
Abstract
Chemotherapy- and radiotherapy-induced nausea and vomiting are the most common, intractable and unpleasant side effects in patients undergoing treatment for cancer. 5-Hydroxytryptamine-3 (5-HT3) receptor antagonists plus dexamethasone have significantly improved the control of acute nausea and vomiting, but delayed nausea and vomiting remains a significant clinical problem. Combined neurokinin-1 receptor antagonists with 5-HT3 antagonists and steroids are observed to be better in the control of both acute and delayed emesis. However, the use of these antiemetics is observed to possess inherent side effects. The medicinal plants such as Scutellaria baicalensis, Korean red ginseng, American ginseng berry, Ganoderma lucidum, Zingiber officinale, grape seed extract, and the oil of Mentha spicata are reported to be effective in the treatment of nausea and vomiting mostly in preclinical studies. Of these, ginger has also been evaluated for its efficacy in humans and the results have been contradictory. The current review for the first time summarizes the results related to these properties. An attempt is also made to address the lacunae in these published studies and to emphasize aspects that need further investigations for these plants to be of use in clinics in the future.
Introduction
Despite significant progress in the field of cancer treatment, effective management of chemotherapy- and radiation-induced nausea and vomiting, abbreviated as CINV and RINV respectively, is still a major problem as nearly 70% to 80% of patients are affected. 1 These complications are the most feared adverse effects of these cytotoxic treatment modalities and may compel the patient to opt out of the therapy. Severe nausea and vomiting at times leads to the development of complications such as fluid–electrolyte imbalances, weight loss, dehydration, anorexia, weakness, fractures, esophageal tears, prerenal azotemia, wound dehiscence, or decline in behavioral and mental status. 1
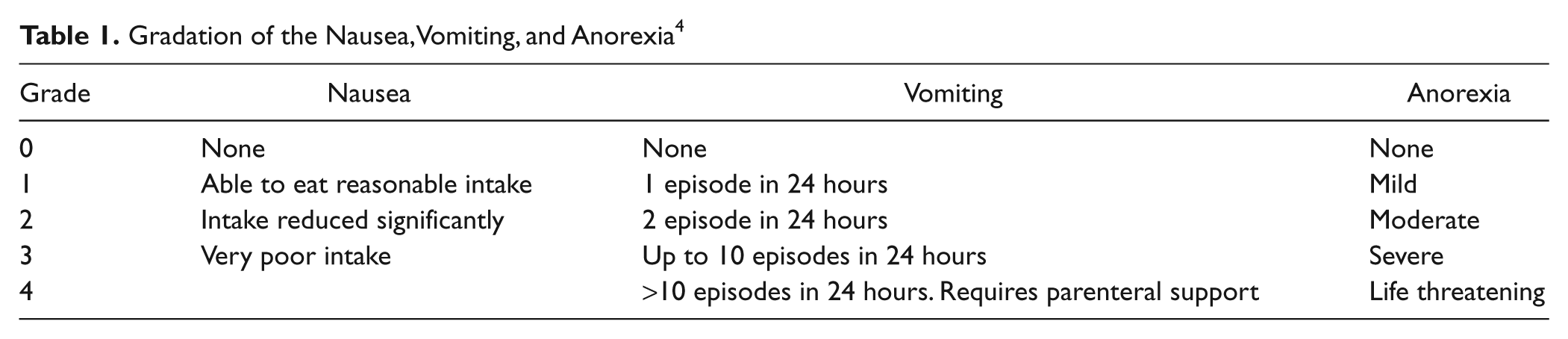
These adverse effects may deteriorate patients’ physical and mental status, self-care, and functional ability and may lead toward withdrawal from the anticancer treatment regimen. This will invariably affect the treatment outcome and survival of the patient.1,2 It also increases patient’s anxiety and dissatisfaction with the hospital experience and may contribute to future anticipatory nausea. 3 Depending on the severity and frequency, nausea and vomiting are graded as represented in Table 1.
Gradation of the Nausea, Vomiting, and Anorexia 4
Depending on the time after administration of the chemotherapy/radiotherapy, nausea may be classified as acute nausea, which occurs within 24 hours after chemotherapy and can be subdivided into early acute (within 12 hours) and late acute (12 to 24 hours); delayed nausea, which appears more than 24 to 96 or 120 hours after treatment; anticipatory nausea, which occurs before a new cycle of chemotherapy in response to conditioned stimuli, such as the smells, sights, and sound of the treatment room and breakthrough nausea and vomiting that occurs despite preventive therapy.1-3,5
The major factors that determine the incidence and severity of CINV include the dose and type of chemotherapy administered, the treatment schedule, the use of combinations of chemotherapeutic agents, and patients’ inherent characteristics. Chemotherapeutic agents such as carmustine, cisplatin, cyclophosphamide (≥1500 mg2), dacarbazine, mechlorethamine, and streptozocin are the highly emetogenic and cause increased frequency of nausea and vomiting. 5
Comparatively, RINV is not as prevalent or severe as CINV but can interrupt treatment schedule, can negatively influence the efficacy of the treatment, and can affect the quality of life. 6 The pathophysiology of RINV is incompletely understood but is thought to be similar to that caused by chemotherapy. 6 Unlike chemotherapy, which is systemic treatment; radiotherapy is delivered from an external source and is localized. 6 The severity of RINV depends on the site of irradiation, the field size, and the dose per fraction.6,7 RINV is very high when the total body, proper abdominal, and gastrointestinal regions are irradiated; moderate when the upper abdomen, pelvic, and cranial parts are involved; low when the lower thorax and craniospinal regions are subjected; and minimal when breast and extremities are irradiated.6,7
Increased risk of CINV and RINV are observed in patients younger than 50 years, with history of light alcohol use, and with history of vomiting during pregnancy-induced nausea/vomiting. Additionally, patients who are dehydrated, debilitated, those who have an electrolyte imbalance, or those who have recently undergone surgery or radiation therapy, are also at greater risk of experiencing serious complications from CINV and RINV.1-3,5-7
Physiological and Biochemical Basis for Nausea
Chronic nausea in the setting of cancer treatment is often multifactorial in origin. Factors such as raised intracranial pressure, metabolic abnormalities such as hypercalcemia, hyponatremia, and uremia, dehydration, malignant bowel obstruction, and gastroduodenal ulcers contribute to vomiting and nausea. 8 Nausea also has a psychological basis, which may either exacerbate or induce chronic nausea. 8 Neurophysiologic studies have shown that both nausea and vomiting are controlled and mediated by the central nervous system but by different mechanisms.4,9 Nausea is mediated through the autonomic nervous system, whereas vomiting results from the stimulation of a complex reflex that is coordinated by a putative true vomiting center.4,10
The vomiting center is believed to receive convergent afferent stimuli from several central neurologic pathways. The sensory stimuli of smell, taste, psychological response, and pain, led from the limbic system stimulate the chemoreceptor trigger zone (CTZ). Motion sickness occurs via impulses from the labyrinthine apparatus of the inner ear. Exogenous chemicals and endogenous substances that accumulate during inflammation, ischemia, and irritation stimulate vagal and spinal nerves from visceral and vasculature to cause vomiting and nausea.4,10
The cause of CINV has both components, that is, peripheral and central, which makes it difficult to treat. Serotonin is produced by the enterochromaffin cells in the enteric nervous system, which accounts for 80% of the total body serotonin. Intestinal irritation or damage to the neoplasm leads to release of 5HT that stimulates the 5HT3 receptors and CTZ that ultimately stimulates the vomiting.4,10
The central pathway, on the other hand, is induced by substance P, which is abundantly present in the CTZ and stimulates the neurokinin-1 receptors as well as the gastrointestinal vagal afferent nerve fiber. A multitude of receptors is effected in CINV, namely, CB1 (canabinoid-1), D3 (dopamine-3), D2 (dopamine-2), H1 (histamine-1), M3, M5 (muscarinic-3 and -5), and GABAB (gamma amino butyric acid-B). This is reflected in the wide array of antiemetic drugs that are present. There are more neurotransmitters and receptor systems in play which are as yet unascertained. In CINV sometimes although emesis is brought under control with drugs, nausea continues unabated, reducing the quality of life.4,10
Conventional Antiemetic Agents Used in Cancer Treatment
Antiemetic agents are the most commonly used interventional agents in the management of treatment-related nausea and vomiting. Conventionally, an antiemetic agent should be effective against the nausea and vomiting produced by most chemotherapeutic drugs; have no interaction with the cancer chemotherapeutic agents; be available as oral, injectable, and suppository forms; possess minimal side effects, especially euphoric reactions; be efficient and reproducible gastrointestinal absorption; have therapeutic blood levels for 4 to 12 hours postadministration; be effective with repeated use; show low abuse potential; and have reasonable cost. 4
The basis for antiemetic therapy is the neurochemical control of vomiting. Many antiemetics act by competitively blocking receptors for these substances, thereby inhibiting stimulation of peripheral nerves at the CTZ, and perhaps at the “vomiting center.” Combination of antiemetic regimens has become the standard care for the control of CINV. 10 However, the choice is complicated as when selecting an antiemetic the clinicians must opt for an agent that provides optimal protection against nausea and vomiting while avoiding drug–drug (antiemetic–anticancer) interactions and additional adverse events. The other factors that need to be considered are the dose of antineoplastic agent used, the combination of antineoplastic drugs, route of administration, and the treatment schedule.1,4
Regimens to prevent radiation- and chemotherapy-induced nausea and vomiting are guided by the emetogenic potential of the drug dose and the combinatorial agents used. Patients in a hospital setup receiving highly emetogenic potential chemotherapy, may require higher doses of antiemetics, whereas those receiving highly emetogenic chemotherapy on an outpatient basis may do best with sublingual or rectal antiemetic routes of delivery.1,4 Various classes of antiemetics, their applications, and inherent side effects are summarized in Tables 2 and 3.
Potency of Antiemetic Drugs 4

Side Effects of Antiemetics Commonly Used in the Prevention of CINV and RINV

Abbreviations: CINV, chemotherapy-induced nausea and vomiting; RINV, radiotherapy-induced nausea and vomiting; HPA axis, hypothalamic–pituitary–adrenal
Plants as Antiemetic Agents
Complementary therapies are widely used throughout the world and according to a recent report almost 80% of the global population relies on alternative therapies for their health care. 11 When compared with the conventionally used drugs of modern medicine, these medications are clearly underresearched. However, their wide acceptance makes it imperative that scientific investigations are performed with the plants commonly used in the various traditional systems of medicine and have been practiced for centuries. 11
Observations suggest that traditional knowledge and plants have contributed to the development of antiemetic drugs in the prevention of CINV and RINV and the development of the cannabinoids dronabinol, nabilone, marinol, and cannabis from Cannabis sativa commonly known as marijuana is the best example. 4 Scientific studies carried out in the past 2 decades have shown that some of the most important medicinal plants, for xample, Scutellaria baicalensis, Korean red ginseng, American ginseng berry, Ganoderma lucidum, Zingiber officinale, and grape seed extract possess antiemetic action against CINV and mint oil and ginger against RINV. In the following sections, the antiemetic and antinausea observations are addressed.
Ginseng
Among all medicinal plants, globally, ginseng is probably the most famous and extensively investigated plant. The generic name Panax derived from the Greek word Panakos means a panacea, a virtue ascribed to it by the Chinese, who consider it a sovereign remedy in almost all diseases. 12 Ginseng is a slow-growing perennial plant and the fleshy root bears resemblance to the human body. Because of this morphological feature, they are also known as “man-root.”13,14 There are 11 species of ginseng, but the most important and the well-studied species are the Panax ginseng (Asian, Korean, or Chinese ginseng) and Panax quinquefolius (also called American, Canadian, or North American ginseng).14,15 In the United States, where the market for medicinal botanicals is US$3 billion (CA$4.3 billion) and growing, ginseng is the top-selling herb among first-time herbal users and ranks third, surpassed only by Echinacea and garlic. 16
In the traditional Chinese system of medicine, ginseng is referred to as the ultimate tonic to benefit the whole body and has been used for more than 2000 years. 15 Ginseng has been used to improve the body’s resistance to stress, to increase vitality, increase general well-being, immune function, libido, and athletic performance. Preclinical studies suggest it to possess adaptogenic, anti-inflammatory, antineurological, hypoglycemic, antineoplastic, immunomodulatory, cardiovascular, central nervous system, endocrine, and ergogenic effects. 14 In traditional medicine, ginseng is also used for the alleviation of emesis. 15 Preclinical studies have shown that the Korean red ginseng (P ginseng) 17 and the American ginseng berry (P quinquefolius) 18 prevent cisplatin-induced nausea and vomiting in experimental animals. The following section addresses these aspects.
Korean Red Ginseng in the Prevention of CINV
In Korea, depending on the type of processing, ginseng is classified into fresh ginseng (<4 years old), white ginseng (4-6 years old and dried after peeling), and red ginseng (harvested when 6 years old, steamed, and dried). 19 Red ginseng is not skinned before it is steamed or otherwise heated and subsequently dried. 19 In the course of the steaming process, ginseng starch is gelatinized, causing an increase in saponin content. Traditionally, red ginseng has been used to restore and enhance normal well-being, and it is often referred to as an adaptogenic. 19
Kim et al 17 evaluated the antiemetic effect of Korean red ginseng total extract (aqueous) on cisplatin-induced nausea and vomiting using ferrets. In the cisplatin control, intraperitoneal (i.p.) administration of cisplatin (7.5 mg/kg) induced both nausea and vomiting. After a latency period of 1 hour, the episodes of nausea and vomiting initiated and reached a peak at 1.5 hours and persisted for 3 hours. Oral administration of the extract (0.3, 1.0, and 3.0 g/kg) reduced the cisplatin-induced nausea and vomiting in a concentration-dependent manner. With increase in the dose of cisplatin to 10 mg/kg, the nausea and vomiting were severe and the lower 2 doses of 0.3 and 1.0 g/kg were ineffective, whereas the highest dose of 3.0 g/kg exhibited significant antiemetic effects. In the time-dependent effect studies, the authors also observed that oral administration of 3.0 g/kg of the extract was effective only when administered 1 and 2 hours before cisplatin (7.5 mg/kg, i.p.) and that a further increase to 4 hours before cisplatin administration was not as effective as the other 2 earlier time points. 17
American Ginseng Berry in the Prevention of CINV
Studies have shown that pretreatment with ginseng berry extracts (50, 100, and 150 mg/kg body weight) and the phytochemical ginsenoside (2 and 5 mg/kg body weight) by intraperitoneal route 30 minutes before cisplatin (3 mg/kg body weight) resulted in a significant reduction in cisplatin-induced pica (Pica means eating of nonnutritive substances such as kaolin, a illness-response behavior in mice 20 and rats. 21 ) The phytochemical ginsenoside Re also caused a significant reduction in the intake of kaolin and the optimal protective effect was observed at 5 mg/kg. 18
The extract also decreased the amount of kaolin consumption at all time points (24, 48, 72, 96, and 120 hours) with differing levels of efficacy. The lowest dose of 50 mg/kg significantly attenuated the pica but did not improve the food intake, whereas the next higher dose of 100 mg/kg was effective in eliminating pica at 24 to 120 hours time point and also improved the food intake. With further increase in the dose to 150 mg/kg, pica was attenuated, especially when compared with the cisplatin alone cohorts at both 24 and 48 hours but showed a prolonged reduction in food intake from 24 to 96 hours. 18
The extract was observed to be effective in scavenging superoxide anion and hydroxyl radicals in vitro, thereby contributing to the protective effects at least in part.18,22 In vitro studies with the recombinant 5-hydroxytryptamine-3A (5-HT3A) receptor expressing xenopus oocyte have shown that the ginseng saponins (total saponin, panaxadiol saponin fraction, panaxatriol saponin fraction, and ginsenoside-Rb1 and -Rg1) inhibit the peak current induced by the agonist 5-HT on the 5-HT3A receptor in a dose-dependent, reversible, and voltage-independent manner. Of all the fractions, optimal results were observed with the panaxatriol saponin fraction, suggesting that some of the specific types of ginsenoside might have an antagonistic action against 5-HT3A receptor related to nausea and vomiting. 23
The observation that 100 mg/kg completely reversed pica and significantly improved food intake suggests the effectiveness of ginseng berry extracts in treating cisplatin-induced nausea and vomiting. The extract possess free radical scavenging and antagonistic action against 5-HT3A receptor suggest its possible use in the prevention of CINV. Detailed studies with other emetogenic antineoplastic drugs and also with other animal models of studies are required to confirm its efficacy before initiating clinical studies.
Scutellaria baicalensis Georgi in the Prevention of CINV
Commonly known as Baikal skullcap, Scutellaria baicalensis is a perennial herb of the family Lamiaceae with fleshy root, branched stems, papery leaves, purple-red to blue flowers, and black-brown ovoid nutlets.24-27 For more than 2000 years, it has been one of the most widely used herbs in the traditional Chinese herbal system of medicine.
24
Its use was first documented in the Shen Nong Ben Cao Jing circa 100
The roots are of use in the treatment of dysentery, diarrhea, allergic and inflammatory diseases, allergic rhinitis, to reduce cholesterol level, decrease blood pressures, atherosclerosis, hypertension, cholecystitis, hepatitis, cataract, diabetes complications, acute bronchitis, asthma, cold, cancer, bacterial and viral infections of the respiratory and the gastrointestinal tract, hepatitis, jaundice, tumor, and leukemia in the traditional Chinese medicine.26,28,29
With regard to inhibition of CINV, Aung et al 30 studied the antiemetic effects of hot water–soluble extract of the roots of S baicalensis against cisplatin-induced alterations in rats. When compared with the control animals, administration of cisplatin (3 mg/kg) decreased the food intake at all study time points (1, 2, 3 and 4 days post–cisplatin treatment) with the nadir being observed at 24 hours posttreatment. A progressive recovery in food consumption was observed from day 3 onward suggesting recovery. Cisplatin treatment also increased the intake of kaolin at all the time points, suggesting that the prolonged increase in pica consumption corresponds to a prolonged and delayed emetic response to cisplatin in humans. 31
Pretreatment with water-soluble extract of S baicalensis 30 minutes before cisplatin administration caused a decrease in the intake of pica at the 2 lower doses of 1 and 3 mg/kg. At a higher dose of 10 mg/kg the kaolin consumption increased, suggesting a possible pro-oxidant effect. However, there was no significant improvement in the food intake. The authors proposed that the observed beneficial effects may be because of the antioxidant effects of S baicalensis and its binding to 5-HT1A receptors.30,32 Similar results were also observed in another study and the reported in vitro free radical scavenging effects of the extract confirmed that the antioxidant action of the herb may be, at least in part, responsible for attenuating the cisplatin-induced nausea and vomiting. 22
Ganoderma lucidum (Fr.) Karst in the Prevention of CINV
Commonly known as Reishi mushroom, this white rot lamellaless macrofungus belonging to the phylum Basidiomycetes and family Polyporaceae is an important mushroom in the herbal system of medicine in China, Japan, and other East Asian countries.33,34 It is found to grow on the dried trunks of dead plum, Guercus serrata or pasonia trees in densely wooded mountains where humidity is high and the lighting is dim. 35 The Chinese name of this mushroom is Lingzhi, which means “spiritual potency.”33,34 This mushroom was also regarded by the Chinese as the “Medicine of Kings” and “mushroom of immortality” for more than 2000 years.33-35 Phytochemical studies have shown that the basidiocarp, mycelia, and spores of Reishi contain triterpenoids, polysaccharides, nucleotides, sterols, steroids, fatty acids, proteins/peptides, and trace elements.33,36
In traditional Chinese system of medicine, Reishi mushroom has long been used as a medicine to treat various human diseases. 36 These mushrooms are supposed to enhance intellectual capacity and memory, promoting agility, increase life span, inhibit tumor growth, reduce hypertension, modulate immune response, and increase hematopoietic activity.33-36 Pharmacological studies have shown that the Reishi mushrooms possess immunomodulatory, anti-atherosclerotic, anti-inflammatory, analgesic, chemopreventive, antitumor, chemo- and radioprotective, sleep promoting, antibacterial, antiviral (including anti-HIV), hypolipidemic, anti-fibrotic, hepatoprotective, anti-diabetic, anti-androgenic, anti-angiogenic, anti-herpetic, anti-oxidative, and radical-scavenging, anti-aging, hypoglycemic, estrogenic, and anti-ulcer properties.33-36
Experimental studies have shown that intraperitoneal administration of 1, 3, and 10 mg/kg G lucidum extract was effective in attenuating cisplatin-induced nausea and vomiting in the rat pica model. Additionally, the area under the curve for kaolin intake from time 0 to 72 hours for cisplatin only, 1, 3, and 10 mg of the extracts along with cisplatin treatment was 327.6, 264.0, 169.2, and 88.8 g/h, respectively. The reduction in the area under the curves of kaolin intake after 1, 3, and 10 mg/kg G lucidum extract administrations were 19.4%, 48.4%, and 72.9%, respectively. Additionally, when compared with the cisplatin alone cohorts, administering G lucidum extract was observed to be effective in increasing the intake of food and lacked adverse effects, such as restlessness or respiratory distress following the injections. Together, these observations suggest that in addition to reducing the nausea and vomiting, the extract also has a supportive effect in improving the general health and appetite in animals. 37
Grape Seed Polyphenols in the Prevention of CINV
For thousands of years, the fruit and the plant Vitis vinifera, commonly referred to as grapes have been grown and harvested for medicinal, nutritional, and economic value. The seeds of grapes have been a waste product of the winery and grape juice industry, but recent studies suggest that they possess immense health benefits.38,39 Depending on the variety of grapes, the seeds are reported to contain lipids, proteins, carbohydrates, and 5% to 8% polyphenols. The polyphenols in grape seeds are mainly flavonoids, including gallic acid, the monomeric flavan-3-ols catechin, epicatechin, gallocatechin, epigallocatechin, and epicatechin 3-O-gallate, and procyanidin dimers, trimers, and more highly polymerized procyanidins. 38
Scientific studies have shown that grape seed extract is a powerful antioxidant and its effect is 20 times greater than vitamin E and 50 times greater than vitamin C, 39 and it also protects the body from premature aging and various diseases. 38 Studies also indicate that because of its antioxidant effect, it is useful in promoting youthful skin, good cell health, elasticity, and flexibility. Animal studies have also shown that grape seed extract possess cardioprotective, anticancer, and anti-inflammation properties. 39 Proanthocyanidins are also reported to protect the body from sun damage, to improve vision, to improve flexibility in joints, arteries, and body tissues such as the heart, and to improve blood circulation by strengthening capillaries, arteries, and veins. 38
With regard to prevention of CINV, Wang et al 40 investigated the antiemetic effects of 3 grape seed extracts prepared in the investigators’ laboratory, obtained from a US-based dietary supplement company and from China. Phytochemical studies showed a great variation in the constituents of the 5 major constituents (gallic acid, catechin, epicatechin, procyanidin B2, and epicatechin gallate). The extract obtained from China had the highest level of polyphenols (194.21 mg/g), followed by the US-based dietary supplement company sample level (35.84 mg/g). The lowest total polyphenol content (27.27 mg/g) was observed in the sample prepared in the investigators’ laboratory. 40
Pretreatment with the grape seed extract (3 mg/kg), by intraperitoneal route reduced the cisplatin-induced pica from 0 to 72 hours but did not alter food intake or body weight. Conversely, with increase in the concentration to 10 mg/kg, all 3 extracts decreased the cisplatin-induced pica and with 30 mg/kg, the antiemetic effect of all the extracts was further reduced. Among the 3 samples studied, the investigators’ laboratory sample reduced emesis by 45%, the US-based dietary supplement company extract by 54%, and the extract obtained from China by 66%, clearly indicating that effect was proportional to the content of polyphenol in the extract. Additionally, the area under the curve for kaolin intake from time 0 to 72 hours for cisplatin only, laboratory sample, US company sample, and Chinese company samples were 518.0, 284.0, 238.2, and 178.7 g/h, respectively. 40
Mint Oil in the Prevention of RINV
Mint is a broad term given for a group of aromatic perennial herbs belonging to the genus Mentha and the family Labiatae. It is one of the most important culinary and medicinal plants in the world. In various traditional medicines, mint is used as a stomachic, tonic, carminative, antispasmodic, and anthelmintic. 41 Mint oil extracted from the stem, leaves, and flowers of the plant by steam distillation is used all over the world for flavoring, cosmetic, and medicinal purposes.41,42 The oil is traditionally used in relieving digestive ailments, for irritable bowel syndrome, headache, non-ulcer dyspepsia such as indigestion, gas problem, and acidity. 43 It is also a main ingredient for Ayurvedic medicines (eg, Dabur’s “Pudin Hara” used for gastric disturbances. 43
Scientific studies have shown that the mint oil possesses analgesic, anti-inflammatory, antiseptic, anti-infectious, antimicrobial, antispasmodic, astringent, carminative, digestive, expectorant, febrifuge, fungicidal, nervine, vasoconstrictor, decongestant, stimulant, cognitive enhancer, stomachic properties and is also effective against irritable bowel syndrome.41-43 At the biochemical level, mint oil is reported to modulate calcium channel–dependent processes in intestinal, neuronal, and cardiac preparations.41-43 The oil is also reported to possess neuromodulatory and performance-enhancing properties. 44
Studies have shown that mint oil (Mentha spicata Linn.) was effective in mitigating radiation-induced conditioned taste aversion (CTA), a phenomenon understood to be controlled in rodents by the same pathways that control nausea and vomiting in humans. 45 It was observed that the intraperitoneal administration of mint oil (5, 7.5, 10, 12.5, and 15% v/v) 1 hour before exposure to 2 Gy of whole body irradiation showed significant decrease in CTA at all doses, when compared with the 2 Gy radiation control at all time points (1, 2, 3, 4, and 5 days post irradiation). However, the best effect was observed as follows 10% > 12.5% > 15% > 7.5% > 5%. 45
Mechanistically, it is quite possible that the free radical scavenging and the antioxidant effects of mint may have contributed to the reduction in CTA. Studies have also shown that rotundifolone, an active constituent of mint oil, mimics the effects produced by calcium channel blockers, and thus can neutralize the injurious effects of biogenic amines such as histamines and 5-HT and also modulate vagal activity and reduce intestinal motility and contractility. 46 Mint oil is also known to exert neurobehavioral effects, increase alertness, sharpen mental process, and rejuvenate a sluggish and tired mind. 47 All these properties may have contributed to the observed effect.
Ginger in the Prevention of CINV and RINV
The rhizome of Zingiber officinale (family Zingiberaceae), commonly known as ginger, is an important herb in the various traditional systems of medicine. 48 It is an integral part of several medicinal formulations in Ayurveda, the traditional system of Indian medicine. In various traditional systems of medicine, ginger is reported to be a carminative, diaphoretic, antispasmodic, peripheral circulatory stimulant, astringent, appetite stimulant, anti-inflammatory agent in addition to being useful in treating cold, headaches, arthritis, rheumatological conditions, and muscular discomfort.48-50
Studies have shown that ginger possesses antimicrobial, antischistosomal, anti-inflammatory, antipyretic, antioxidative, hypoglycemic hepatoprotective, diuretic, and hypocholesterolemic effects.49,50 Ginger is also beneficial to the gastrointestinal tract, to increase bile secretion, and to prevent gastric ulcers.49,50 Scientific studies have also shown that ginger prevents nausea and/or emesis resulting from pregnancy, motion sickness, postoperation chemotherapy, and radiation, thereby validating the traditional observations and emphasizing its broad-spectrum antiemetic effects.49,50 In the United States, ginger is recommended to relieve and prevent nausea. 48
Preclinical studies have shown that ginger possesses antiemetic effects and prevents gastric emptying against the highly emetogenic cisplatin. Sharma et al 51 evaluated the anitemetice effects of various ginger extracts (acetone, 50% ethanolic and aqueous) against emesis induced by 3 mg/kg cisplatin in the healthy mongrel dogs with the 5-HT3 receptor antagonist granisetron as a known control. The authors observed that the acetone and 50% ethanolic extract at the doses of 25, 50, 100, and 200 mg/kg per os (p.o.). exhibited significant protection whereas aqueous extract at these doses was ineffective against emesis. The acetone extract was more effective than ethanolic extract but was less effective than granisetron. 51
The acetone and 50% ethanolic extract of ginger in the doses of 100, 200, and 500 mg/kg (p.o.) and fresh ginger juice (2 and 4 mL/kg) were also investigated against cisplatin effect on gastric emptying in rats. It was observed that all the 3 ginger preparations reversed the cisplatin-induced delay in gastric emptying, and the ginger juice and acetone extract were more effective than the 50% ethanolic extract. 52 The reversal produced by the ginger juice was better than the 5-HT3 receptor antagonist ondansetron, whereas that of the acetone extract of ginger was similar to ondansetron. 52 Together, these studies suggest that ginger possesses antiemetic effects and also reduces the gastrointestinal side effects of cisplatin.51,52
Gingerol (Figure 1), the active principle of raw ginger, was also investigated for its antiemetic effects against the cisplatin (7.5 mg/kg i.p.)-induced emesis in minks. 53 Pretreatment with gingerol (50, 100, or 200 mg/kg, i.g.) caused a concentration-dependent reduction in the number of retching and vomiting incidents during the 6-hour observation period. The effects of 200 mg/kg of gingerol and the positive control ondansetron were almost similar. 53 Immunohistochemical studies showed that gingerol caused a dose-dependent suppression in the levels of substance P and NK1 receptors in area postrema and ileum. 53

Structure of gingerol, an important phytochemical present in ginger rhizome
Studies by Sharma et al 54 have shown that the administration of the hydroalcoholic extract of ginger 1 hour before exposure to 2 Gy of γ irradiation was effective in blocking the saccharin avoidance response for 5 posttreatment observational days. The study showed that intraperitoneal administration of the extract (50, 100, 150, and 200 mg/kg body weight) to male rats caused a dose- and time-dependent protective effect and that the best effects were observed at 200 mg/kg body weight. 54 It was also observed that in the female rats (administered with 150, 200, 250, and 300 mg/kg body weight) the optimal effect was observed at 250 mg/kg by intraperitoneal route, confirming the existence of gender difference in relation to behavioral responses or differential metabolism. 55 The authors hypothesize that the observed protective effects of ginger may be because of its antioxidant properties.54,55
The antiemetic studies with ginger in humans have been mixed and contradictory. In one of the earliest studies, Pace 56 investigated the antiemetic effect of ginger in leukemic patients receiving chemotherapy. The patients were randomized to receive oral ginger or placebo in addition to prochlorperazine. The results showed that when compared with those receiving placebo, a significant reduction in nausea was observed in patients receiving ginger. 56 Furthermore, pilot studies by Meyer et al 57 and Pecoraro et al 58 have also supported ginger’s use as an antiemetic in patients undergoing chemotherapy.
Additionally, experiments have confirmed that ginger is effective in reducing nausea and vomiting induced by low-dose cyclophosphamide in combination with other anticancer drugs causing mild emesis. 59 However, the antiemetic efficacy of ginger was found to be equal to that of metoclopramide but inferior to that of ondansetron. 59 Combining high-protein meals with ginger also reduced the chemotherapy-induced delayed nausea and the use of standard antiemetic medications in patients with cancer. 60
In a double-blinded crossover study, Manusirivithaya et al 61 have observed that the addition of ginger to standard antiemetic regimen of gynecologic oncology patients receiving cisplatin offered no advantage in reducing nausea or vomiting in the acute phase of cisplatin-induced emesis, whereas in the delayed phase it was effective and that the beneficial effect was comparable to that of metoclopramide.
Studies have also shown that the administration of ginger (0.5, 1.0, or 1.5 g) along with 5-HT3 receptor antagonists reduced the chemotherapy-induced nausea in patients undergoing treatment for breast, alimentary, and lung cancers. 62 The optimal effect was observed for the cohorts who had received 0.5 or 1.0 g of ginger. 62 Very recently, Pillai et al 63 have also observed that ginger root powder was effective in reducing the severity of acute and delayed CINV when provided as a adjunct to ondensetron and dexamethasone in bone sarcoma patients receiving the highly emetogenic chemotherapy containing cisplatin/doxorubicin. Together, these reports clearly suggest the usefulness of ginger as an adjuvant to the conventional antiemetic agents.
Contradictory to these observations is the recent study by Zick et al 64 suggesting that ginger offers no benefit in reducing the prevalence or severity of acute or delayed CINV when combined with 5-HT3 receptor antagonists and/or aprepitant. Furthermore, the authors also observed that the participants who took both ginger and aprepitant had more severe acute nausea than participants who took only aprepitant, suggesting a possible antagonism. 64 Overall, these observations clearly suggest that more observational studies, with a larger sample size, are needed to confirm the encouraging preliminary data on ginger safety.
Conclusions
Numerous preclinical studies in the past 2 decades have demonstrated unequivocally that traditionally used plants such as S baicalensis, Korean red ginseng, American ginseng berry, G lucidum, ginger, and grape seed extract possess antiemetic actions against CINV, and mint oil and ginger against RINV. Most of the antiemetic studies against CINV have been with cisplatin and future studies are required with other chemotherapeutic agents and their combinations that induce emesis. This would clearly indicate the spectrum of efficacy of these plants in preventing CINV. The outcomes of such studies may be useful for the clinical applications of these plants and their phytochemicals as antiemetic agents and may open up a new therapeutic avenue.
Most of the plants studied have been used in traditional systems of medicine for many centuries. These plants are consumed by humans and are reported to be devoid of toxic effects at the permissible doses. However, the observation that some of the plants possess pro-oxidant effects necessitates performing detailed toxicological studies to understand the antioxidant and pro-oxidant concentrations of these plants. Some of the administration has been by intraperitoneal route, which is not the preferred route for humans. Studies should be planned to test the efficacy of these plants when administered through oral route. Experimental studies should also be performed with tumor-bearing animals to rule out the possibility of interference of these plant compounds with the antineoplastic activity of the emetogenic anticancer agents. Only when these studies are performed and satisfactory results obtained, can the value of these plants as antiemetic agents be appreciated.
From the contradictory clinical observations with ginger and the animal studies with grape seed extracts it is very evident that the concentration of phytochemical plays a major role in the observed pharmacological effects. Therefore, studies should also be performed with well-characterized and standardized extracts. Studies should also be aimed at identification of the bioactive compounds present in the respective plants that are responsible for the antiemetic effects. Currently, only gingerol and ginsenoside, the active principles of raw ginger and ginseng, respectively, have been reported to possess antiemetic effects. Similar studies should also be performed with other phytochemicals. When these studies are performed, it will clearly indicate the potential of these plants as possible nontoxic antiemetic agents against chemotherapy- and radiation-induced nausea. Till then, caution needs to be taken especially with the plants that exhibit pro-oxidant effects (at higher doses) as their use can further increase emesis and aggravate side effects, thereby affecting the treatment response/regimen and survival of the patient.
Footnotes
Acknowledgements
Mr Raghavendra Haniadka, Dr Princy Louis Palatty, and Dr Manjeshwar Shrinath Baliga are grateful to Rev Fr Patrick Rodrigus (Director), Rev Fr Denis D’Sa (Administrator), and Dr Jaya Prakash Alva (Dean). Dr Rajesh Arora is grateful to Dr W Selvamurthy, Chief controller Research and Development (Life Sciences and International Collaboration) for support and encouragement.
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.