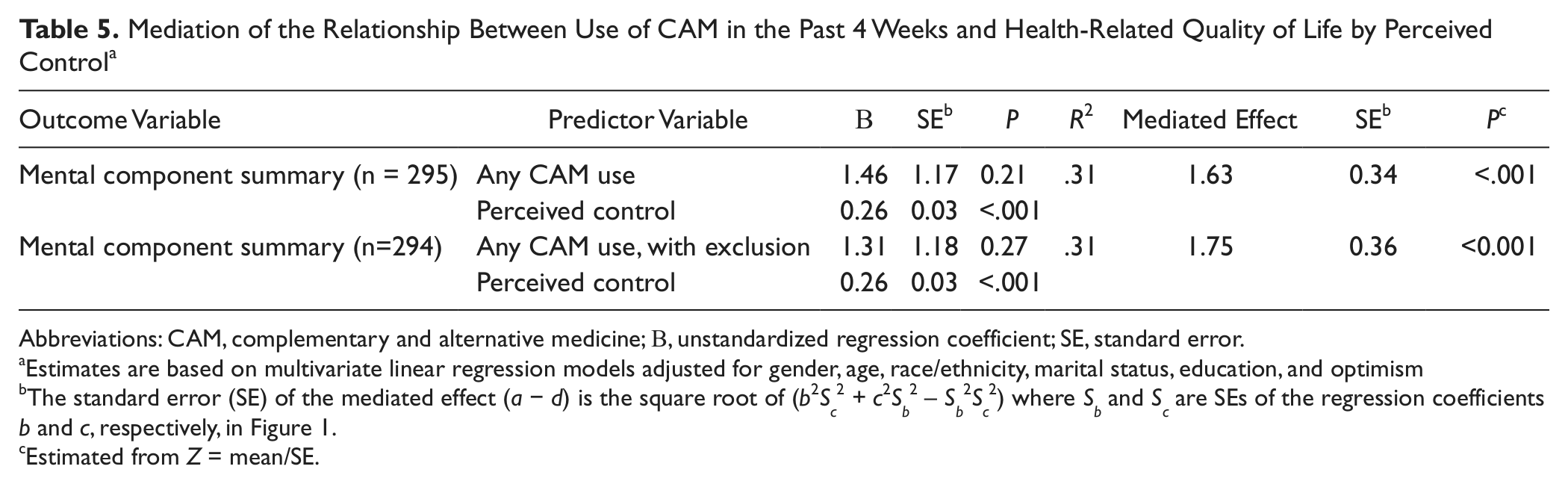
Abbreviations: CAM, complementary and alternative medicine; B, unstandardized regression coefficient; SE, standard error.
Estimates are based on multivariate linear regression models adjusted for gender, age, race/ethnicity, marital status, education, and optimism
The standard error (SE) of the mediated effect (a − d) is the square root of (b2Sc2 + c2Sb2 − Sb2Sc2) where Sb and Sc are SEs of the regression coefficients b and c, respectively, in Figure 1.
Estimated from Z = mean/SE.
Discussion
This is the first study to assess CAM use and its relationship to HRQOL in a large population-based sample of 2- to 5-year survivors of aggressive NHL. Our findings that close to 61% of NHL survivors report using some type of CAM within the past 4 weeks and 40% report using CAM, excluding prayer and support groups, are quite similar to results for US adults reported by the 2002 US National Health Interview Survey where 62% of adults 18 years and older reported any CAM use, including prayer and 36% used CAM, excluding prayer. 34 A population-based study of cancer patients and those with other chronic conditions in California who participated in the California Health Interview Survey in 2003 found that 57.9% of cancer patients and 56.3% of those with other chronic conditions reported seeing at least one provider of CAM. 35 In this latter study, more than 58% of cancer patients used personal prayer as did 50% of those with other chronic conditions, comparable to our finding of 52.2% using prayer. These comparisons suggest that overall use of CAM among NHL cancer patients may not differ substantially from other cancer patients or those with other chronic conditions.
Comparison with other studies of CAM use among NHL patients is limited to a recent pilot study 4 of 56 lymphoma patients surviving 5+ years that included both Hodgkin lymphoma and NHL patients, which found that 68% of the respondents used CAM; however, prayer was mentioned by just 7%. The specific types of CAM use were distributed differently than the pattern we found, potentially because of different questionnaire designs and the different sociodemographic and clinical characteristics of the samples. A higher percentage were found to use chiropractic services and massage compared with our study and the California Health Interview Survey also found higher percentages using these services than we did as well. 35 Thus it is possible that we may have underestimated use of these specific therapies.
We focused our analyses on use of CAM during the 4-week period before completing the survey to assess the relationship between CAM and HRQOL as measured by the SF-36 mental and physical summary scores and other psychosocial variables, which also pertained to this 4-week period of time, including measures of optimism and cancer survivors’ perceptions of control over their cancer. Whereas other studies have found that cancer survivors say they use CAM to increase their sense of control over their disease,4,11,12,36 we were able to measure their perception of control independently from their use of CAM. We did not find a significant association between CAM use and the physical component summary score. Although we initially found the relationship between CAM use (with or without including prayer) and a higher mental functioning score to be statistically significant, the size of the difference between users and nonusers was less than 10% of the total scale, and would not be considered to be a clinically meaningful difference, according to some definitions. 37 In addition the relationship between CAM use and mental functioning was significantly mediated by perceived control such that CAM use and mental functioning were no longer significantly associated once perceived control was included in the multivariable model. This finding, which implies that efforts to give cancer patients a better sense of control over their disease may have important implications for improving quality of life, is a significant contribution to our understanding of the role CAM may be playing in the cancer survivor’s life.
The results are supportive of findings from a previous study of breast cancer in Hispanic women in which CAM use was higher in women who had higher enabling skills and problem solving abilities. 17 CAM, as a type of self-care, was associated with a higher quality of life in women with these abilities. Similar to findings for other groups of cancer survivors,7,12,38 we found being younger and more educated were variables associated with CAM use in NHL survivors. It is likely that these patients have greater capabilities to assert control over their care through use of CAM and other methods and experience improvement in mental functioning as a result. However, this study and others are cross-sectional studies from which causality cannot be inferred.
Other limitations of the study included the restriction to 2- to 5-year NHL survivors from Los Angeles who responded to the survey and who were able to speak English; thus, generalization to shorter or longer term survivors or to survivors from other regions of the country or to those who were non-English speakers is not possible. In addition, those in the original sample who were unable to be located were more likely to be younger, male, and Hispanic; thus the final sample may not be representative of these subgroups. However, these variables are controlled for in the multivariable models. The lack of detail on the questionnaire regarding use of specific types of CAM within the larger categories may have resulted in an underestimation of the prevalence of some subtypes of CAM.
Conclusions
Despite lack of definitive evidence of the effectiveness of many CAM options,36,39,40 cancer patients (as well as those with other conditions) continue to use CAM to a large degree. Since CAM encompasses a complex array of therapies with biological, physical, and psychological effects, some of which may be harmful, 41 it may enhance patient care if physicians took a proactive role in discussing these options with their patients 42 and steered them toward therapies with the potential to enhance their sense of control over their disease while counseling them to avoid those which may be harmful. Specifically, mind–body interventions such as hypnosis, imagery/relaxation, meditation, and yoga, may be helpful in improving quality of life through increased perception of control. 43 Although more rigorous studies are needed, CAM use appears to be increasing in popularity and filling an important need that should not be ignored. 44 Additional studies of the benefits and risks of these therapies are needed. Furthermore, developing standardized methods of communicating the risks and benefits associated with CAM to patients should be developed since current recommendations are based largely on expert opinion as opposed to being evidence based. 45
Footnotes
Acknowledgements
The ideas and opinions expressed herein are those of the authors and endorsement by the CADHS, the NCI, and the CDC or their contractors and subcontractors is not intended nor should be inferred.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The collection of cancer incidence data used in this study was supported by the California Department of Health Services (CADHS) as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885; the National Cancer Institutes (NCI) Surveillance, Epidemiology and End Results Program under contract N01-PC-35139 awarded to the University of Southern California, and contract N02-PC-15105 awarded to the Public Health Institute (PHI); and the Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under agreement #U55/CCR921930-02 awarded to the PHI.