
Abstract
Hypotheses. The authors hypothesized that the use of alternative medicine, in the form of Chinese medicine (CM), among patients in the continuing care phase of nasopharyngeal carcinoma (NPC) in Taiwan is higher than the use in a matched control group of noncancer individuals. Study design. This was a case-control study. Methods. Using a population-based claim database, the authors identified 181 long-term survivors of NPC and 905 matched controls. They obtained information on CM use and associated cost as outcome measures. Descriptive analysis and regression models were applied to examine the association between NPC and the outcome measures. Results. The unadjusted CM initiation (34% vs 32%; P = .54), intensity of use (2.15 vs 1.73 visits; P = .37), and cost (US$79 vs US$58; P = .16) were higher for patients in the NPC group than for those in the control group. Regression analyses suggested that the NPC group had significantly more CM visits (1.01; 95% confidence interval = 0.07-1.96), and more than 50% of these visits were related to cancer. Conclusion. The authors confirmed their hypotheses that the use of CM in the continuing care phase by patients with NPC in Taiwan was higher than the use in their matched, noncancer counterparts. These findings suggest that current clinical surveillance strategies for NPC might not meet patients’ physical and emotional needs.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a rare tumor in the West, with the incidence as low as 1 per 100 000 people in the United States and Europe. The incidence of NPC is much higher in certain parts of Asia: in Taiwan, Hong Kong, and southern China, the rate of incidence is close to 30 per 100 000. 1 NPC is the 10th leading invasive cancer among men in Taiwan, accounting for 1116 incident cases and 611 deaths in men in 2006. 2 NPC is more prevalent in men, with a 2 to 3 versus 1 male to female incidence ratio.1,2 Overall, the prognosis for NPC is good, with 2-year local relapse-free survival observed in more than 90% of patients.1,3 However, long-term complications such as chronic xerostomia (dry mouth) are prevalent among survivors of NPC, 1 and supportive care is often the only option available for patients treated with Western medicine.
Complementary and alternative medicine (CAM), defined by the US National Institutes of Health as “a group of diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine,” is becoming increasingly popular worldwide.4-6 By this definition, traditional Chinese medicine (CM) can be considered a form of CAM.4,5,7 To date, the efficacy of CAM in oncology care remains controversial. 5 Despite being controversial, the use of CAM (including CM) has been documented in many studies involving cancer patients and long-term survivors of cancer.8-15 A recently published systematic review reported that the rate of CAM use in the treatment of cancer was in the range of 30% to 80%. 6
The role of CM in the care of patients with NPC is largely unknown. Although studies have suggested that CM is an efficacious concomitant therapy for NPC in the initial phase of care (ie, within 12 months of diagnosis), this finding has not been confirmed in clinical trials.16,17 For long-term survivors of NPC entering the continuing care phase, there is evidence of a favorable risk–benefit ratio associated with some forms of CAM (eg, acupuncture); however, the use of herbs or other CM for patients with NPC in the continuing care phase is more controversial. 7 Despite a moderate to high prevalence of CAM use documented in many studies of cancer patients, a study focusing on the use of CAM among prostate cancer patients has reported a reduced use 2 years after they were diagnosed with cancer. 11 The use pattern of CAM among NPC patients in the continuing care phase has not been explored in the literature. Currently, neither CAM nor CM is included in the treatment guidelines for NPC, as publicized by professional societies such as the National Comprehensive Cancer Network, or as local practice guidelines in Taiwan.18,19
The literature suggests that an individual with cancer seeks CAM for various reasons, including dissatisfaction with conventional medicine or health providers, satisfaction with CAM, because the use of CAM is congruent with his/her own values and culture, because of a potentially favorable risk–benefit ratio associated with CAM, and a desire to improve physical and mental health, reduce treatment-related side effects, and have a sense of control over one’s illness.7,20-28 Studies have found that cancer patients may rely on CAM to reduce treatment-related side effects.26,28 In addition, Mao et al 23 concluded that a major driver for the use of CAM among cancer survivors was unmet physical and emotional needs. Other researchers found that the use of CAM among cancer patients and survivors was more driven by nonclinical factors, such as cultural congruence or for the purpose of empowerment and personal autonomy so as to cope with the feeling of helplessness resulting from the cancer diagnosis. 27
Compared with physicians and patients in many other countries, those in Taiwan are more familiar with CM. The rate of CM use was 28 500 per 100 000 residencies in Taiwan in 2007. 29 In addition, CM has been a covered service under the National Health Insurance (NHI) of Taiwan since its inception. CM services reimbursed by the NHI include CM consultation, herbal medication, acupuncture, muscle strain therapy, and dislocation therapy. 30 These factors make Taiwan an ideal environment in which to study the use of CM among patients with NPC. In this population-based study, we made use of a retrospective case-control study design to explore our hypotheses that the use of alternative medicine, in the form of CM, is increased in the continuing care phase of patients with NPC in Taiwan.
Methods
Data Source
The primary data used in our study were extracted from the NHI Research Database in Taiwan. The NHI program, established in 1995, is a single-payer, compulsory social insurance program that provides insurance coverage to all citizens in Taiwan. Services covered under the NHI include outpatient visits, hospitalization, home nursing care, certain screening and preventive services, laboratory tests and diagnostic imaging, dental care, and traditional CM.31,32 As of 2007, 22.6 million of Taiwan’s 22.96 million people were enrolled in this program. Taiwan’s National Health Research Institutes (NHRI) deposit the enrollment file and original claims data for all services reimbursed by the NHI into a single database, the NHI Research Database, which allows researchers to link enrollment records and claims data. To facilitate clinical, epidemiological, and health services research using these data, the NHRI de-identifies personal information in the data and makes the database accessible to researchers in Taiwan through a process of data acquisition and approval. 33 As of December 31, 2009, the NHI Research Database had been used in more than 200 studies. 33
For this study, we used the 1998-2007 ambulatory care expenditures by visits (CD) and inpatient expenditures by admissions (DD) files from the Longitudinal Health Insurance Database 2005 (LHID2005). The LHID2005 is a subset of the NHI Research Database that collects all the current and previous claims data of 1 million beneficiaries who are randomly sampled from the 2005 enrollment file. We also used the registry for catastrophic illness patients (HV; 1997-2007) and the traditional CM data set (1997-2007). 33 Following the data linkage strategy used to create the LHID2005, we constructed the personal identifiers with a combination of 3 person-level factors: personal ID, gender, and date of birth. 33
Study Design and Selection of Study Sample
We used a retrospective, matched case-control study design to examine the use of CM in the continuing care phase among long-term survivors of NPC. We identified patients in the case and control groups of the study following the strategies illustrated in Figure 1. Briefly, first, we identified NPC cases as patients with 2 or more office visits on different dates that were coded with ICD-9 (International Classification of Diseases, 9th revision) codes indicative of NPC from the LHID2005. Because cancer is one of the diseases covered by the catastrophic illness program, which waives copayment for expenses related to the disease that establishes a patient’s eligibility (although a registration fee is still required), the date that a patient with cancer became eligible for the program is a close approximation of the date on which the diagnosis was confirmed. Then, we limited the NPC cases to those that could be linked to the registry for catastrophic illness patients’ (HV) file, so that we could establish an index date (ie, date of NPC diagnosis). On establishing the index date, we identified the long-term survivors as those who survived 3 or more years after the initial diagnosis of NPC and characterized the continuing care phase as the 12-month duration in the second year after the initial diagnosis of NPC. 34 Finally, we constructed a matched control group of individuals without cancer using the frequency-matching method.35,36 The control group was matched with the NPC group by age, gender, and the region of residence.
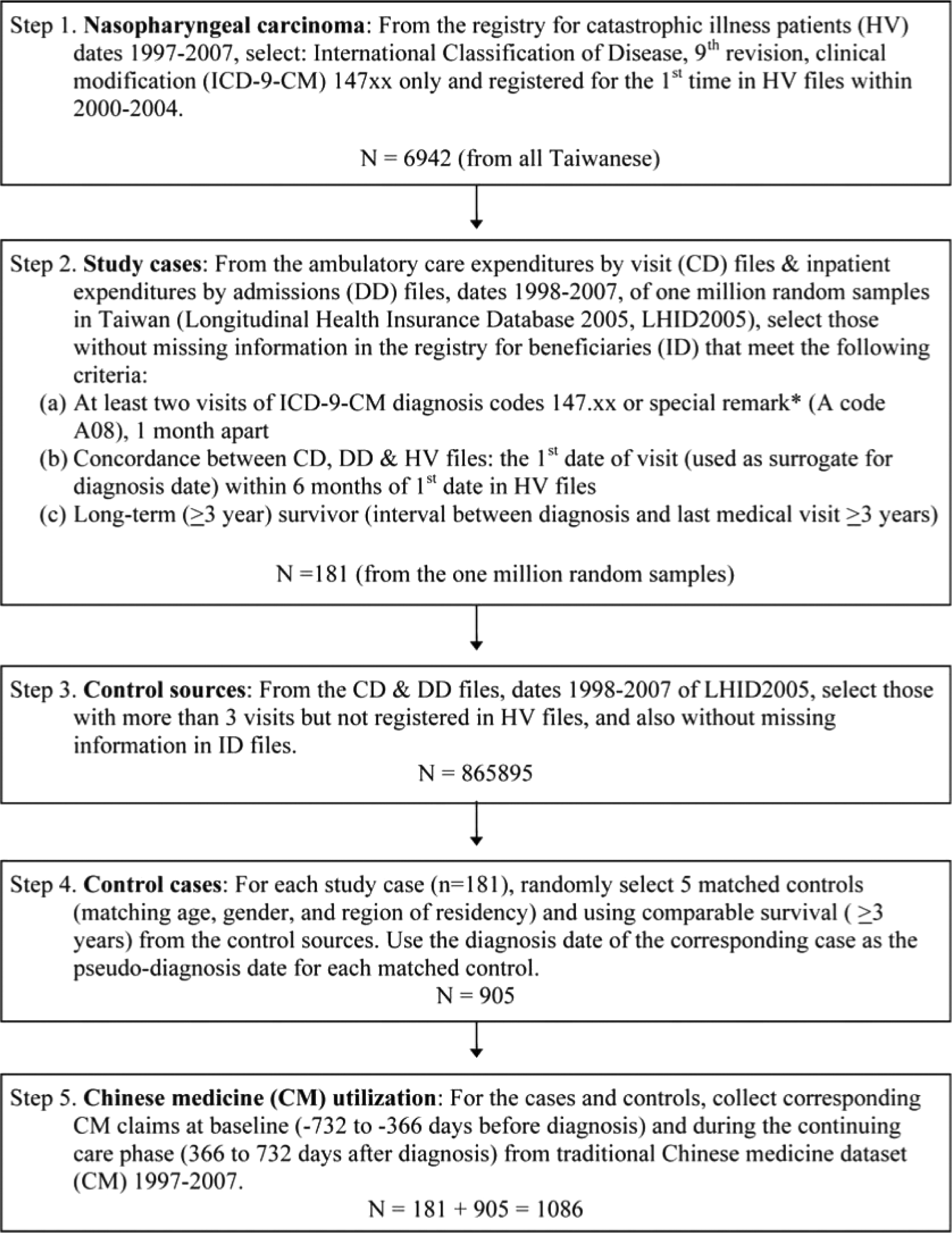
Selection of study population and collection of corresponding Chinese medicine use data
Study Variables
We identified CM-related visits from the claims data and quantified the use of CM in the continuing care phase in 2 ways: initiation and intensity of use. We used a binary variable to capture whether a patient had initiated the use of CM at any time during the continuing care phase and measured the intensity of use by the total number of CM office visits in that duration. In addition, we estimated costs associated with CM use during the 12-month continuing care phase. We obtained cost information from the total payment variable in the CM data set, inflated all costs to the 2008 NT$ (New Taiwan dollar) based on the consumer price index in Taiwan, 37 and converted the costs to US dollars using the purchasing power parity index. 38
Explanatory variables in multivariate analyses included age, gender, socioeconomic status (SES), the geographic region of the patient’s residence as reported from the enrollment file, time period (year of diagnosis), and comorbidity. Age at diagnosis was dichotomized as elderly (≥65 years old) versus nonelderly (<65 years old). Following the procedures established in previous studies,30,39 we classified the residency of our study population according to 5 regions: the Taipei metropolitan region, and the north, central, south, and Kaohsiung and east regions. We characterized the SES of our study population as 1 of 2 groups according to income class: those with low income (household monthly income equal to or lower than minimal wage or without a well-defined monthly wage, with the exception of farmers and fishermen) versus others. This is similar to a strategy used in a previous study based on the NHI Research Database. 30 We calculated a patient’s comorbidity using an algorithm developed by Klabunde et al40-43 that was modified for use with the NHI claims data. 39 We quantified prior CM use as a binary variable indicating whether a patient had exposure to CM in the duration of 13 to 24 months prior to the diagnosis of NPC and included this variable as an additional explanatory variable to capture a patient’s experience with CM prior to his or her cancer diagnosis. We anticipated that patients with prior exposure to CM might be more likely to view CM as an alternative source of treatment when seeking care.
Statistical Analysis
First, we described the difference in CM use between the NPC and the control groups in bivariate analyses. Then, we used logistic regression, negative binomial regression, and the generalized linear model (GLM) with the γ family of distributions and a log-link function to examine factors associated with the initiation of CM, the intensity of CM use, and the cost of CM, respectively, in multivariate analyses. We selected a negative binomial model over the commonly used Poisson model in consideration of the overdispersion of the count data that characterized CM-related visits. The specification of the GLM also accounted for the skewed distribution typically observed in medical cost data.44,45 A descriptive analysis was also used to identify the primary diagnosis reported at CM visits and the total visits and costs in the continuing care phase to compare CM users versus nonusers. To determine whether the findings of our study were sensitive to the choice of control group, we performed sensitivity analyses for a second control group generated by the same program, which was used to identify a random sample of a matched control group. Statistical significance was defined as a P value <.05. We used SAS for Windows, version 9.0 (SAS Institute, Cary, NC), for data management and Stata SE, version 10.1 (StataCorp, College Station, TX), for statistical analyses.
Results
Descriptive Statistics
The characteristics of our study sample are described in Table 1. As shown, the matching algorithm yields identical distributions in age, gender, and geographic regions between individuals in the NPC and the matched control groups. Compared with those in the control group, we found a significantly higher proportion of individuals in the NPC group with a comorbidity score of 1 or higher (25% vs 34%; P = .0076). No statistically significant difference was found in the prior experience with CM and income classes between these 2 groups. The bottom 3 rows in Table 1 compare the initiation and intensity of CM use and CM-related costs between the NPC and control groups in univariate analyses. We found that a higher proportion of individuals in the NPC group initiated the use of CM during the 1-year study period; however, the difference between the 2 groups was not statistically significant (34% vs 32%; P = .54). The NPC group was also associated with a higher number of CM-related visits (2.15 vs 1.73; P = .37) and higher costs (US$79 vs US$58; P = .16) than the control group, although none of the observed differences was statistically significant.
Characteristics of Patients in the NPC and Control Groups

Abbreviations: NA, not applicable; NPC, nasopharyngeal carcinoma; SD, standard deviation; CM, Chinese medicine; USD, 2008 US dollars.
χ2 test.
Missing n = 2.
t test.
Multivariate Analysis
Table 2 presents the results of logistic regression for factors associated with the initiation of CM use. It shows that the higher odds ratio (OR) associated with the NPC group was not statistically significant (OR = 1.11; 95% confidence interval [CI] = 0.78-1.58), whereas female gender, prior experience with CM, and higher comorbidity scores were significantly associated with CM use.
Logistic Regression for the Initiation of CM Use in the Continuing Care Phase

Abbreviations: CM, Chinese medicine; CI, confidence interval; NPC, nasopharyngeal carcinoma; SES, socioeconomic status.
P < .05.
Table 3 summarizes the findings of negative binomial regression to examine the intensity of CM use in terms of the total number of CM visits. Instead of presenting the regression coefficients, we converted the estimates into marginal effects, so that we could assess the effect of each covariate as absolute counts (the number of office visits) rather than relative counts. We found positive associations to be statistically significant for the intensity of CM use and NPC status (1.01 visits; 95% CI = 0.07-1.96), female gender (1.35 visits; 95% CI = 0.54-2.16), and prior CM use (2.23 visits; 95% CI = 1.30-3.15). In addition, we found that individuals who resided in the Taipei metropolitan area had significantly lower numbers of CM visits than those who resided in the Kaohsiuing and east region (−0.72 visits; 95% CI = −1.27 to −0.16).
Factors Associated With Total Number of CM-Related Office Visits in the Continuing Care Phase, Negative Binomial Analysis

Abbreviations: CM, Chinese medicine; CI, confidence interval; NPC, nasopharyngeal carcinoma; SES, socioeconomic status.
P < .05.
Table 4 shows the findings of the cost analysis using the GLM. We found statistically significant higher costs in 3 groups of individuals: patients with NPC (US$40.64; 95% CI = 2.94-78.33), women (US$41.56; 95% CI = 10.14-72.98), and prior CM users (US$76.85; 95% CI = 46.96-106.75).
Generalized Linear Model of Costs Associated With Chinese Medicine Use in the Continuing Care Phase

Abbreviations: CI, confidence interval; NPC, nasopharyngeal carcinoma; SES, socioeconomic status; CM, Chinese medicine.
P < .05.
Sensitivity Analysis
We generated another random sample of a control group and compared their CM use with that of patients in the NPC group. This comparison shows that the initiation of CM use (32% vs 30%), the intensity of use (1.73 vs 1.71 visits), and costs (US$58 vs US$58) were similar to those observed in the initial control group, suggesting that the findings we reported were unlikely to be driven by the selection of control groups.
Comparisons Between CM Users and Nonusers
To better understand the clinical presentation associated with patients’ office visits that led to CM use, we listed the top 10 most frequently reported primary diagnosis codes in the claims of CM visits for the NPC and control groups. Figure 2 shows that a large proportion of CM claims among patients in the NPC group listed NPC or head and neck cancer as the primary diagnosis. Among other claims, long-term complications of NPC, such as polydipsia (4%), cervicalgia (3%), and tinnitus (2%), were found in the top-10 list for patients in this group but not for those in the control group. We also compared the overall patterns of health care use between the 2 groups. Table 5 shows that, overall, CM users had a higher number of visits and annual medical costs than nonusers. The differences between CM users and nonusers were more pronounced among patients in the NPC group. Among patients with NPC, compared with those who did not use CM in the continuing care phase, CM users had 15 more visits (43.92 vs 28.88) and more than US$1600 higher total medical costs in that 12-month duration. The magnitude of the difference was much smaller in the non-NPC group (8.6 more visits and US$167 higher medical costs).

Distribution of the top 10 primary diagnosis codes for Chinese medicine claims: nasopharyngeal carcinoma (NPC) group versus control groupa
Total Number of Visits and Medical Costs, by CM Use and NPC Status

Abbreviations: CM, Chinese medicine; NPC, nasopharyngeal carcinoma; SD, standard deviation.
2008 US dollars.
Discussion
In this retrospective case-control study of 181 long-term survivors of NPC and their age-, gender-, and region-matched noncancer controls (n = 905), we found that after adjusting for demographic, socioeconomic, and clinical characteristics as well as for the time trend, patients in the NPC group had significantly more frequent CM visits (1.01 visits) and higher costs (US$40.6) related to CM use in the continuing care phase but were not significantly more likely to initiate CM use than those in the non-NPC group.
Although a large number of population-based studies of treatment/use pattern as well as the associated factors have been based on claims data in the United States, these data are not ideal to examine the use of CM because most insurance plans in the US provide limited coverage of CM use. Thus, the rate of CM use estimated from the US claims data is likely to be grossly underreported because these data are not able to capture self-paid use of CM. If the use of CM can be viewed as an indication for unmet health needs, an underreported use pattern would then fail to raise physicians’ awareness of important symptoms or conditions that require medical attention. The more favorable reimbursement environment for CM in Taiwan’s NHI program means that claims data in the NHI Research Database is more useful for examining the use of CM as compared with claims data in the United States. Despite the advantages of using the NHI claims data in studies related to CM, the data have been underutilized for that purpose. Previous studies using the NHI Research Database have focused on the overall prescription pattern 46 and use among patients with specific diseases or conditions, such as schizophrenia, chronic hepatitis, and pregnancy.47-49 Only 2 studies have used the NHI claims database to investigate the use of CM in relation to cancer; however, of these, 1 study examined a potential pathological role of CM in urinary tract cancer, whereas the other was a cross-sectional study of CM use among patients with prostate cancer.50,51 To our knowledge, this is the first study to use the NHI Research Database to examine CM use among long-term cancer survivors and the first to explore the use of CM in the continuing care phase of NPC.
In a study that examined CM use in the general population of Taiwan, Chang et al 30 reported that female gender, middle age (45-54 years), and residing in the central and southern regions of Taiwan were associated with a higher likelihood of CM use, whereas an association between disease severity (including NPC) and CM use was not statistically significant. Our findings were similar: We found that women were significantly more likely to use CM, and patients with NPC were not any more likely to use CM than their matched noncancer counterparts. In addition, we found that prior experience with CM and greater comorbidity were significant predictors of CM use. The positive association between CM use among NPC patients in the continuing care phase and prior CM use could be explained by cultural congruence, in the sense that the use of CM is consistent with patients’ own culture and value judgment, a finding consistent with a previous study. 27 It should be noted that while findings from our study can potentially provide important information regarding CM use for NPC patients outside Taiwan, factors such as cultural congruence imply that there would be a higher use rate of CM by NPC patients in Taiwan than in other countries.
Another plausible explanation of higher CM use among survivors of NPC is unmet health care needs. Although not directly verifiable from claims data, the top 10 diagnoses listed in Figure 2 and the patterns of total health care use, in terms of both the number of visits and costs (documented in Table 5), shed some light on this discussion. The ICD-9 codes frequently associated with CM claims (Figure 2) indicate that, apart from cancer, 3 of the diagnoses on the top 10 list for the NPC group are symptoms commonly associated with chronic complications that arise secondary to irradiation treatment of the head and neck. Specifically, we found that more than 50% of CM visits for NPC patients in the phase of continuing care were associated with cancer diagnosis or treatment-related complications. These symptoms include polydipsia (excessive thirst in response to radiation damage to the salivary gland and resulting xerostomia), and cervicalgia and tinnitus (likely consequences of radiation-induced fibrosis and inflammation), which are frequently encountered in this patient population.1,52 The substantially higher total number of visits and medical costs found among CM users compared with nonusers in the NPC group could also indicate more frequent use of health care resources in an effort to resolve unmet health needs. Although a similar pattern was also observed in the control group, the magnitude of difference between the CM users and nonusers was much larger in the NPC group, suggesting a higher level of unmet health care needs among survivors of NPC.
Although the evidence-based literature does not clearly support the use of CAM in a clinical setting, some clinical trials have established CAM’s effectiveness in reducing pain and anxiety among cancer patients.53,54 As more rigorous investigations of CAM are undertaken, its use among cancer patients and survivors may increase. CAM is relatively inexpensive compared with conventional Western medicine. Using insurance claims data from a large provider in the United States, Lafferty et al 55 reported that CAM accounted for approximately 1% of total expenditures in the continuing care phase for cancer patients. We found that CAM accounted for 2.5% of the total medical expenditure during the continuing care phase for patients with NPC. The use of CM to alleviate long-term complications for individuals with NPC might lead to a favorable cost–benefit ratio. Given the public’s growing interest in complementary and alternative treatments, future studies of the comparative effectiveness and cost-effectiveness of CAM will be of value.
As a retrospective analysis of claims databases, our study has several limitations. First, we selected a group of patients with NPC from a nationally representative sample (ie, LHID 2005) of the general population of Taiwan. 33 Therefore, although our study sample should be representative of the Taiwanese population, it is possible that it is not representative of the larger cohort of individuals with NPC in Taiwan. Second, we were not able to fully explore the specific reasons for which patients sought CAM because patients with NPC, who represented a large number of the CM claims, had a cancer-related primary diagnosis code and unreported secondary diagnosis codes in the vast majority of claims. Furthermore, diagnosis codes alone did not provide information regarding patients’ motives behind the use of CM; therefore, we were not able to learn from the data whether patients’ use of CM was meant to substitute or complement conventional therapies. Third, the validity of a cancer diagnosis based on claims data in the NHI Research Database has not been confirmed; however, the accuracy of that database has been validated for another disease diagnosis. 56 Fourth, claims data typically contain limited information on patient-reported outcomes (such as symptom burden, quality of life, or patient satisfaction) and survival status. Although a report from the UK House of Lords identified the role of CAM in achieving patient satisfaction 5 and clinical trials have shown CAM to be effective in reducing pain and anxiety in cancer patients,53,54,57 we were not able to determine whether increased use of CM was associated with better health outcomes among patients with NPC in the continuing care phase.
Despite these limitations, this study uniquely contributes to the literature by documenting the increased costs and use patterns of CM among long-term survivors of NPC. The observation that approximately 34% of these patients sought care with CM and that more than 50% of the CM visits had a diagnosis of cancer or a long-term complication associated with cancer or cancer treatment in the continuing care phase suggests that the needs of NPC survivors might not be satisfied through conventional clinical strategies currently in use.
Conclusion
We confirmed our hypotheses that the use of CM is increased in the continuing care phase of patients with NPC in Taiwan. Our findings suggest that current clinical surveillance strategies for NPC might not meet patients’ physical and emotional needs. Further research is needed to explore whether CM, or more broadly CAM, can bring additional benefits to these patients.
Footnotes
Acknowledgements
The authors thank Ms LeeAnn Chastain for her editorial contributions.
Authors’ Note
This study is based on data from the NHI Research Database provided by the Bureau of National Health Insurance and managed by the NHRI in Taiwan. The interpretations and conclusions do not represent those of the Bureau of National Health Insurance or the NHRI.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was partly supported by the China Medical University Hospital, Taiwan (Grant Numbers DMR-98-132), and the Department of Health, Taiwan (Grant Number DOH100-TD-C-111005).