
Abstract
Background. In the earlier stages of prostate cancer, effective treatments have created a need for research to focus on practices that may improve quality of life throughout survivorship. Physical activity is a significant supportive care management strategy for prostate cancer survivors, though the optimal modality is not yet understood. Hypotheses. The authors hypothesized that yoga would be a feasible physical activity option for prostate cancer survivors and their support persons and that the incorporation of social support would increase physical activity adherence. Methods. This 14-week feasibility study involved a 7-week class-based yoga program (adherence phase), followed by 7 weeks of self-selected physical activity (maintenance phase). Demographic information, physical activity behavior, quality of life, fatigue, stress, mood, and fitness variables were assessed at 3 time points. Prostate cancer survivors’ perceived social support was rated during yoga and after yoga. Results. Class attendance was 6.1 and 5.8 for prostate cancer survivors (n = 15) and their support persons (n = 10), respectively, for the 7 classes. Levels of perceived social support were higher for those who brought a support person. Significant improvements with regard to stress, fatigue, and mood before and after yoga class (all Ps < .05) were reported by all participants. No clinically significant changes were noted on prostate cancer survivor’s quality of life or fatigue over the course of the 14-week study. Conclusions. Yoga is a feasible physical activity option for prostate cancer survivors. The program had a promising uptake rate, high program adherence rate, and there were acute program benefits with regard to stress, fatigue, and mood for all participants. Future examination is warranted with regard to chronic benefits and group cohesion influences on levels of perceived social support.
Keywords
Introduction
Prostate cancer is the most common cancer among Canadian men, with an incidence rate of 129/100 000. 1 Although common, prostate cancer is considered manageable with a wide range of treatment options.1,2 Unfortunately, these prostate cancer therapies tend to significantly affect a man’s physical and psychological well-being, by eliciting harsh side effects, both acutely and long-term. 2
Androgen deprivation therapy (ADT), used to shrink tumors or slow tumor growth, can elicit multiple side effects such as reduced libido, impotence, and fatigue. 3 ADT is also known to heighten one’s risk of depression, increase body weight and fat mass, and decrease bone density.2,4
Radiation therapy, a significant curative treatment, often produces gastrointestinal problems and the need for frequent urination in many cancer patients. 1 Windsor et al 5 report that about 80% of prostate cancer patients experience fatigue at some point during the course of their radiation therapy, with the fatigue becoming chronic in 30% of patients. Fatigue is often associated with other negative impacts, such as psychological distress, poor nutrition, and reduced functional capacity. 5
Depending on the cancer stage and the individuals’ prostate specific antigen level, prostatectomy may be a treatment option. If any damage is done to the surrounding nerves, prostate cancer patients may experience impotence, and even with nerve-sparing surgery individuals may experience incontinence. 1 Sexual problems can have profound effects on both the cancer survivor and their partner, eliciting feelings of frustration, loss of self-esteem, and embarrassment. 6
At later stages of prostate cancer, chemotherapy may be necessary and side effects including nausea, vomiting, and fatigue commonly occur. 1 Not surprisingly, all men diagnosed with prostate cancer—whether monitoring prostate specific antigen levels, receiving treatment, or recovering—are at a significant risk for decreased quality of life (QOL) because of negative physical changes and emotional distress.7,8
Supportive interventions, such as physical activity programs, are following a recent trend in health research that is steering away from solely treating an individual’s disease to addressing their overall health-related QOL.9,10 The benefits produced by resistance and aerobic training programs that are designed specifically for prostate cancer survivors are well established.11-15 Some of these benefits include increased muscular strength, 16 decreased fatigue levels,16-18 and increased aerobic capacity. 15 Still unknown is the optimal modality of physical activity for this population, from a health benefit, personal preference, and feasibility standpoint.
A potential alternative form of physical activity to the commonly examined types (resistance and aerobic training) is yoga. Yoga, an Eastern mind–body practice, has been used for physical and emotional therapeutic benefit for thousands of years. Traditionally, yoga is one of the 6 branches of classical Indian philosophy and encompasses 8 disciplines pertaining to ethics, individual observances, postures, breath control, withdrawal of senses, concentration, meditation, and self-realization. 19 In Western practice, yoga typically refers to the third and fourth limbs, postures (asanas), and controlled breathing (pranayamas). 19 A variety of yoga styles are practiced in Western cultures (eg, Iyengar, Ashtanga, Vini, Hatha, Tibetan), all of which incorporate their own asanas, pranayamas, and mind–body or meditative techniques.19,20
Although yoga is not a new therapy, only recently has it been empirically reviewed for use in cancer populations as a valuable complementary therapy to help manage cancer side effects. 21 Researchers interested in yoga’s positive influences on the cancer survivor population suggest that it may be a gentler form of physical activity that could help promote regular participation for individuals who may face additional barriers compared with the general population, such as treatment side effects.22,23
The yoga and cancer research conducted to date, almost exclusively with survivors of breast cancer, reveals a diverse list of benefits.21,22,24 Several psychological benefits have been noted such as improved mental health,25,26 spirituality,25,27 mood, 28 and emotional function,29,30 along with decreased anxiety and depression.23,28,31 QOL improvements were reported in a variety of areas such as fatigue,32-34 sleep quality,20,32 and overall QOL scores.27,29,33,35 Many participants also demonstrated positive medical changes such as decreased shoulder stiffness, 28 decreased bodily pain, 26 and decreased hot-flash frequency and severity, 32 along with decreases in postchemotherapy nausea 36 and treatment-related distress symptoms. 32 Moreover, adherence rates for yoga programs are quite promising. For example, Blank et al 28 reported a 92% attendance rate for their yoga program offered to breast cancer survivors, whereas Cohen et al 37 reported that 92% of participants attended 7 of the 8 yoga sessions.
Although the aforementioned benefits are significant, this is not to say yoga will produce the same benefits in different cancer populations who undergo vastly different treatments (ie, prostatectomy vs mastectomy or radiation therapy directed toward breast tissue vs radiation therapy directed toward the prostate located very close to the urinary and gastrointestinal system). Each unique treatment comes with unique side effects and emotional tolls. 2 For these reasons, the benefits of yoga must be examined in each cancer population separately.
In addition to determining the optimal modality of physical activity for prostate cancer survivors, it is important to recognize that cancer survivors face an abundance of barriers along the way, from the aforementioned side effects, to time constraints and family commitments, to issues of accessibility, thus creating a complex behavior for an individual to adhere to alone. Recognizing that individuals who are adopting or maintaining physical activity could benefit from the aid, assistance, or support received from others38,39 may be an important part of physical activity program design.
Purpose
To our knowledge, this is the first study to examine the feasibility and benefit of a therapeutic yoga program offered to prostate cancer survivors and their support persons. For the purpose of this study, a feasible program was defined as one that prostate cancer survivors self-registered for during the recruitment period, adhered to during the intervention (ie, class attendance as high or higher than reported in previous physical activity research, ranging from 60% to 85% 40 ), and benefited from with regard to the outcomes described below. Additionally, the program was considered to be feasible if the participants did not report any adverse events (eg, musculoskeletal injury, cardiovascular event, etc). The secondary purpose included examining the impact of social support on physical activity adherence.
Methods
This study was a 14-week feasibility study made up of an adherence phase, weeks 1 to 7, which involved a class-based therapeutic yoga program offered to all prostate cancer survivor participants and their support persons, and a maintenance phase, weeks 8 to 14, which involved self-selected physical activity.
Participants
Prostate cancer survivors were recruited to this yoga for cancer survivors program via various methods including poster and pamphlet recognition, physician referrals, study information sessions at the local treatment center, and cancer support group newsletters. Support persons were identified by survivors, if they chose to include a support person in their program. The support person could be of any relation to the prostate cancer survivor, including spouse, friend, or other relative. The following inclusion criteria were met by each participant: (a) a diagnosis of prostate cancer (stage I-IV; did not apply to support persons), (b) at least 18 years of age, (c) the ability to read and write in English, (d) no barriers to physical activity assessed by the Physical Activity Readiness Questionnaire (PAR-Q) or by the Physical Activity Readiness Medical Examination (PARmed-X), and (e) resting blood pressure <144/94 mm Hg and resting heart rate <100 beats per minute before each of the 3 fitness assessments. 41 Additionally, each participant read and signed an informed consent form that was approved by the Conjoint Health and Research Ethics Board. As this was a pilot study examining the feasibility of a yoga program for prostate cancer survivors, no inclusion criteria with regard to treatment status, social economic status, or ethnicity was employed.
Yoga Sessions
All yoga classes ran weekly for 7 weeks and were 75 minutes in length. Participants were divided among 4 sessions. To reduce program delivery variability, each of the certified yoga instructors attended the teacher-training workshop at the University of Calgary through the Health and Wellness Laboratory, ensuring competence in the research-based yoga for cancer survivors program (Table 1). The 4 yoga instructors for the study taught the following specific sequence:
0 to 10 minutes: Gentle breathing and laying supine with legs flexed at the hip and supported by a wall. The pelvis was in a neutral position and arms were abducted with palms facing toward the ceiling.
10 to 60 minutes: A series of 6 to 10 modified yoga poses composed of gentle stretching and strengthening exercises of specific groups of muscles, tendons, and ligaments (Table 1). The asanas became more challenging over the course of 7 weeks as the participants’ yoga abilities improved.
60 to 75 minutes: Relaxation. For these final 15 minutes, students focused their attention on breathing and on the internal sensations of the body, while laying in a supine position with legs slightly abducted or with knees in flexion with the plantar side of the feet placed on the floor, arms slightly abducted, palms up (ie, savasana or corpse pose).
Yoga Thrive 7-Week Protocol a

Each session occurs over a 75-minute period.
Data Collection
The following data were gathered via questionnaire packages and fitness appraisals at each of the 3 assessment points (baseline, post yoga program, and 7-week follow-up, unless otherwise noted).
Demographics—All
The demographic information collected from all participants included age, date of birth, marital status, education level, annual income, employment status, and previous participation in yoga. Medical information collected from the prostate cancer survivors included cancer diagnosis (month, year, stage at diagnosis, current stage, local, or metastatic), surgery (yes/no), ADT (yes/no), date of last treatment, other forms of treatment (type and length), and change in treatment regime (post program and follow-up assessments only).
Physical activity—All
Godin’s Leisure Score Index (LSI) of the Godin Leisure Time Exercise Questionnaire was used to assess all participants’ physical activity at all the 3 assessment points. 42 The LSI is a valid and reliable measure, based on criteria such as test–retest scores, objective activity monitors, and fitness indices. 43 The scale has also been used successfully in adult prostate cancer survivor populations and in yoga research.18,29,44 The LSI contains 3 questions that assess the frequency and duration of mild, moderate, and strenuous physical activity preformed for at least a 15-minute duration during free time in a typical week in the past month. 42 A change of 30 minutes of activity per week between assessment points was considered to be a clinically important difference, as this amount equals one additional day of physical activity according to the Canadian Physical Activity Guide. 45
Physical activity levels for the yoga sessions were measured via attendance logs (adherence rate), completed weekly by the instructors. A calendar was used as an additional daily physical activity log during the maintenance phase, completed by the participants. The calendar allowed participants to record any physical activity bouts (mild, moderate, or strenuous) lasting 10 minutes or longer.
QOL—Prostate cancer survivors
Prostate cancer survivors’ QOL was measured using the Functional Assessment of Cancer Therapy–Prostate scale (FACT-P). The FACT-P includes the 27 general questions of the Functional Assessment of Cancer Therapy–General scale (FACT-G) that provide assessments of physical, social or family, emotional, and functional well-being, with a scoring range of 0 to 108,45,46 along with 12 supplementary questions regarding “additional concerns” specific to prostate cancer and its treatment. 47 The FACT-P has a scoring range from 0 to 156, with a higher score representing a better QOL. The recommended clinically important difference range on the FACT-P is between 6 and 10, while a change of 4 is considered to be a clinically important difference on the FACT-G.48,49 At all the 3 assessment points during the current study, Cronbach’s α levels of the FACT scales exceeded .70 except on 2 of the subscales (emotional well-being and additional concerns); therefore, caution should be taken with interpretation of these specific subscales.
QOL—Support persons
QOL assessment for the support persons was measured using the Short Form 12 (SF-12). This 12-item survey was derived from the Short Form 36 and has proven to be a reliable and valid assessment of QOL in various populations. The results of the SF-12 are expressed by 2 meta-scores—the Physical Component Summary and the Mental Component Summary—each with a scoring range from 0 to 100 and designed to have a mean score of 50 and a standard deviation of 10 in a representative sample of the US population. 50 A high score on the SF-12 indicates better QOL. A clinically important difference on the SF-12 is considered to be a change of 5 units. 51
Fatigue—Prostate cancer survivors
The Functional Assessment of Cancer Therapy–Fatigue scale (FACT-F) was used to measure fatigue levels in prostate cancer survivors. 52 The FACT-F is a 13-item scale that includes items relating to the consequences of fatigue and symptom expression. The fatigue scale has excellent internal consistency (αs = .95), 52 and in the current study, Cronbach’s α values exceeded .80 at all the 3 assessment points. The scoring range on the FACT-F is from 0 to 52, with a higher score reflecting less interference from fatigue on activities and roles of daily living. A clinically important difference on the FACT-F is considered to be 3. 49
Fatigue—Support persons
The Fatigue Severity Scale (FSS), used to assess support person’s fatigue levels, has been widely used in a variety of populations.53,54 Using a 7-point scale, 9 items of fatigue are evaluated to provide a unitary measure of fatigue. This instrument has good internal consistency in both cancer (α = .96) and healthy controls (α = .88).53,55 In the current study, Cronbach’s α values exceeded .80 at all the 3 assessments points. The FSS is designed to have a mean scoring range of 1 to 7, with a higher score indicating a higher level of fatigue. A clinically important difference on the FSS is defined as a change in the range of 0.5 to 3.5, while a score above 5.2 is considered to be a clinical level of fatigue.54,56
Social support—Prostate cancer survivors
The Social Provisions Scale (SPS) was filled out at the follow-up assessment only and was used to measure prostate cancer survivors’ perceived social support 57 retrospectively, during the yoga program and presently, following the completion of the yoga program. Statements such as “There are people I know who will help me if I really need it” were rated in terms of the way participants felt during the 7-week program versus the way they felt after completion of the 7-week program. The SPS assesses different facets of social support (ie, attachment, social integration, reassurance of worth, reliable alliance, guidance, and opportunity to nurture). A higher score indicates a higher level of perceived social support. Scores from this instrument have been shown to be reliable and valid in both healthy and cancer populations.58,59
Fitness—Prostate cancer survivors
Prostate cancer survivors’ fitness and physiological assessments followed the Canadian Physical Activity, Fitness and Lifestyle Approach (CPAFLA) protocol and were administered by a certified exercise physiologist (CSEP-CEP) at all the 3 assessment points. Along with an approved PAR-Q or PARmed-X form, pretest screening included resting blood pressure (<144/94 mm Hg) and heart rate (<100 beats per minute) to ensure each participant was cleared for exercise on his assigned assessment day. The fitness assessments included flexibility (sit-and-reach), muscular strength (hand dynamometer), and functional exercise capacity (6-Minute Walk Test). Anthropometric assessments included bodyweight, height (used to calculate body mass index), and waist circumference.
Thermometer ratings—All patients
Before and after each yoga practice, all participants were asked to rate his or her stress, mood, and fatigue level on a “thermometer” scale ranging from 0 to 10, with 10 indicating extreme stress, extreme fatigue, and positive mood, and 0 representing no stress, no fatigue, and negative mood. These indices were used both for statistical analysis and for participant monitoring by the yoga instructors.
Statistical Analysis
PASW statistical package (version 18.0) was used for all statistical analyses. One-sample Kolmogorov–Smirnov tests (exact significance) were used to examine the normality of the data, while stem-and-leaf plots were used to scan for any outliers in the data set. Descriptive statistics were used to describe the study sample and questionnaire outcomes. Analysis of variance (ANOVA; parametric) along with Friedman’s ANOVA (nonparametric) tests were run to indicate any significant changes between assessments for the primary outcomes. When necessary, post hoc analyses were carried out (ie, Bonferroni correction to address the problem of multiple comparisons and decrease the chance of a type I error, when additional analysis was carried out to indicate specifically where significant differences occurred and Wilcoxon signed-rank tests when multiple comparisons were of a nonparametric nature). Finally, t tests were run to (a) compare adherence rates, (b) compare physical activity maintenance levels, and (c) compare perceived social support, between those who chose to bring a support person to the yoga program versus those who did not. t Tests were also used to examine perceived social support of prostate cancer survivors during the yoga program compared with after yoga and additionally to compare acute levels of mood, stress, and fatigue before and after each yoga class for all participants.
Results
Accrual
Active recruitment occurred over the course of 4.5 months from September 2009 to January 2010, during which time 34 individuals (including both prostate cancer survivors and support persons) expressed interest in the program either by providing contact information at an information session or by phone calls to the researcher. Of the 34 who showed initial interest in the program, 25 completed program registration—15 prostate cancer survivors and 10 support persons (identified by the prostate cancer survivors). Of the 10 support persons, 9 were spouses of the prostate cancer survivors and 1 was a friend. All 25 participants completed their questionnaire packages at the 3 assessment points. Only 1 prostate cancer survivor was unable to attend his final fitness assessment session due to surgical complications.
Demographics
Demographic characteristics of the study participants are presented in Table 2. The mean age of the entire sample was 62.0 ± 9.1 years. Ages for prostate cancer survivors ranged from 48 to 81 years (mean = 64.5 years), whereas the support persons ranged in age from 49 to 72 years (mean = 60.6 years). All the support persons were female, of whom 9 were spouses and 1 was a friend. The full medical information of the prostate cancer survivors is given in Table 3.
Participant Demographic Information

Prostate Cancer Survivors’ Medical History
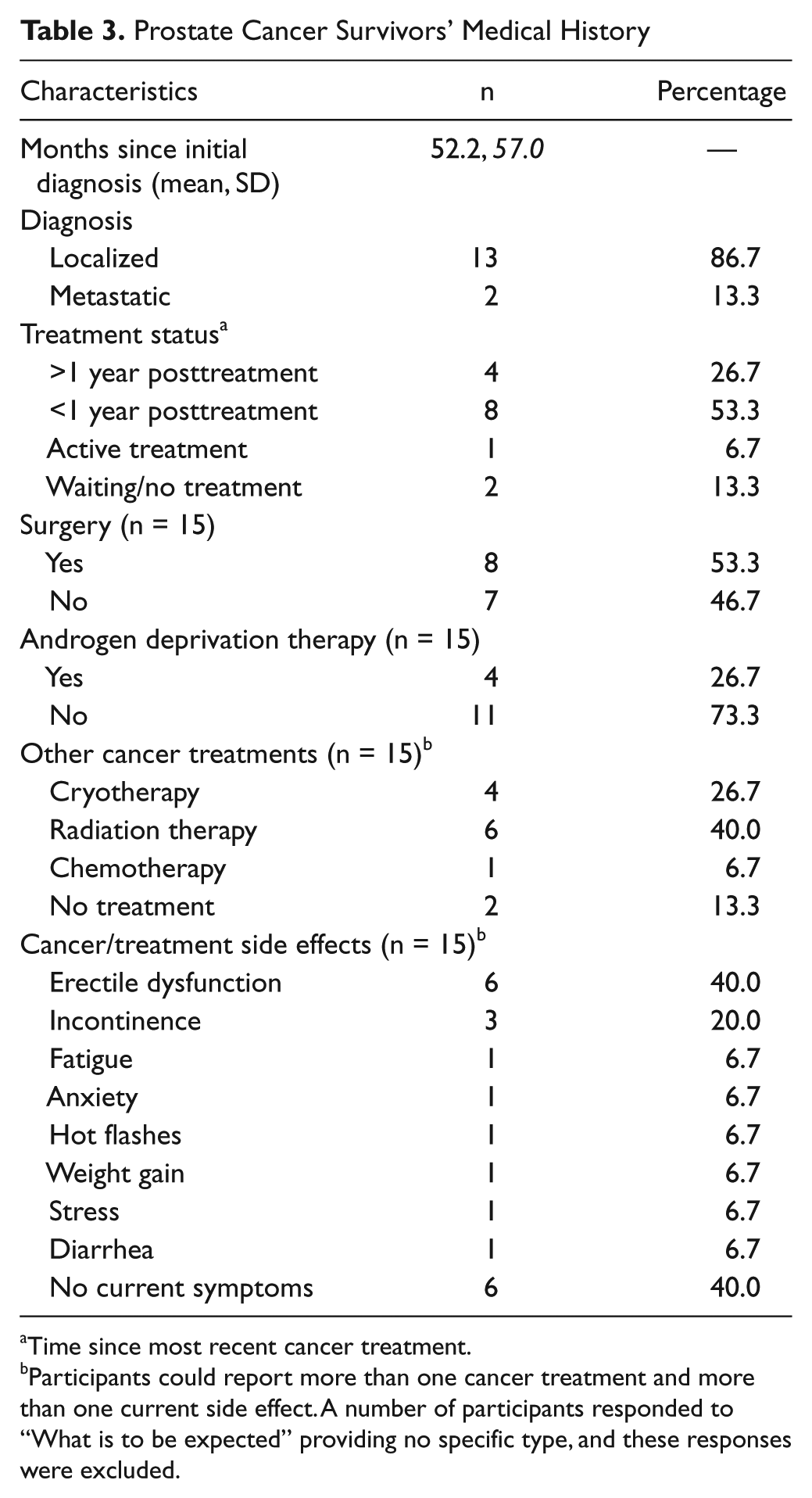
Time since most recent cancer treatment.
Participants could report more than one cancer treatment and more than one current side effect. A number of participants responded to “What is to be expected” providing no specific type, and these responses were excluded.
Attendance
Yoga program attendance as recorded by the yoga instructors at the beginning of each class was extremely high. The mean numbers of classes attended, out of the 7 classes, were 6.1 ± 0.8 and 5.8 ± 0.8 for prostate cancer survivors and support persons, respectively. The number of yoga classes attended by those prostate cancer survivors who brought a support person (mean = 6.0) compared with those who did not (mean = 6.2) were not significantly different (P = .664).
Acute Yoga Intervention Benefits: Stress, Mood, and Fatigue
T-test comparisons of the thermometer ratings from before to after each class revealed improvements in prostate cancer survivors’ mood (P = .000) and decreases in levels of fatigue and stress (P = .000, P = .004, respectively). Similar benefits were seen for the support persons, with improvements in mood (P = .000) and decreased levels of fatigue and stress (P = .001, P = .030, respectively) from the beginning to the end of each yoga session. For a summary of the acute yoga class benefits, see Table 4.
Thermometer Scale Ratings
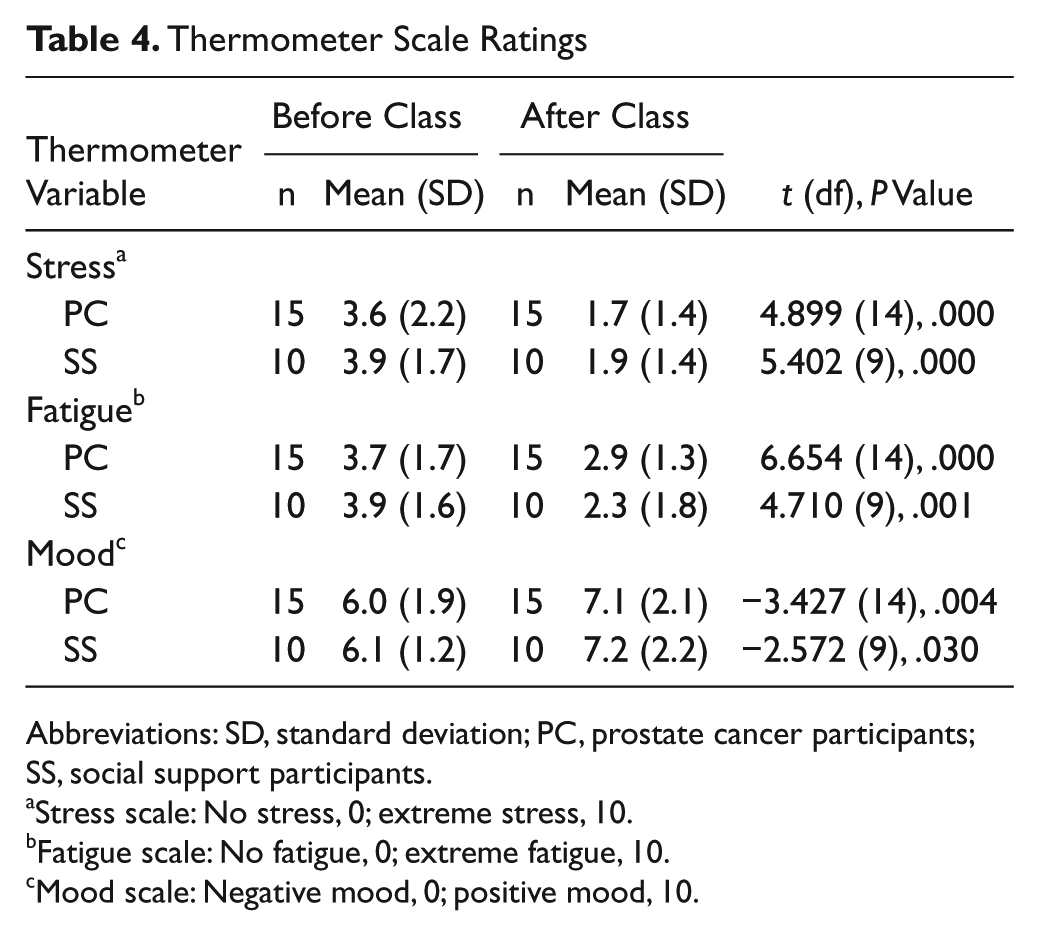
Abbreviations: SD, standard deviation; PC, prostate cancer participants; SS, social support participants.
Stress scale: No stress, 0; extreme stress, 10.
Fatigue scale: No fatigue, 0; extreme fatigue, 10.
Mood scale: Negative mood, 0; positive mood, 10.
Physical Activity Levels
According to the ANOVA tests, there were no statistically significant changes on any of the physical activity variables for either the prostate cancer survivors or the support persons (all P values > .05), including physical activity duration, frequency, or LSI total score.
Quality of Life
There were no statistically significant changes on any of the QOL scales (all P values > .05) for prostate cancer survivors over the 14-week study except for on the FACT-P (ANOVA: P = .019, Friedman’s: P = .053), which decreased significantly after the program (Bonferroni approach; see Table 5).
Participant Reported Outcomes

Abbreviations: FACT-(P, G), Functional Assessment of Cancer Therapy–(Prostate, General); PC, prostate cancer; PCS, physical component summary; MCS, mental component summary; FACT-F, Functional Assessment of Cancer Therapy–Fatigue; FSS, Fatigue Severity Scale.
Higher scores on the FACT-(P, G) scales and subscales indicate better quality of life.
Statistically significant at α < .05.
Exact significance is reported from Friedman’s test.
A score above 50 on the SF-12 represents a better quality of life, while a score below 50 represents a worse quality of life.
Higher scores on the FACT-F reflects less interference from fatigue on activities and roles in daily life.
A score of >4 points indicates clinically significant fatigue.
= Clinically important difference from the previous assessment.
Neither of the SF-12 QOL subscales (physical or mental) used to measure the support persons’ QOL changed significantly over the course of the study (P values > .05). At all the 3 assessment points the mental component score was consistently higher than the physical component score (see Table 5).
Fatigue
ANOVA tests indicated the fatigue prostate cancer survivors experienced did not change significantly over the course of the 14-week program (P > .05; see Table 5). This was also true of the support persons, as their fatigue levels did not change by a statistically significant amount from preintervention to postintervention to follow-up (P values > .05; see Table 5).
Perceived Social Support
Paired t tests were used to examine the perceived social support prostate cancer survivors felt retrospectively (during the yoga program versus after the yoga program). Both ratings were measured on the follow-up questionnaire. There were no statistically significant differences (P > .05) in the perceived social support that participants indicated they felt during the yoga program versus after the yoga program.
Ratings of perceived social support were statistically higher (P = .037) during the yoga class for those who chose to bring a support person than for those who chose not to (see Table 6). Although those with support also demonstrated higher perceived social support levels following the yoga program, the difference was no longer significant (P > .05).
Perceived Social Support Outcomes

Abbreviation: SPS, Social Provisions Scale.
A higher score indicates a greater degree of perceived support.
Fitness and Anthropometrics
Examination of fitness measures and anthropometrics (Bonferroni correction) indicated an improvement in flexibility from 27.3 ± 12.3 cm to 29.3 ± 10.6 cm (P = .048) from preintervention to follow-up. No other fitness or anthropometric measures changed significantly over the course of the study.
Discussion
Feasibility
The purpose of this study was to determine if a therapeutic yoga program offered to prostate cancer survivors would be a feasible physical activity option. For the current study, a feasible program was defined as one that prostate cancer survivors self-registered for during the recruitment period, adhered to during the intervention, provided potential benefits (or no negative impact) on the outcomes of interest, and did not result in any adverse events (ie, injuries from yoga). Examining the impact of social support on physical activity adherence was a secondary focus of the study.
Results from our study suggest a therapeutic yoga program offered to prostate cancer survivors and their support persons is a feasible physical activity option. First, although the current sample was relatively small, it does compare with the original yoga research on which this study is based, in which 38 cancer survivors (20 intervention and 18 control participants) were recruited in approximately 1 year. However, in both the original study and the ongoing community-based Yoga Thrive program, approximately 95% of the participants are female. This highlights the need for research examining the role of yoga for male cancer survivors.
Promising initial uptake rates of prostate cancer survivors were supported by a program adherence rate of 87%. This level of adherence is slightly higher than the commonly reported adherence rates (60% to 85%) in the general cancer survivor population for physical activity interventions 40 yet similar to that reported in past yoga programs (eg, 92% compliance rate in Blank et al 37 ).
Furthermore, no adverse events, including injuries or cardiovascular complications, were reported by any of the participants during or following the yoga program. This is of particular importance as both the recommendation and administration of safe physical activity programs for cancer survivors is crucial.
Although the cancer and yoga literature has shown various improvements in patient-reported outcomes, the current study found acute changes (ie, thermometer scale ratings of pre- and postclass changes) but relatively few chronic changes from preintervention to postintervention. Specifically, fatigue was unchanged during the 14-week study and QOL scores, although lower after the program, did not change by a clinically significant amount. 48 However, the scores observed on the QOL scales for the prostate cancer survivor group were on par with nondiseased populations 60 and were approaching “ceiling” values, 61 thus it is not surprising that the yoga program had little impact. This sample was also relatively active before beginning the yoga program, with 87% of participants meeting the Canadian Physical Activity physical activity guidelines at the baseline assessment. 45 It may be that this population had already experienced the QOL benefits associated with physical activity, such as improved physical function and psychological well-being. 62
Finally, only minor changes in flexibility, with statistically significant increases that were maintained at the follow-up assessment, were seen. It may be that more chronic fitness benefits, such as resistance and aerobic functioning, are gained from long-term 63 or more frequent yoga practice. For example, although changes in functional aerobic capacity were not significant from preintervention to postintervention (P = .478), there was a trend toward increased walk distances during this time (641.0 ± 93.7 to 662.8 ± 82.4). A 54-meter change in walking distance is considered to be a clinically important difference, 64 and after 7 weeks of yoga, participants’ mean walking distance increased by about half this amount.
Although no long-term benefits were reported with regard to prostate cancer survivors’ QOL or fatigue levels, noteworthy were the acute effects participants experienced during each yoga session. Specifically, the prostate cancer survivors experienced significant decreases in their levels of stress and fatigue, along with significant increases in mood, from the beginning to the end of each yoga session. The yoga intervention used gentle poses and stretching that may be less likely to produce adverse consequences and be more likely to foster compliance to the program. 19 Moreover, yoga is meant to promote a union between body, mind, and spirit, differentiating it from more conventional forms of physical activity. 21 This mindful practice associated with yoga may generate immediate positive consequences, both physically and psychologically. 24 Future research will need to more fully examine the link between mindfulness and positive changes in these patient-reported outcomes.
Though adherence to the current program was not higher for those who chose to bring a support person compared with those who chose not to, involving a support person was associated with higher levels of perceived social support. This may be reflective of the direct assistance or encouragement the prostate cancer survivors felt from their support person. 65 Alternatively, as the overall mean perceived social support for all prostate cancer survivors during yoga was reasonably high, the peer atmosphere of the classes may have provided support for the participants. The influence of group cohesion in promoting physical activity adherence is well established in the general older adult population and should be further investigated in the context of activity programming for prostate cancer survivors. 66
Support Persons’ Outcomes
Over the course of the study, support persons’ physical and mental QOL scores were above the population norm of 50, indicating a high QOL, 67 and did not significantly change between assessments. Additionally, when compared with a group of spouses whose partners had advanced stages of prostate cancer or had just been newly diagnosed, it is apparent that the support persons in the current study demonstrated mental QOL that was marginally higher and physical QOL that was markedly higher. 68 As the majority of the prostate cancer survivor sample had localized prostate cancer and many were posttreatment, into the recovery stage, the influence of symptom distress on the support persons’ QOL may have been lessened.
Heightened levels of fatigue are also commonly reported by cancer survivors’ support persons or caregivers. 69 Before commencing the yoga program, support persons were considered to be clinically fatigued. 56 Though their perceived fatigue was still rated at a clinical level following the yoga program, it did decrease by a clinically significant amount. 54 Seven weeks later, at the follow-up assessment, perceived fatigue returned to baseline values, indicating the yoga program’s potentially positive influence on fatigue levels.
Conclusion
This study is the first to examine the feasibility of a therapeutic yoga program offered to prostate cancer survivors and is unique in its incorporation of an additional aspect of social support, beyond that of group dynamics, by inviting survivors to bring a support person with them to the yoga program. The results revealed yoga for prostate cancer survivors to be a feasible program. Program registration, high adherence rates, high program completion rates, and no reports of adverse events all support the feasibility of offering yoga for prostate cancer survivors. Overall, a yoga intervention for the prostate cancer survivor population is feasible and appears to offer some potential benefits. Specifically, the prostate cancer survivors who took part in this study exhibited significant increases in flexibility, an aspect of fitness key for independent living and overall health. Finally, the yoga program produced acute benefits during each class, including decreased stress and fatigue and improved mood.
The primary limitations of the current study were the small sample size recruited for the purpose of assessing program feasibility, the lack of a control group, and the 1-item preclass/postclass primary outcome measure. Additional limitations within the sample include the potential self-selection bias of healthier and more active individuals who were interested in a yoga program. This group was heterogeneous in regard to physical activity levels, socioeconomic status, treatment status, and time since treatment completion.
Future research might consider a number of methodological changes based on findings from the present study. First and foremost, offering a greater number of yoga classes over a longer period of time, thereby maintaining the small class sizes while increasing the overall sample, would allow for greater statistical power and the potential to highlight significant changes concealed by a small sample. Inclusion of a control group (waitlist or an “active” comparison) would also aid in determining if the changes are due to the yoga intervention or to other factors (ie, time, group environment, attention, etc). Future research recruitment strategies that also focus on informing prostate cancer survivors’ wives, partners, and caregivers may be advantageous, as many of the initial registration calls were from the support persons. Future studies might also benefit from a stronger physician referral system to boost enrollment. Examining the role of social support on physical activity adherence and maintenance, by comparing classes with or without support persons, should be examined, and finally, examining maintenance tools, such as a yoga DVD for at home use, may be beneficial. Last, with regard to the yoga program itself, exploring the ideal “dose–response” is essential for future program design and prescription. Past yoga programs for cancer survivors have ranged from once per week to daily practice, 22 with a mix of instructor-led and home-based sessions. The ideal dose–response of therapeutic yoga, specific to various cancer diagnoses, is yet to be explicitly described. This is essential to produce the optimal gains in areas such as decreased treatment side effects, fatigue, mind/body connection, and overall enhanced QOL.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Culos-Reed receives funding support from the Canadian Imperial Bank of Commerce for her cancer survivorship research program.