
Abstract
Determining the optimal amputation level in diabetic foot (DF) and peripheral artery disease (PAD) patients is crucial for minimizing reamputation risk while preserving functionality. The Society for Vascular Surgery Wound, Ischemia, and Foot Infection (SVS WIfI) and International Working Group on Diabetic Foot (IWGDF) scoring systems are widely used for risk stratification, but their predictive value for reamputation remains unclear. The current study aimed to evaluate the predictive utility of these scoring systems for reamputation risk in patients undergoing amputations due to DF or PAD. A retrospective cohort study was conducted on 108 patients who underwent unilateral amputations due to DF or PAD between 2016 and 2021. Patients were categorized based on WIfI and IWGDF classifications, and clinical outcomes, including reamputation rates, ICU admissions, and mortality, were analyzed using logistic regression and post hoc analyses. Reamputation occurred in 41 (38%) patients. Higher WIfI (OR: 3.85, 95% CI: 2.10-7.05, P = .001) and severe IWGDF scores (OR: 3.25, 95% CI: 1.80-5.88, P = .008) significantly correlated with increased reamputation risk. Patients with high-risk scores also exhibited higher ICU admission (P = .03) and mortality rates (P = .01). Male gender (OR: 3.47, 95% CI: 1.45-8.31, P = .005), diabetes (OR: 2.32, 95% CI: 1.10-4.90, P = .027), and prolonged hospitalization (OR: 1.04, 95% CI: 1.01-1.08, P = .021) were independent predictors, while above-ankle amputations were protective for reamputation (OR: 0.22, 95% CI: 0.11-0.43, P < .001). Both scoring systems are effective in predicting reamputation risk, with WIfI providing a more comprehensive risk assessment. Combining these tools may enhance decision-making and improve patient outcomes in terms of reamputation prevention, hospital stay, ICU admission, and mortality.
Introduction
Determining an appropriate level of amputation for patients with diabetic foot (DF) and peripheral arterial disease (PAD) is a difficult and extensive clinical decision. Clinicians must evaluate the advantages of preserving limb length for mobility against the potential risks of postoperative complications during this procedure. To improve a patient's quality of life and functionality, procedures like transmetatarsal (TM) amputation are commonly performed. However, these distal approaches often pose challenges, such as difficult wound healing and the need for additional amputations, particularly in cases involving infections or advanced vascular conditions.1,2 However, proximal amputations such as transtibial (TT) and transfemoral (TF) are known to be associated with lower reamputation rates. Despite these advantages, these operations involve a greater risk of surgical trauma and mortality. Such issues indicate an urgent need for reliable prediction tools to help healthcare providers make wise and personalised decisions.3,4
Previous research indicates that the Society for Vascular Surgery Wound, Ischaemia, and Foot Infection (SVS WIfI) grading system has been little utilised to forecast the likelihood of reamputation. Although this system has been used to assess the likelihood of amputation in patients with DF infection,5–7 extensive research has not been conducted specifically on the likelihood of reamputation. 8 Similarly, the International Working Group on Diabetic Foot (IWGDF) guidelines recommend the use of the WIfI classification to predict healing potential and risk of amputation in individuals with diabetes, PAD and foot ulcer or gangrene. 9 However, studies linking IWGDF classifications directly to reamputation outcomes are very limited. 10
Given this gap in the literature, our study evaluates the relationship between SVS WIfI and IWGDF classifications and critical clinical outcomes such as reamputation rates and survival. Using these scoring systems, we aim to address an important gap in the literature by investigating their utility in predicting underreported reamputation outcomes. Utilising a retrospective cohort design, we hypothesise that higher SVS WIfI and IWGDF classifications are associated with increased reamputation risks.
Methods
Study Design
Patients who underwent amputation for DF and PAD in our clinic between 2016 and 2022 were retrospectively analysed (Approval Number: 2021/176). This study was conducted in accordance with the ethical rules regarding human experimentation as stated in the Declaration of Helsinki.
Study Population
The current study included individuals who had undergone their first unilateral below ankle (finger, Ray, TM, Lisfranc, Chopart, or Syme) and above ankle (TT and TF) amputation due to DF and/or PAD, and had lived for at least one year between January 1, 2016, and December 31, 2021. The participants were all over the age of 40. 11 Patients who were monitored for a minimum of one year following amputation were included. Exclusion criteria involved patients with bone tumors, Buerger's disease, hereditary and upper-limb amputation, autoamputation caused by diabetes, or those who had balloon angioplasty performed after the first amputation. 12 Additionally, amputations performed at the joint level and individuals who had previously undergone lower limb amputation for any reason were excluded.
Baseline Variables
The patients were divided into two groups: those who had not undergone reamputation and those who had. All patients were evaluated for age, gender, side, follow-up time, surgery time, hospitalisation time, and preoperative and postoperative blood values. A comparison was made between two groups, one with reamputation and one without reamputation, in terms of intensive care unit (ICU) admission, demographic data, blood transfusion, exitus rates, ASA score, and whether the cause was DF or PAD.
Scoring Systems and Risk Stratification
All SVS WIfI and IWGDF scores were independently assigned by AB, one of the study authors with over five years of clinical experience in managing DF and PAD. The scoring process was conducted based on patient history, clinical examination findings, laboratory results, and imaging studies, including radiographs and Duplex ultrasound. Each score was determined following the official guidelines of the SVS WIfI classification and the IWGDF scoring system. All scoring data were recorded in the patient's electronic medical records. Since the scoring was performed by a single experienced clinician, inter-rater reliability assessment was not applicable. This approach ensured consistency in patient classification and minimized variability. The SVS WIfI classification system offers a comprehensive assessment by combining wound, ischaemia and infection factors. This grading is clinically adapted to four different limb stages (1 to 4), and each stage correlates with the probability of wound healing and one-year risk of amputation. 13 SVS WIfI scores were calculated based on clinical and diagnostic data such as wound size, perfusion assessments (eg ankle-brachial index or finger pressure measurements) and signs of infection.
The IWGDF also uses infection severity grades and the presence of osteomyelitis as part of its risk assessment system. Grade 1 indicates no infection and Grade 4 indicates severe infection; subcategories for osteomyelitis include 3O for moderate infection and 4O for severe infection. 14 Adapted to the unique clinical circumstances of individuals with diabetic foot complications, these nuanced scales provide a thorough method for predicting healing results and amputation risks.
Definition of Amputation and re-Amputation
After considering all of the options, a multidisciplinary team decided on amputation and the appropriate level to do it. This group's speciality included plastic surgeons, orthopaedic surgeons, endocrinologists, infectious disease specialists, and cardiovascular surgeons. The decision for amputation was based on Duplex ultrasound findings, which evaluated distal perfusion and vascular flow characteristics. Revascularization was considered before amputation if Duplex ultrasound findings indicated salvageable limb perfusion, and there was no severe infection requiring immediate surgical intervention. If revascularization was not successful or contraindicated, amputation was prioritized. When a patient had a localised infection, manageable ischaemia according to Duplex ultrasound results (eg, sufficient distal flow signals), and no deep tissue involvement or significant necrosis, below-ankle amputations were considered. When CT angiography indicated significant ischaemia, when infection reached deeper structures, or when localised amputation did not seem to manage the infection or heal well, above-ankle amputations were performed.
Our concept of a “reamputation” included any further operation on the amputated limb. This included soft tissue revisions, which addressed inadequate wound healing, infection, or necrosis at the same amputation level, bone shortening procedures performed to optimize soft tissue coverage and reduce tension (especially in cases of exposed or infected bone), and higher-level amputations when infection, ischemia, or wound progression rendered the initial level insufficient. 15 While following the standardised criteria set out by the interdisciplinary workgroup, reamputation decisions in this study were customised to each patient's presentation. Wound revisions or bone shortening treatments at the same level were usually the extent of reamputation for patients presenting with localised infections of soft tissues or necrosis. Prolonged drainage from wounds, worsening tissue necrosis, or exposed bone without sufficient covering of soft tissues were some of the clinical findings that influenced these judgements. Whenever localised treatments proved inadequate due to persistent ischaemia or infection, the reamputation was advanced to a higher level, such as from TM to TT amputation. Insufficient perfusion was frequently confirmed and decision-making was aided by CT angiography in these cases. Further, when local wound control failed in patients with systemic infection or sepsis, reamputation to a higher level was prioritised as a means of infection management and ensuring survival. Systemic indicators, such as increased C-reactive protein (CRP) or white blood cell counts, also played a role in these determinations.
Postoperative Protocols
Wound care, early mobilization, and personalized rehabilitation regimens were part of the postoperative treatment plans. Antibiotic regimens were planned based on wound cultures. Patients with PAD were given anticoagulants or antiplatelet drugs to prevent thromboembolic events, and negative pressure wound therapy (NPWT) was applied to high-risk wounds The administration of blood transfusions was based on haemoglobin levels and the patient's cardiovascular stability both during and after operation.
Imaging and Preoperative Assessment
The severity of ischemia and limb perfusion were assessed preoperatively using vascular tests such as CT angiography or Doppler ultrasound. Integration of imaging findings with clinical assessments enabled precise surgical planning and risk stratification based on the SVS WIfI and IWGDF frameworks.
Statistics
Statistical analyses were conducted utilising SPSS version 26.0 (IBM Corp., Armonk, NY, USA). The median (interquartile range) or mean ± standard deviation were used to express continuous variables after the Shapiro-Wilk test was used to check the normality of the data distribution. The frequency and percentage values were used to represent the categorical variables. The independent sample t-test or Mann-Whitney U test was employed for continuous variables, while the chi-square test or Fisher's exact test was utilised for categorical variables for comparisons between reamputation and non-reamputation cohorts. To identify the parameters that may be used for reamputation prediction, binary logistic regression analysis was carried out. Odds ratios (OR) have been determined with a 95% confidence interval (CI) to evaluate the strength of the relationships. The Hosmer-Lemeshow test was utilised to evaluate the adequacy of the logistic regression model. Post-hoc analyses were conducted for pairwise comparisons utilising Bonferroni correction to address multiple testing. In all analyses, P < .05 was accepted as the statistical significance limit.
Results
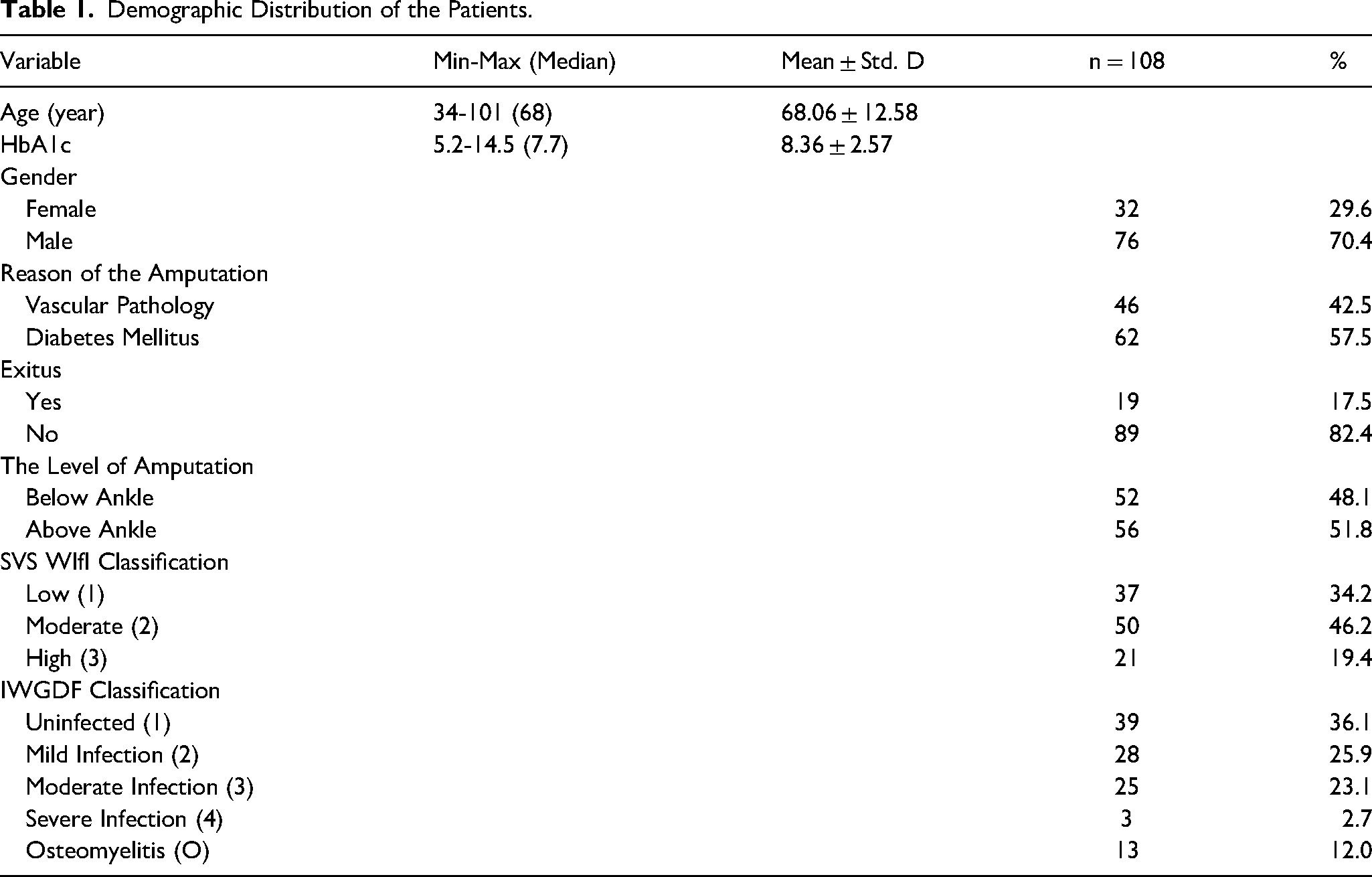
Initially, 132 patients were identified. Nevertheless, 24 individuals were omitted, comprising 8 who had previously had lower-limb amputation, 6 who received concurrent balloon angioplasty following the first amputation, 4 who underwent upper-limb amputation, and 6 patients without complete follow-up data. In this retrospective analysis, 108 patients fulfilled the aforementioned criteria. A total of 67 people who underwent amputations solely were classified as the first group, whereas 41 people who underwent reamputations were classified as the second group. The demographic data of the patient population is shown in Table 1, while various factors and biochemical parameters are examined in Table 2 according to whether the patients had reamputation or not. A significant difference was seen in the length of hospital stays between individuals who required reamputation and those who did not (mean difference: 7.75 days, P = .043, P < .05). The statistical analysis showed that the gender distribution of the reamputation group was significantly different from the non-reamputation group. (Male: 85.3% vs 61.1%, mean difference: 24.2%, P = .011, P < .05). Other biochemical indicators, however, did not show any statistically significant variations. (Table 2).
Demographic Distribution of the Patients.
Comparison of Patient Characteristics, Surgical Parameters, and Biochemical Markers Based on Reamputation Status.
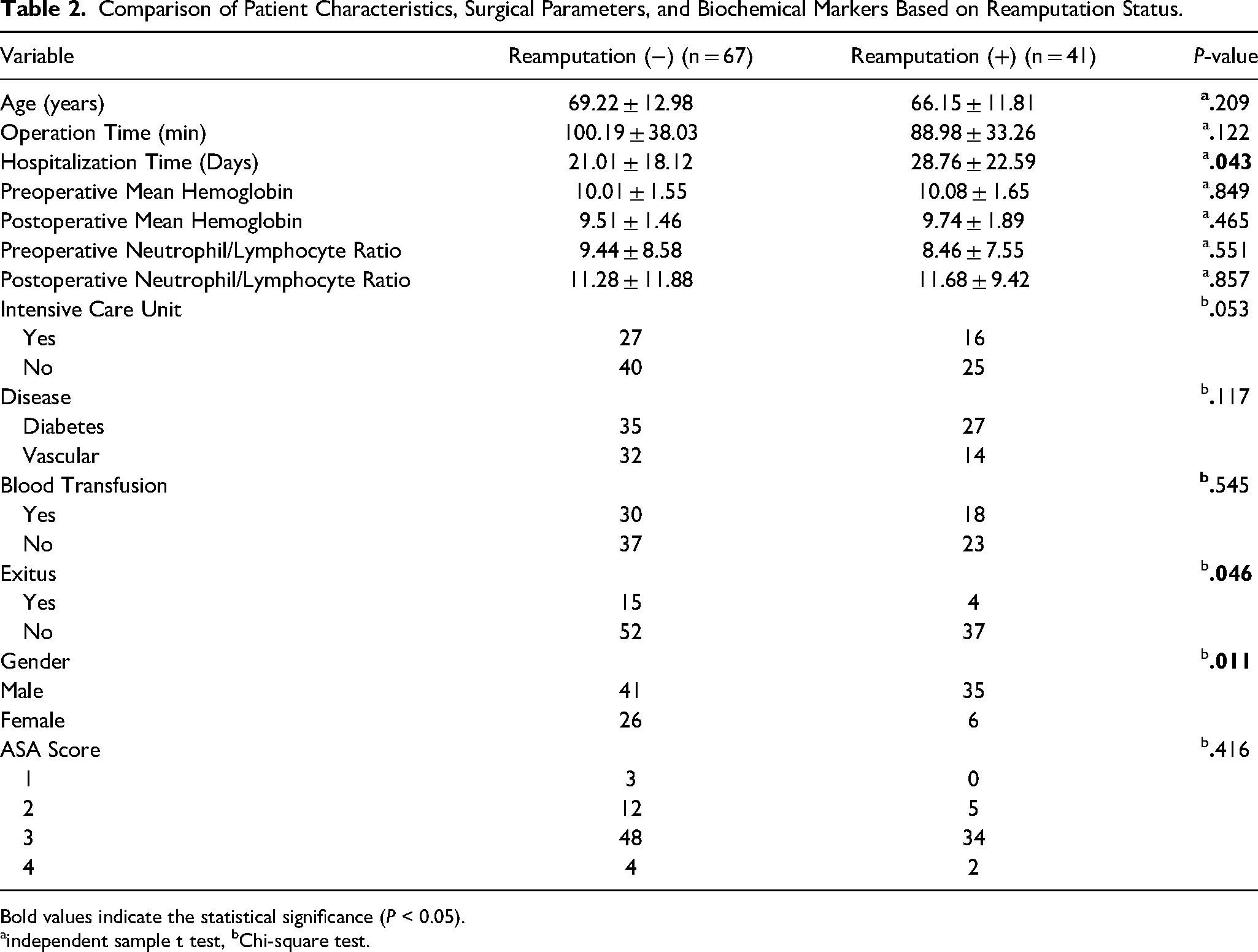
Bold values indicate the statistical significance (P < 0.05).
independent sample t test, bChi-square test.
Upon evaluating the existence of reamputation and particular indicators, it was shown that the mortality rate of individuals who did not undergo reamputation was much greater compared to those who did (Non-reamputation: 22.3% vs Reamputation: 9.7%, mean difference: 12.6%, P = .046, P < .05) (Table 2). No relationship has been identified between reamputation and criteria such as blood transfusion (P = .545), the patient's ASA score (P = .416), and admission to the ICU (P = .053, P > .05) (Table 2).
Table 3 and Figure 1 examine the rates of ICU admission, mortality (exitus), and reamputation based on the classifications of SVS WIfI and IWGDF. Patients in the highest-risk SVS WIfI category had significantly higher rates of ICU admission (61.9%) compared to the lowest-risk category (16.2%, P = .01). Mortality rates were also elevated in the highest SVS WIfI category (47.6%) compared to the lowest (2.7%, P = .01). Similarly, reamputation was more frequent in the highest-risk SVS WIfI group (52.4%) compared to the lowest-risk group (21.6%, P = .03). A similar trend was observed in the IWGDF classification. ICU admission was significantly higher in the severe osteomyelitis group (69.2%) compared to the no-infection group (17.9%, P = .03). Mortality rates were highest in the severe IWGDF cases (46.1%) compared to the lowest-risk group (0%, P = .01). Reamputation was also more frequent in severe IWGDF cases (53.8%) than in the lowest-risk category (10.2%, P = .01). These findings suggest that patients in high-risk categories require more aggressive management and close monitoring.
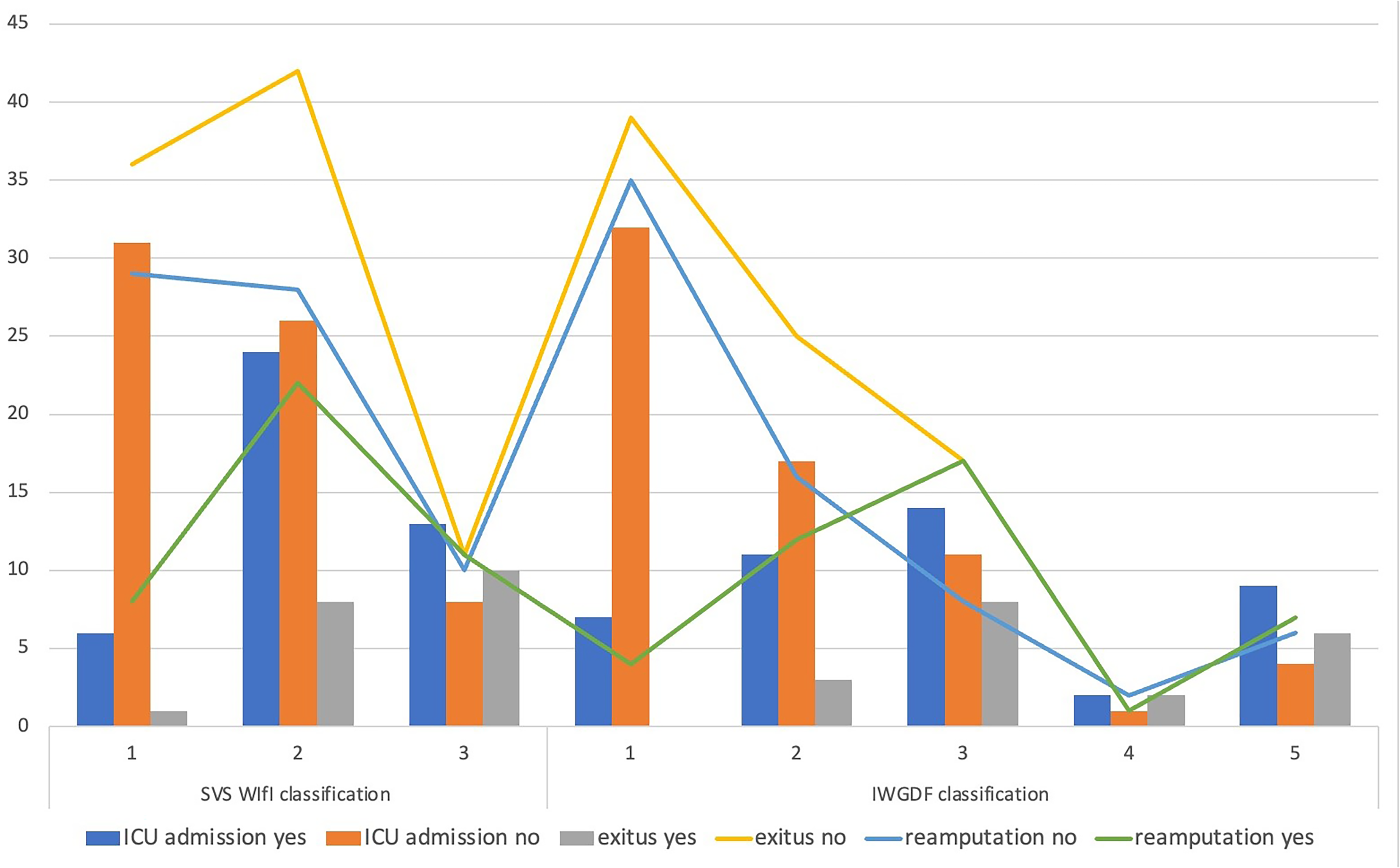
Distribution of ICU admission, mortality, and reamputation rates according to SVS WIfI and IWGDF classifications. The figure illustrates the increasing frequency of ICU admission, mortality, and reamputation rates with higher-risk SVS WIfI and IWGDF categories. Patients in the highest-risk groups exhibited the highest rates of adverse outcomes.
SVS WIfI and IWGDF Classifications and Their Association with Clinical Outcomes.
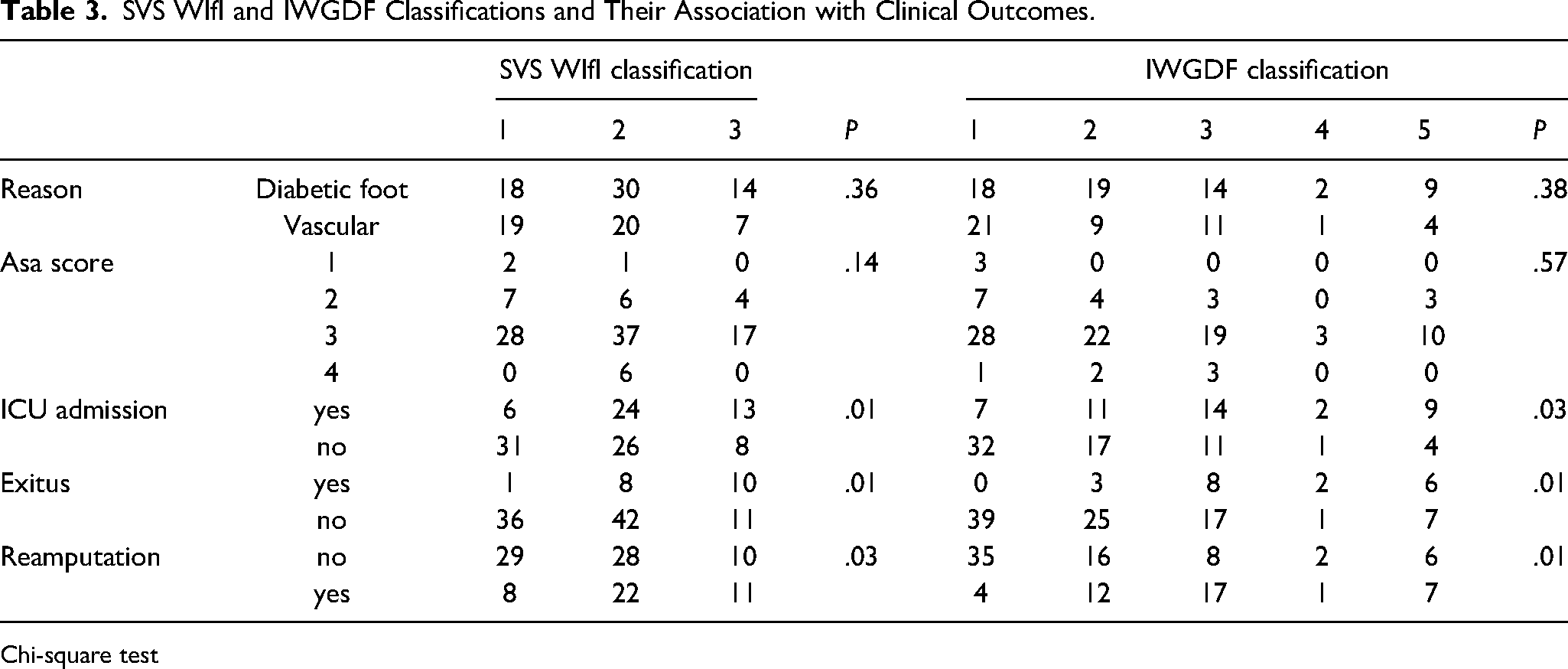
Chi-square test
Table 4 presents the results of post-hoc analyses comparing ICU requirement, mortality (exitus) and reamputation rates between different risk groups according to the IWGDF and SVS WIfI scoring systems. There are statistically significant variations in these outcomes between the low-risk and high-risk groups. Category 5 (severe osteomyelitis) and category 1 (no infection) of the IWGDF were substantially different in terms of the need for ICU (mean difference: 0.513, P = .008). Furthermore, there was a notable disparity between the low-risk category 2 and the high-risk category 4 of SVS WIfI (mean difference: 0.457, P = .001). Categories with higher IWGDF scores also had substantially higher mortality rates; category 5 was statistically different from category 1 (mean difference: 0.462, P = .001). Reamputation rates were observed to be considerably greater for IWGDF category 5 compared to category 1 (mean difference: 0.436, P = .025). The significance of targeted therapies in patients with high IWGDF and SVS WIfI scores is underscored by our findings, which emphasise the higher clinical burden in these populations.
Post-hoc Analysis of ICU Admission, Mortality, and Reamputation Rates Based on IWGDF and SVS WIfI Classifications.
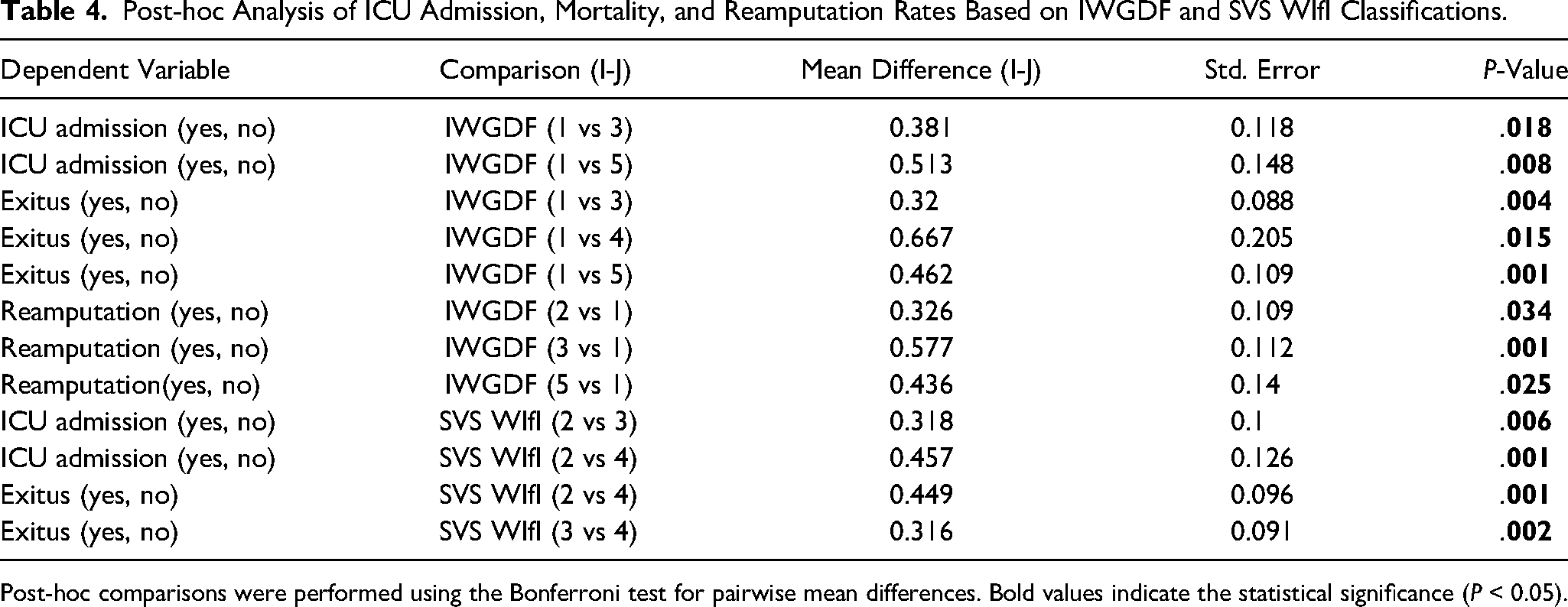
Post-hoc comparisons were performed using the Bonferroni test for pairwise mean differences. Bold values indicate the statistical significance (P < 0.05).
Table 5 presents the results of the binary logistic regression analysis identifying predictors of reamputation risk in patients with DF and PAD. The results showed that the likelihood of reamputation was much higher in males (OR: 3.47, 95% CI: 1.45-8.31, P = .005). Reamputation risk was also highly anticipated by DF (OR: 2.32, 95% CI: 1.10-4.90, P = .027). In addition, the likelihood of reamputation was considerably reduced in individuals who had above-ankle amputations (OR: 0.22, 95% CI: 0.11-0.43, P < .001). Reamputation was also more likely to occur in patients whose hospital stays were longer (OR: 1.04, 95% CI: 1.01-1.08, P = 0.021). There was a considerable association between high SVS WIfI scores (High vs Low) and an increased risk of reamputation (OR: 3.85, 95% CI: 2.10-7.05, P = .001). Similarly, reamputation risk was strongly predicted by severe IWGDF scores (Severe vs Mild) (OR: 3.25, 95% CI: 1.80-5.88, P = .008). This research proves that vascular problems and advanced infection are major factors that affect the frequency of reamputations.
Logistic Regression Analysis of Predictors Associated with Reamputation Risk in Patients with Diabetic Foot and Peripheral Artery Disease.
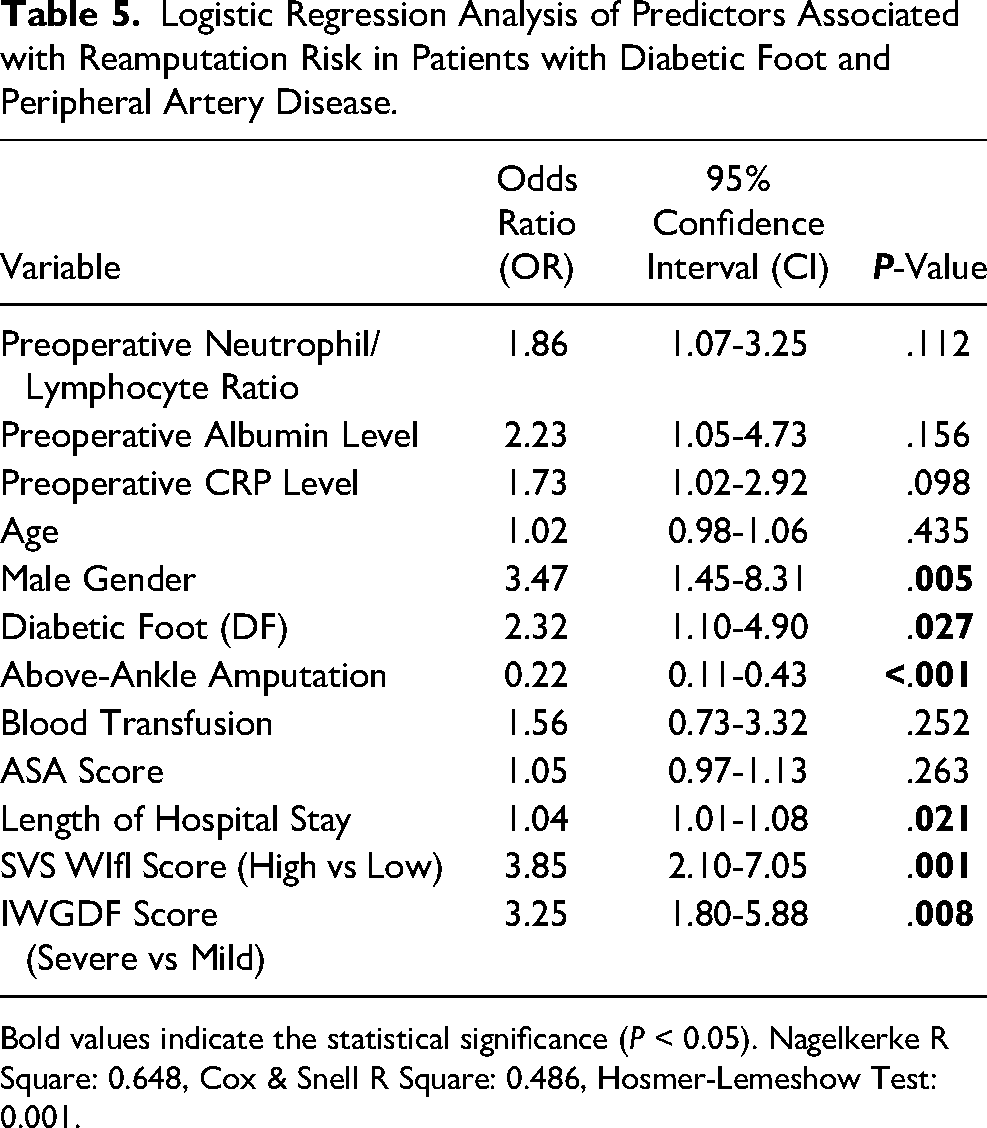
Bold values indicate the statistical significance (P < 0.05). Nagelkerke R Square: 0.648, Cox & Snell R Square: 0.486, Hosmer-Lemeshow Test: 0.001.
On the other hand, there was no statistically significant correlation seen for the following: preoperative albumin level (OR: 2.23, 95% CI: 1.05-4.73, P = .156), preoperative neutrophil/lymphocyte ratio (OR: 1.86, 95% CI: 1.07-3.25, P = .112), or preoperative CRP (OR: 1.73, 95% CI: 1.02-2.92, P = .098). Neither blood transfusion nor ASA score was associated with an increased risk of reamputation (OR: 1.56, 95% CI: 0.73-3.32, P = .252 and OR:1.05, 95% CI: 0.97-1.13, P = .263) respectively. Lastly, the odds ratio (OR) for reamputation was 1.02 (OR: 1.02, 95% CI: 0.98-1.06, P = .435), which did not indicate a statistically significant link between age and reamputation risk.
Discussion
In patients with DF and PAD, this study presents a thorough assessment of reamputation risk variables and emphasises the predictive value of the SVS WIfI and IWGDF scoring systems. Increases in reamputation rates, ICU hospitalisations, and death were shown to be highly linked with higher SVS WIfI and IWGDF scores, adding considerably to the current body of knowledge. To highlight, reamputation was found to be independently predicted by being male, having diabetes, and a length of time spent in the hospital, whereas above-ankle amputations protected against reamputation. In order to improve surgical outcomes and provide targeted therapies to high-risk individuals, our findings highlight the need of incorporating sophisticated risk classification methods into clinical decision-making.
The majority of amputees were male (70.4%) with an average age of 68.06 ± 12.58 years. The significant disparity between genders cannot be attributed to the variation in the occurrence of diabetes (9.12% in men, 13.1% in women), 16 or the prevalence of PAD, which, although more prevalent in younger men, has comparable rates in older men and women. 17 Nonetheless, research has demonstrated that men are more susceptible to foot ulcers and, as a result, have a higher risk of lower extremity amputation. This is due to the more severe neuropathy and increased joint stiffness experienced by men. 18
Some studies published in the literature show a clear independent connection between the WIfI grade and risk of major amputation. Research exists on the correlation between wound healing duration and WIFI score; however, no research have investigated the association between WIFI grading and reamputation. To our knowledge, this study is among the first to establish a direct correlation between WIfI scores and reamputation risk, expanding the current understanding of the WIfI system's clinical applicability.
Ward et al 19 observed that a rising WIfI score correlated with an 84% higher likelihood of major amputation one year post-risk adjustment. Robinson et al 20 reported that WIfI stage 4 wounds were linked to a 12-fold increase in the risk of major amputation within one year following risk adjustment. Darling et al 21 prospectively reported that the WIfI classification system may stratify a patient's amputation risk at presentation as well as during therapy, so assisting clinicians in determining the aggressiveness of limb preservation efforts. However, reamputation was not evaluated in any of these studies. In the current study, high SVS WIfI scores (High vs Low) were strongly associated with an increased reamputation risk (OR: 3.85, 95% CI: 2.10-7.05, P = .001). This may be supported by publications in the literature showing the relationship between wound healing and the WIFI scoring system. Hicks et al 22 demonstrated that an increase in WIfI stage independently predicted poor wound healing following risk adjustment. The existence of an advanced-stage wound (WIfI stage 3 and 4) emerged as the most significant predictor of poor wound healing, surpassing factors such as wound size, PAD, and other patient-related risk factors. Initial evaluations of the WIfI classification system by Cull et al 23 and Zhan et al 24 established that the SVS WIfI classification technique corresponds with significant clinical results for limb salvage and wound healing. Conversely, Vartanian et al 25 indicated that the probability of wound healing was not substantially influenced by WIfI degree (stage 4: odds ratio, 0.97; 95% CI, 0.34-2.81). Only the location of the wound was independently correlated with the healing process. In the current study, since the revision of the amputation stump and any kind of wound revision is considered as reamputation, any study in the literature that examines the link between wound healing and WIFI score is of interest to the current study. One of the limitations of our study is that the patients who underwent reamputation were not analysed in subgroups (going to the next level of amputation, or wound site revision, etc) due to the small number of patients.
As per the IWGDF/IDSA guidelines of 2023, 14 it was indicated that, based on the evaluation of the wound and the extent of tissue loss, the outcomes of non-invasive tests, and the IWGDF/IDSA infection severity score, all patients should be categorised according to the WIfI classification system, which aids in further assessing the necessity for a vascular intervention as outlined in the IWGDF PAD guidelines. The incorporation of WIfI scoring into the IWGDF framework not only aids in determining vascular interventions but also highlights its importance in predicting patient outcomes, such as wound healing and amputation risk, in diabetic foot management. Moreover, prior research indicates that when the levels of IWGDF infection severity increase, the likelihood of amputation rises.26–28 In our study, severe IWGDF infection scores were also independently associated with reamputation risk, further underscoring the predictive value of this classification system in DF management. Although the prognostic capability of the IWGDF system has been questioned due to its lower predictive accuracy compared to other tools (eg, ROC: 0.67 for IWGDF vs 0.80 for Eurodiale Risk Score), 28 we advocate for the combined use of IWGDF and WIfI scores to better guide reamputation decisions and ensure a more comprehensive risk assessment. The combination of WIfI and IWGDF scoring systems offers a more comprehensive risk assessment by integrating ischemia, wound characteristics, and infection severity. However, implementing these systems together may be time-consuming and requires standardization and clinical integration. Incorporating them into electronic health records could streamline the process, and future studies should evaluate the effectiveness of this approach.
Reamputations after a major initial lower extremity amputation are often occurring on the opposite side and are linked to PAD. 29 Glaser et al 30 concluded that chronic renal insufficiency, PAD, and prior major amputation were the leading predictors of contralateral reamputation, although diabetes mellitus was not statistically significant. The inclusion criteria for the current study excluded reamputation to the contralateral side. However, revision to the same side was regarded as reamputation. The study by Seçkin et al 12 identifies several risk factors for reamputation, including albumin value, smoking, hypertension, duration of diabetes, number of debridements following surgery, and prolonged hospitalisation. Acar et al 31 identified male gender and prolonged diabetes duration as the most significant predictors for the necessity of reamputation, consistent with the findings of the current study. Ohsawa et al 32 identified female gender and older age as important indicators of risk for reamputation. Tukenmez et al 33 discovered hypertension, coronary artery disease, and leukocytosis to be the predominant nondiabetic-related risk factors for reamputation. Conversely, our findings indicate that older age and leukocytosis were not independent predictors of reamputation. The likelihood of reamputation in our sample was higher for males compared to females. Font-Jiménez et al 34 indicate that, regarding the level of resection, patients with diabetes most frequently experience minor and ipsilateral reamputations. As in line with the literature, analysis of the cases accepted for reamputation in the current study revealed that the majority of patients were diabetic and did not belong to the PAD group. Most patients underwent below-ankle amputation, with either modifications to the wound site or progression to the next level of amputation.
Our findings highlight the importance of combining SVS WIfI and IWGDF scoring systems for risk assessment in DF and PAD. SVS WIfI evaluates vascular status and wound healing potential, while IWGDF focuses on infection severity and osteomyelitis. This combined approach improves risk prediction and guides treatment strategies. Using both classifications enables early identification of high-risk patients, allowing prompt revascularization, intensive wound care, and infection control. High-risk patients in both systems had the highest rates of reamputation, ICU admission, and mortality, emphasizing the need for close monitoring and multidisciplinary intervention. These tools aid in prioritizing patients for limb salvage or early amputation. Clinicians should use SVS WIfI and IWGDF scores together for DF and PAD management. Patients with severe scores require urgent vascular assessment and infection control. A structured risk assessment based on these scores can guide wound care, antibiotic therapy, and surgical planning. However, applying these systems in low-resource settings can be challenging due to limited access to Duplex ultrasound, CT angiography, and trained specialists. Alternative risk assessment methods using clinical parameters and basic vascular tests may be needed. Future research should focus on adapting these scoring systems for broader accessibility.
Limitations
There are several limitations of the study that must be recognized. First, the retrospective design may cause selection bias and preclude from establishing causation between risk factors and reamputation. Second, the limited cohort size precluded subgroup analyses, including differentiating stump revisions from high-level amputations. Further stratification based on reamputation timing (early vs late), anatomical level (below-ankle vs above-ankle), and the underlying indication for reamputation (infection progression vs ischemic failure) could provide deeper insights into patient outcomes. The lack of subgroup analysis may have obscured potential variations in prognosis and treatment response between different reamputation scenarios. However, given our sample size constraints, such subgroup analyses were not feasible in this study. Future research should consider a more granular approach to reamputation classification, which could help refine predictive models and improve individualized patient management. Understanding whether early versus late reamputation is influenced by distinct risk factors or whether certain surgical techniques are more effective in specific subgroups could further enhance clinical decision-making. Third, it was a single center study so the results and findings may not generalize to wider populations or health care settings. Fourth, although the research demonstrated the predictive utility of WIfI and IWGDF scoring systems, it neither makes a direct comparison of prognostic accuracies nor validates the synergistic use in clinical practice. Fifth, functional outcomes of reamputation, quality of life, and patient satisfaction in the long term were not assessed. Such information could, therefore, give a more composite picture of how varied grading systems affect the care of the patient. Last, while both Doppler ultrasonography and CT angiography were used for vascular assessments, these imaging modalities were not uniformly applied among all patients in our trail, potentially leading to heterogeneity in how ischemia severity was assessed. Indeed, Doppler ultrasonography was used more often because it is readily available, while CT angiography was reserved for cases that warranted more sophisticated vascular assessments, increasing the risk of variability in the decision process. Despite its shortcomings, this investigation addresses one of the few studies to relate two scoring systems, namely SVS WIfI and IWGDF, to reamputation risk in DF and PAD patients. The study thus adds value to the underappreciated area of the prognostic value of these scoring systems and their potential use jointly for clinical decision-making.
Conclusion
This study provides evidence that higher SVS WIfI and IWGDF grades are significantly associated with an increased risk of reamputation in patients with PAD and DF. These systems enable clinical decision-making and risk stratification: higher scores were directly associated with higher rates of reamputation, ICU admissions, and mortality. Although above-ankle amputation offered some protection against reamputation, reamputation was independently predicted by male sex, diabetes, and duration of stay. Despite its limitations, this study is among the few that consider the relationship between these scoring systems and the likelihood of reamputation, offering us valuable insights into their prognostic utility. Future studies should seek to validate the combined use of the WIfI and IWGDF scores in larger cohorts to further refine their clinical applicability and improve patient outcomes.
Footnotes
Authors’ Contribution
All the authors have approved the final contents of the submission and been actively involved in the planning and in the enactment of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Informed consent was obtained from the patients or legal guardians of all subjects. Ethical approval was obtained from the Bakırköy Dr Sadi Konuk Training and Research Hospital's ethics committee (approval number: 2021/176). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.