
Abstract
Management of residual deformity in patients with Charcot Neuro-osteoarthropathy represents a therapeutic challenge. The midfoot is the most frequently affected area, leading to the typical rocker-bottom deformity. Surgical exostectomy in these areas of bony prominences offers a non-reconstructive method to remove pressure and allow ulcers to heal or prevent their development when conservative measures fail. This review includes a total of 11 studies, aimed to assess the outcome of exostectomies in the prevention and recurrence of ulcers under the bony prominence in patients with Charcot midfoot and its main complications. Exostectomy was successful in 60% of cases after the first surgery and in 90.7% of cases in total. The procedure, when done below the lateral column, seems to have a higher number of diverse complications. This fact must be taken into account when performing this procedure.
Keywords
Introduction
Charcot Neuro-osteoarthropathy (CNO) or Charcot foot is an uncommon complication of diabetes mellitus (DM). It is a destructive inflammatory process often leading to joint degeneration, deformity, and disability in neuropathic patients. 1 The result of CNO is ulceration and infection in areas of high pressure, as a consequence of the residual deformity, which increases the risk of amputation. 2 CNO is considered one of the most devastating consequences of DM and is included in the range of diabetic foot syndrome. 3
The loss of sensitivity characteristic of diabetic neuropathy plays a central role, but, in addition, the peripheral circulation must be able to produce vasodilation that increases local flow in the foot and triggers the process. 4
The incidence of Charcot foot in the population with diabetes is between 0.1–7.5%, but the frequency increases to 35% among patients with diabetic neuropathy. 5 It has been reported that the incidence of bilateral involvement is between 9% and 75% of cases. The amputation rate in patients with Charcot's foot is 9%. 6
Midfoot Charcot Neuro-osteoarthropathy is the most common anatomic location of deformity, according to the anatomical classification by Sanders and Frykberg, 7 with around a 60% incidence rate at the tarsometatarsal joint, resulting in the typical rocker-bottom foot deformity. 8 It has an apex in the midtarsal joint that can be observed in radiological studies that evolves into bony prominences in the plantar region in the medial or lateral area. 9 Studies have shown that this midfoot deformity has a high risk of ulceration, due to its high-pressure peaks at the vertex of convexity. 10 The International Working Group of the Diabetic Foot (IWGDF) has indicated that elevated plantar pressures are an independent risk factor for ulceration and should, therefore, be avoided to prevent diabetic foot ulcers (DFU). 11 When conservative treatment is insufficient, midfoot offloading exostectomy allows for obtaining a plantigrade foot, early closure of the lesion, and less recurrence, due to the removal of the prominent bone area. 12 This offloading surgery reduces pressure in the overloaded area. 13
Exostectomy on the plantar bony prominence in CNO have achieved healing rates of nearly 75% as curative surgeries and have the advantage of decreased periods of immobilization and no internal hardware fixation. 14 Although this technique is apparently effective, some patients develop recurrent ulcerations and unstable position of the foot. For this reason, it has been argued that reconstructive surgery would be more appropriate for some patients. 15
The primary aim of this review is to assess the effectiveness of exostectomy for the management of the CNO midfoot deformity. The secondary objective was to evaluate late complications associated with this type of surgery in patients with CNO midfoot deformity.
Material and Methods
This systematic review was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 16 and has been registered in PROSPERO (a prospective international register of systematic reviews; identification code CRD42024595879).
Literature Search
A systematic review of the literature was conducted by two reviewers (NH.F.O and M.L.M) using PubMed, Medline, and Cochrane for all studies on exostectomy for the management of the diabetic Charcot midfoot deformity from inception up to November 5, 2023. The words “Charcot foot,” “Charcot neuroarthropathy,” “midfoot Charcot,” “rocker bottom,” “exostectomy,” “offloading,” “prevention,” “surgery,” “osteomyelitis,” “limb salvage,” and “ostectomy” were used as a search terms. These keywords were combined using the Boolean operator “AND” forming the following search strategies: Charcot foot AND exostectomy AND offloading AND prevention AND surgery AND osteomyelitis AND limb salvage AND ostectomy; Charcot neuroarthropathy AND exostectomy AND offloading AND prevention AND surgery AND osteomyelitis AND limb salvage AND ostectomy; midfoot Charcot AND exostectomy AND offloading AND prevention AND surgery AND osteomyelitis AND limb salvage AND ostectomy; rocker bottom AND exostectomy AND offloading AND prevention AND surgery AND osteomyelitis AND limb salvage AND ostectomy.
Selection Requirements
Inclusion Criteria
Inclusion criteria included (a) all studies since there are reports in the databases used; (b) studies published in English; (c) studies with abstracts; and (d) articles with original research.
Exclusion Criteria
Exclusion criteria included (a) studies only using a conservative approach to CNO; (b) studies on the surgical approach to CNO in locations other than the foot; (c) studies on surgical treatments of CNO other than exostectomy; (d) articles on surgical treatment of CNO with exostectomy that do not specify quantifiable results in relation to the number of them in the midfoot; and (e) studies on surgical treatment of CNO with midfoot exostectomy that do not present results in terms of any of the data collected: treatment success, healing time, major amputations, minor amputations, death, infection, reinterventions and/or ulceration recurrence.
Literature Screening and Data Extraction
Following the deduplication of search results, potential articles were reviewed based on titles and abstracts. Articles were independently screened by two authors (N.H.F.-O. and M.L.-M.), and the results were compared. A third reviewer (J.L.L.-M.) resolved any disparity between the authors. According to the research questions, the general information of each article was arranged in a data chart, including first author, year, study design, objectives, sample, success, healing time, minor and major amputation, infection, death, revision surgery, reulceration, and non-healing participants. Direct and indirect approaches, column patterns and surgical indications were included in the second chart.
Quality Evaluation of Included Studies (Strobe Guidelines)
Three independent researchers analyzed the data collected from all articles. As the included articles were retrospective cohort studies, the quality evaluation was based on the standard STROBE guidelines to ensure a high-quality presentation of observational studies. 17 Raters assessed the adequacy of reported items using the STROBE guideline checklist, which provides a framework for completeness and transparency. The STROBE guidelines checklist has 22 items, including items 1 (title and abstract), 2 and 3 (introduction), 4–12 (methods), 13–17 (results), 18–21 (discussion), and 22 (funding and sponsorship). Two raters (NH.F.O and M.L.M) independently assessed each study using the STROBE guidelines, and a third rater (JL.L.M) was involved in achieving a consensus in case of disagreement.
Statistical Analyses
As a result of the heterogeneity of the included studies in research design, follow-up time, and outcome indicators, it would be difficult to conduct quantitative analysis; therefore, only qualitative analysis was conducted.
Results
Literature retrieval
A total of 2825 articles were recovered in the initial search. After eliminating duplicates and applying the inclusion criteria, the titles and abstracts of the remaining 28 articles were read. Once the exclusion criteria were applied, 12 articles were selected for full-text evaluation. Finally, 11 articles were included for analysis. Figure 1 shows the literature screening process.
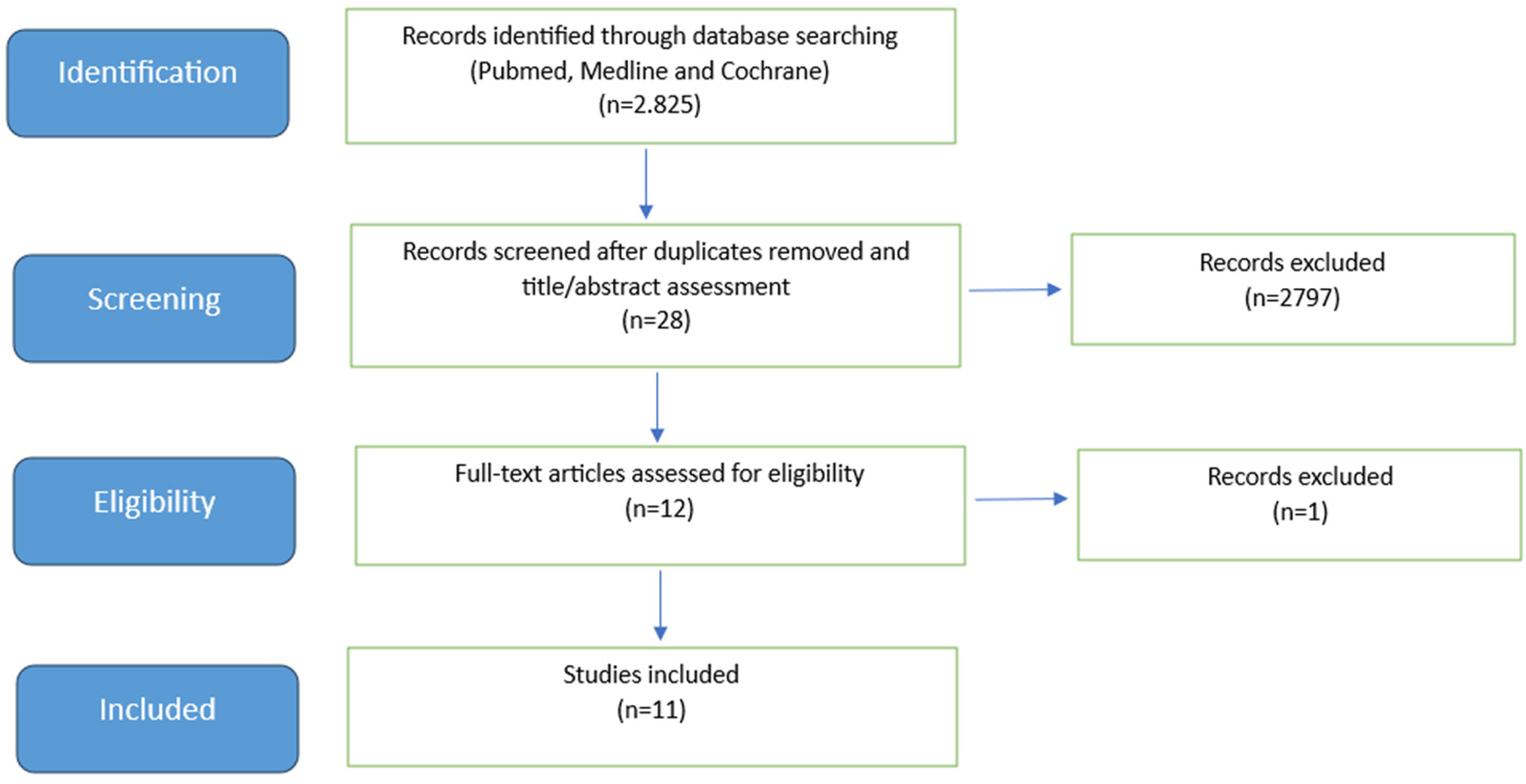
Flowchart of Identified Studies.
Characteristics of the Included Studies
The 11 studies included were case series (Level IV of evidence), all of which were retrospective. The articles included a total of 140 exostectomies performed in patients with diabetes.18–28
In the study conducted by Laurinaviciene et al, 21 a total of 19 patients and 20 feet were included; 18 had Charcot Neuro-osteoarthropathy secondary to diabetes, and in the case of the remaining patient, Charcot Neuro-osteoarthropathy was secondary to excessive alcohol consumption. The authors analyzed the results collectively, so it was not possible to evaluate them independently. Brodsky et al 27 included a total of 11 patients with a Type I midfoot anatomical pattern, according to their own classification, and one patient with a Type II hindfoot anatomical pattern. Similarly, the authors analyzed the results of both patterns together, and it was not possible to separate them for the presentation of results.
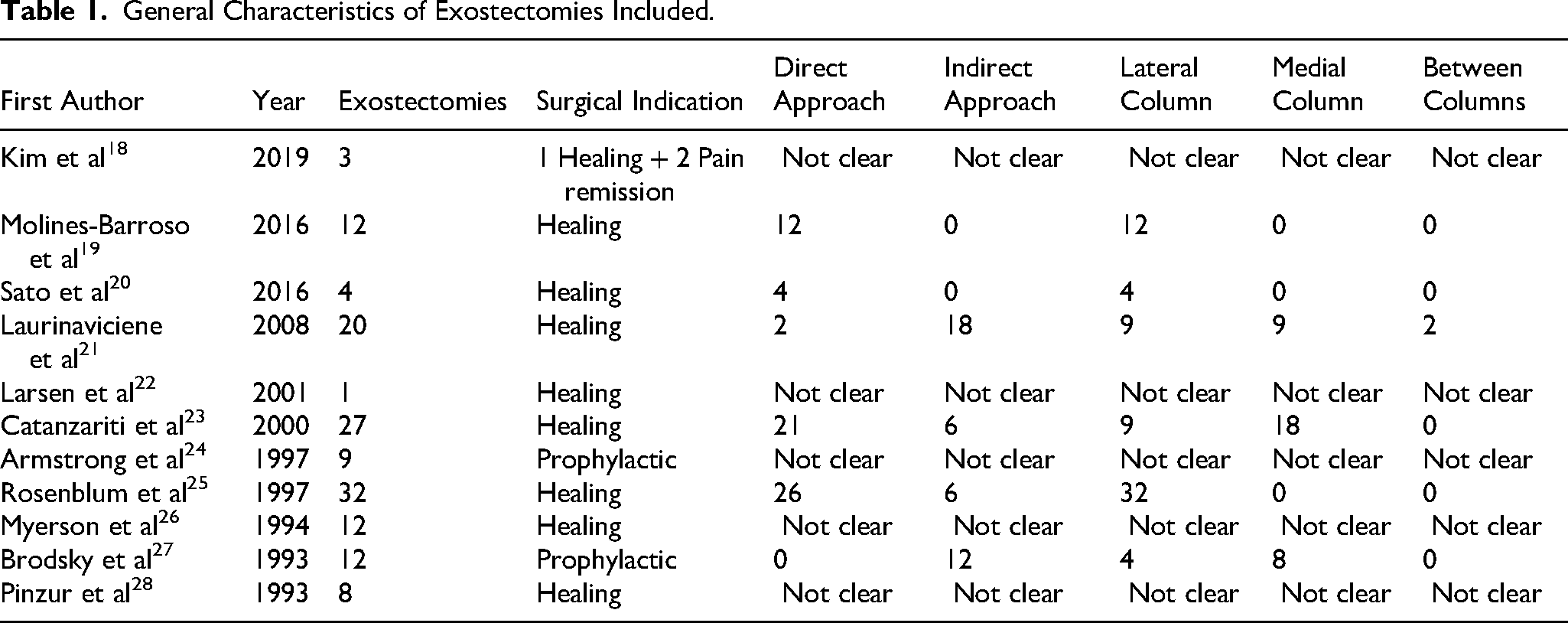
Among the total of 140 exostectomies, 123 had a curative indication. Fifteen exostectomies were performed with prophylactic indication. In only two exostectomies, the surgical indication was to resolve the pain associated with the bone prominence. 18
In all 140 exostectomies, a surgical resection of the midfoot bony prominence was performed. Sato et al 20 performed soft tissue reconstruction associated with the exostectomies using a medial plantar artery flap. Catanzariti et al 23 also used regional flaps to cover large defects in revision surgeries of the exostectomies, where the approach was direct. In cases where the ulcers were larger, Rosenblum et al 25 made a circular incision as part of the subsequent coverage using a regional flap. Myerson et al, 26 in cases where the midfoot deformity was associated with a fixed equinus position of the hindfoot, additionally performed an Achilles tendon lengthening.
The surgical approach was direct in at least 65 of the cases19–21,23,25 The approach to exostectomies was indirect in at least 42 of the cases.21,23,25,27
At least 70 of the exostectomies were under the lateral column19–21,23,25,27; 35 under the medial column21,23,27 and in 2 cases the location was defined as between the middle of both columns. 21 No data were obtained in the studies on the remaining 33 exostectomies (Table 1).
General Characteristics of Exostectomies Included.
Quality of the Reporting
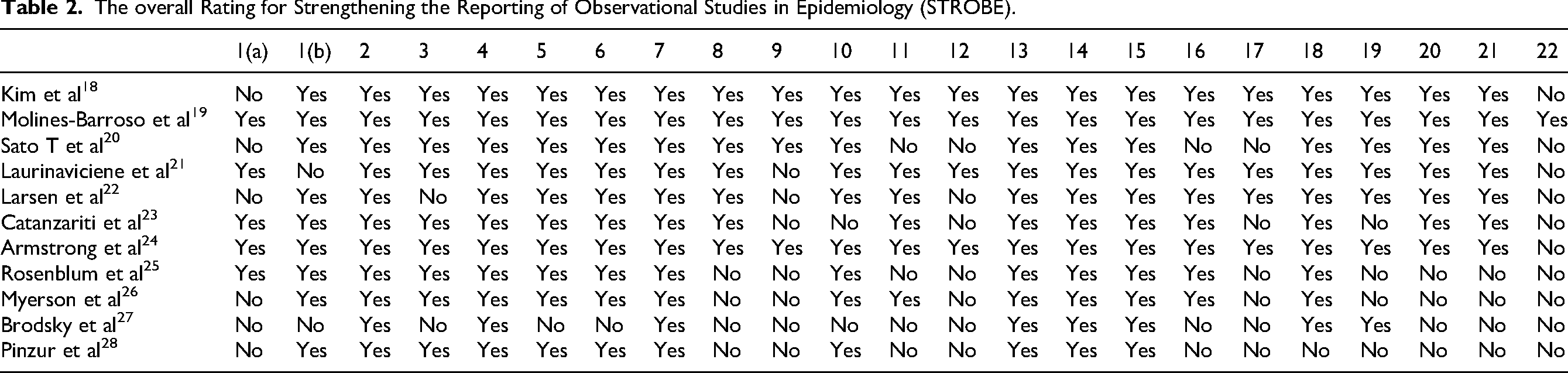
Items 9 (bias), 12 (statistical methods), and 22 (funding) were the most poorly completed in the studies. Table 2 shows the overall rating for the STROBE checklist. 17
The overall Rating for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Screened Outcomes
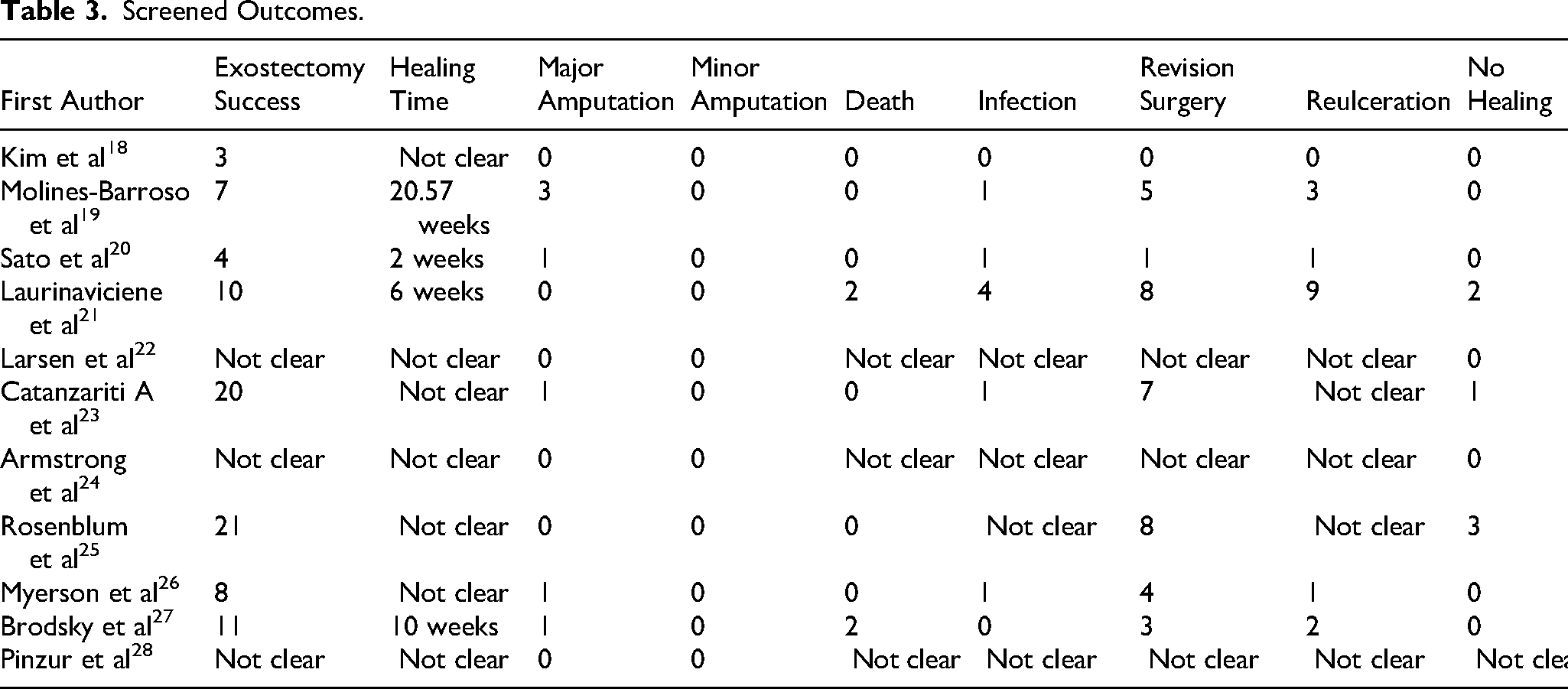
The results obtained concerning the exostectomy success, mean healing times, and adverse events and their relationship with the location of the exostectomy are shown in Tables 3 and 4.
Screened Outcomes.
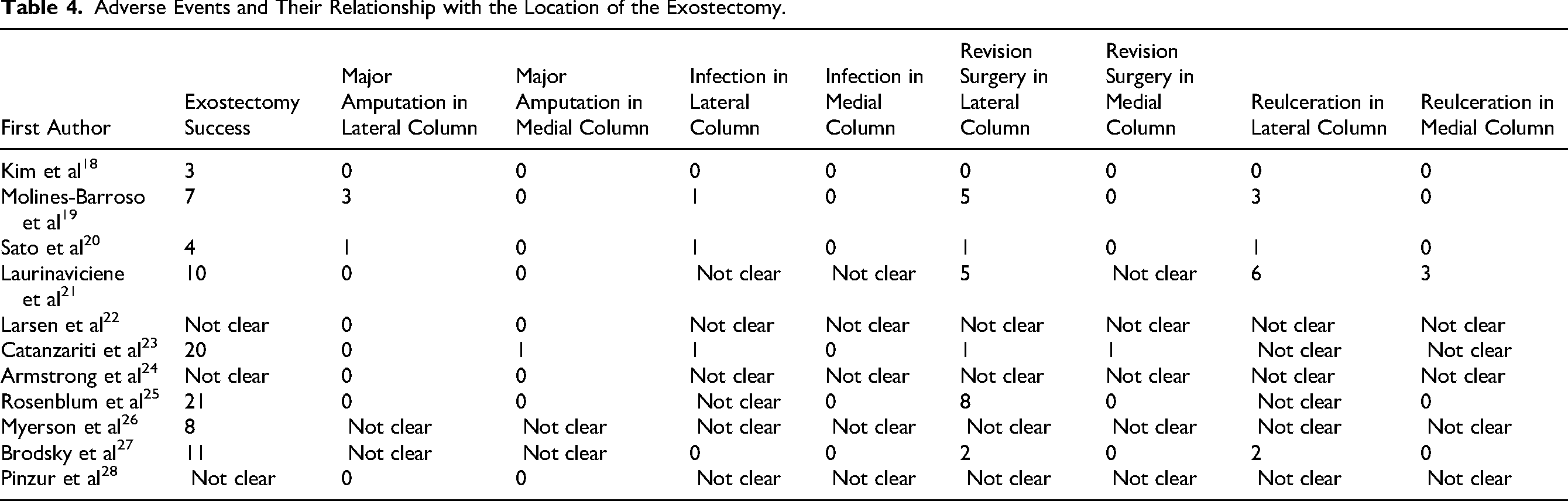
Adverse Events and Their Relationship with the Location of the Exostectomy.
Exostectomy Success
Of the 140 exostectomies, 84 were successful, understood as the closure of both the ulceration concomitant to the deformity and the incision in the case of an indirect approach and after a first procedure. Pinzur et al 28 do not clarify whether any of the eight exostectomies had complications during the follow-up period; they only mention that none led to an amputation. Armstrong et al 24 only mentioned that no amputations resulted as a result of CNO in their series. Larsen et al 22 stated that the procedure healed in a period of five months. The remainder had various complications that will be detailed later in the study.
Mean Healing Times
In the studies that presented data, the mean healing time was between 2 and 20.57 weeks after exostectomies.19–21,27 It should be noted that the shortest healing times were those of exostectomies associated with the medial plantar artery flap (two weeks). 20
Adverse Events
Amputation
As complications associated with the intervention, seven major amputations were observed after exostectomies. Four were related to the lateral column19,20; one to the medial column, 23 and, in the other two cases, the authors of the studies did not present data in this regard.26,27 The amputation in the study by Sato et al 20 was related to the patient's failure to comply with the post-surgical recommendations for use of the Charcot restraint orthotic walker (CROW) after the intervention. In the study by Molines-Barroso et al, 19 three patients suffered a major amputation, one due to a severe infection in the area of the intervention and the other two due to an unstable position of the foot for ambulation. Catanzariti et al 23 reported a below-knee amputation in a patient where the existence of chronic osteomyelitis and severe instability of the midfoot was confirmed after the intervention, and the patient did not want additional surgical procedures to save the limb. Myerson et al 26 reported that one exostectomy developed an infection three months after the procedure and required amputation, without specifying at what level. In the study by Brodsky et al, 27 a Syme amputation was performed on a patient with collapse and recurrent ulceration after exostectomy. The patient underwent subsequent revision surgery with unsatisfactory results. No minor amputation was reported in any of the studies evaluated.
Death
There were four deaths during the follow-up period, none apparently related to the exostectomies. Laurinaviciene et al 21 reported that one patient died of a myocardial infarction two months after the intervention without having completely healed and another died during the healing process of a second recurrence of the ulcer. However, the authors did not provide data on the reasons for this death. Brodsky et al 27 reported two deaths during the follow-up period; one from a patient eight months after intervention in a farm accident and another from a patient who died 33 months after a myocardial infarction. Both had healed before their deaths.
Infection
Of the 140 exostectomies, eight resulted in infection and in three cases amputation was required,19,20,26 Laurinaviciene et al 21 reported superficial wound infections involving soft tissue in three feet with edema, erythema, and increased temperature. Subsequently, the sutures were removed for drainage, closing the wounds by secondary intention. Another patient developed an infection with skin necrosis and osteomyelitis in the exostectomy cavity in which three additional surgical procedures were necessary to remove infected tissues and allow healing that took place three months after the follow-up period established in the study. Catanzariti et al 23 reported a case of a patient with an exostectomy under the lateral column who developed a severe infection after the intervention that required extensive debridement and a skin graft from another area to save the limb. Rosenblum et al 25 had serious complications in 11 cases that included deep wound dehiscence (with and without infection) and ulcer recurrences, without specifying how many of the complications there were.
Reinterventions
A total of 35 reinterventions were recorded in the 11 studies, including seven amputations. With the existing data on this subject, we can affirm that 25 of the reinterventions occurred in exostectomies under the lateral column.
Reulceration
Reulceration after exostectomy was mentioned 16 times. One ended in amputation 20 and three others were resolved with conservative treatment. 19 One reulceration required a subsequent arthrodesis for complete closure. 26 Brodsky et al 27 reported two reulcerations in the same patient who finally underwent a Syme amputation. Laurinaviciene et al 21 detailed nine reulcerations, five of which required a re-exostectomy for closure; in another three cases they closed using conservative treatment and one died before healing completely. There were studies that did not provide quantifiable data in this regard.18,22–25,28 With the data available from the studies, it is known that at least 12 reulcerations occurred under the lateral column and 3 under the medial column.
In only six cases the ulceration did not close after exostectomy during the follow-up period.21,23,25
Radiological changes in the alignment measurements
Regarding changes in the alignment of radiological measurements after exostectomy, the 12 lateral exostectomies in Molines-Barroso et al's 19 study, showed a decrease in the inclination of the calcaneus and an increase in the angle of declination of the talus. Changes in calcaneal inclination were greater for those patients who required revision surgery after exostectomy.
Discussion
The literature reviewed presents favorable data regarding the efficacy of plantar exostectomies in reducing the bony prominence of CNO in the midfoot and allowing ulcer healing as a prophylactic method. Of 140 exostectomies, 84 were successful at the first intervention. Likewise, 117 were effective after second interventions, both conservative and surgical, and 127 in total since ten exostectomies did not specify if they had to perform second interventions.
The results presented in this review show that exostectomies performed under the lateral column had a higher number of postoperative complications compared to those performed under the medial column, based on studies that provided data according to the location variable.19–21,23,25 This is consistent with previous reviews on the subject. Among the complications secondary to exostectomy, the most numerous were the need for reintervention and reulcerations. In the revision surgeries, from the total of 35 in the 11 studies, at least 25 occurred after the procedure under the lateral column. Of the 16 occasions in which reulceration was mentioned, we can affirm that at least ten procedures were under the lateral column. These results are similar to those of previous studies. Molines-Barroso et al 19 indicated that the first observed changes in the decrease of calcaneal inclination and the increase of talar declination showed a tendency toward progressive hindfoot collapse in patients with midfoot CNO who had undergone a midfoot exostectomy under the lateral column. Additionally, they found that plantar exostectomy in the lateral column showed a high probability (41.7%) of adverse events. Catanzariti et al 23 used Fisher's exact test for data analysis and found a statistically significant difference in the complication rate based on the ulcer location (p = 0.00174), with a higher rate in the lateral location compared to the medial location.
Based on the evidence collected during their review, Najefi et al 29 even developed an algorithm to guide decision-making regarding exostectomies in midfoot CNO. In this algorithm, two approaches were distinguished depending on whether the deformity and ulceration of the CNO of the midfoot, without infection and with good perfusion and stability, were located under the medial column, in which case they recommended an ulcerectomy and exostectomy. If the source of the problem was located under the lateral column, they recommended performing these procedures with greater caution and with radiological monitoring of the stability of the foot and the deformity.
One limitation of this review is the level of evidence of the articles included, which were exclusively retrospective studies of case series. Charcot foot is a rare condition, and although there has been an increase in the number and quality of publications on the subject in recent years, they are few in comparison to other clinical studies. 29 In a systematic review conducted by Schneekloth et al, 6 they stated that although the midfoot is the most commonly reported site for CNO in the various anatomical classifications, the highest number of surgical procedures for the treatment of CNO in the last five years was in the hindfoot. Additionally, they stated that the data from the review suggest that arthrodesis, specifically tibiotalocalcaneal fusion (TTC), appears to be more popular as a surgical treatment option for CNO. In addition to the selected articles, only a limited number of studies that include exostectomies in the treatment of midfoot CNO are available. Pinzur et al 30 reported having performed 18 midfoot exostectomies associated with CNO but did not provide specific data on the results and complications of the procedures. Although case series have less evidence, they are the most commonly published studies in surgical lietarture, since they contribute to scientific literature by describing unusual presentations of a common disease, novel interventions, rare diseases, and unexpected results of an intervention. 31
After the failure of conservative treatment, simple exostectomy may be effective in early treatment of low plantar ulcers and bony prominences associated with midfoot CNO and thus prevent catastrophic progression of the plantar lesion.
In the event that an exostectomy under the lateral column is indicated, it is recommended to perform the procedure with greater caution and with radiological monitoring of the stability of the foot and the deformity since these seem to have a greater number of complications.
In the case of a midfoot deformity secondary to CNO in an unstable midfoot, other surgical procedures are recommended to remove the bony prominence, allow for a stable and functional foot.
Conclusions
Exostectomies for the treatment of CNO in the midfoot have been shown to be safe when performed under the medial column. However, under the lateral column they worsen the alignment of the deformity in the sagittal plane and seem to develop a greater number of complications, such as reulcerations, the need for revision surgeries, and even amputation.
Footnotes
ORCID iDs
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.