
Abstract
This investigator initiated prospective observational study investigates the prevalence of contact allergies in patients with a Diabetic Foot Ulcer (DFU). Patients with a DFU received a combined PATCH-test (a test used to investigate the origin of an allergic reaction on the skin) at the upper back, with the European baseline series, the European leg ulcer series, and local used material for leg ulcers. A total of 108 patients with DFU were included of which 86 (79.6%) were male, and 9 (8.3%) and 99 (91.7%) patients had Type 1 and Type 2 diabetes, respectively. Twenty-one patients had a sensitization in the standard series, 30 patients in the leg ulcer series, and 11 patients in both series. Two patients had a positive reaction for one of the local used materials. Most frequent sensitizations were found for Perubalsem (N = 6) and Fragrance-Mix II (N = 4) in the standard series. A sensitization for Povidone-Iodine (N = 20) was most frequently seen in the leg ulcer series. In the local used materials a sensitization for silver sulfadiazine (N = 1) and cutimed-gel (n = 1) were seen. In conclusion, this study provides novel information about sensitizations in patients with DFU, but more research is needed to demonstrate the relationship between allergic reactions and delayed wound healing. The study protocol was registered in www.clinicaltrials.gov (NCT04085705, PAID study).
Foot ulceration is often seen in people with diabetes. It is a common, complex and costly complication. The prevalence of a diabetic foot is 5.1% in Europe 1 and about 0.5% in the Netherlands. 2 There are several well known risk factors such as poor glycemic control, peripheral vascular disease, neuropathy, smoking, history of lower extremity amputation and anatomic foot deformity.
Once a foot ulcer has developed in patients with diabetes, delayed wound healing is a serious problem with an increased risk of amputation. Several conditions play an important role in this delay, such as infection with or without osteomyelitis, arterial and venous insufficiency, edema, elevated foot pressure due to improper footcare and ill-fitting footwear. There are additional factors that contribute to delayed healing such as microbiome and dysregulated immune functions, which are comparable with other chronic wounds, like venous leg ulcers (VLU).3,4
It is less known that contact allergies play a role in delayed wound healing.5,6 Various modern wound dressings are available for the treatment of complex healing wounds such as a diabetic foot ulcer (DFU). It is often assumed that modern wound dressings, because of their hypoallergenic or anti-allergic properties and their comfort to patients, seldom cause allergic reactions.
Sensitization to topical treatment for instance in VLU is still frequent, and moreover, continues to increase, even for new products.5,7–9 Long duration of ulcers, damage of the skin barrier and the use of topical medicaments with occlusive bandages are strong sensitizers and frequently lead to sensitization and contact allergy. Among patients with VLU contact allergies is seen in around 50% of which 10%–20% specific for wound dressings.1,10–12 The prevalence of contact allergies is rising and is also increasing with a longer duration of the ulcer.5,13 Little is known about the occurrence of sensitization and contact allergy in patients with DFU. Some studies with leg ulcer and contact allergies include diabetes, but still little is known about sensitization in patients with DFU.
The aim of this observational prospective study is to determine the prevalence of contact allergies in patients with DFU and to compare the outcome to the prevalence of contact allergies in patients with VLU in general.
Research Design and Methods
Study Design
The PAID study is an investigator initiated prospective observational study. Patients with a DFU were included in the Rijnstate hospital, the Netherlands, between September 2019 and December 2022.
Inclusion criteria were an age of ≥18 years, written informed consent, the presence of diabetes mellitus, and a DFU. Patients using systemic corticosteroid or immunosuppressive therapy during the PATCH testing were excluded.
This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice. Ethical approval has been given by the Medical Ethics Committee of Nijmegen and the local institutional review board of the Rijnstate hospital. Eligible patients who met the inclusion criteria and signed the informed consent were included. The study protocol was registered in www.clinicaltrials.gov (NCT04085705).
Procedures
A combined PATCH-test (a test used to investigate the origin of an allergic reaction on the skin) of three parts was applied to the upper back (day 0). The PATCH-test were read two days later, at day 2 (D2) and the day after day 3 (D3). The patient has finished the study after the reading appointment at day D3.
The PATCH-test for this study has combined the European baseline series, the European leg ulcer series, 12 and local used material for leg ulcers. 14 The procedure for a PATCH-test was performed according to the European Society of Contact Dermatitis.
The patient, the general practitioner and the treating physician were informed in case of an contact allergy and how to avoid contact with the causative chemical. Wound dressings containing these allergens were avoided in current and future wound treatment.
Outcomes
The primary objective of this study is to determine the prevalence of contact allergies in patients with DFU. Secondary objectives include the correlation between the presence of a contact allergy and the number of ulcers in the past, duration of the current ulcer, and the presence of eczema.
Statistical Analysis
Normality was tested using Kolmogorov Smirnov test together with visual inspection of the normality graphs. Continuous variables were presented as mean with standard deviation (SD) or median followed by interquartile rang (IQR) if applicable. Categorical data, including the prevalence of contact allergies, are presented as a number followed by the percentage. Spearman correlation was used to test for correlations because of the not normally distributed variables. Two sided P-values <.05 were considered as significant. In order to provide unbiased and informative findings, no replacement of missing values was done for any parameter. In all applicable cases, reported analysis will mention the number of missing values for each outcome relatively to the considered analysis set. All statistical analyses were performed using IBM SPSS Statistics version 25.0 for Windows (IBM Corporation, Armonk, NY, USA).
Results
Baseline
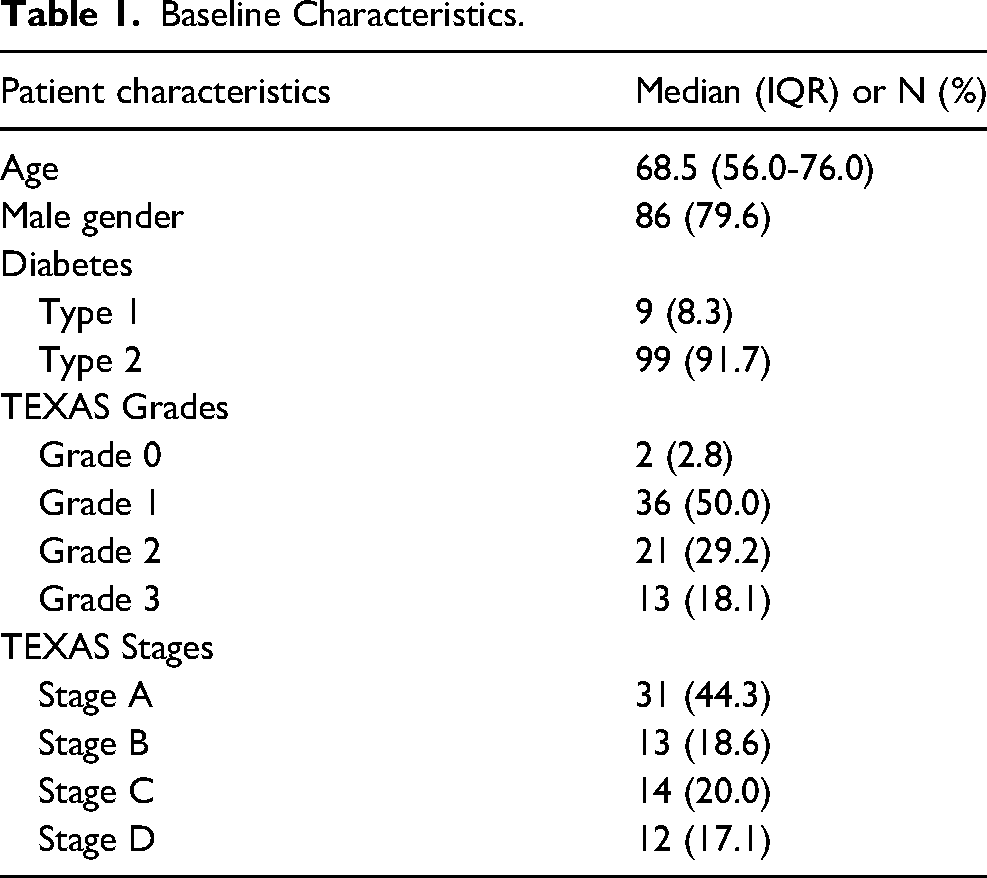
A total of 108 patients were included in the PAID study of which the baseline characteristics are shown in Table 1. The main group of patients had diabetes type 2, with a median duration of 15.0 years (IQR 10.0-25.0). Patients had 1.0 leg/foot ulcers in the past (IQR 0.0-2.0) and a median duration of the current wound of 2.0 months (IQR 1.0-5.0). Five patients (4.7%) had eczema around the current wound and 9 patients (8.6%) experienced eczema in the past. Thirty-eight (35.2%) patients had one or more known sensitizations (anamnestic) at baseline and known atopic constitution was known in 15 patients (13.9%). Median toe pressure was 76.0 mm Hg (IQR 62.75-124.38).
Baseline Characteristics.
Sensitization
It was found that 40 patients (37.0%) were sensitized in either the standard or leg ulcer series. Twenty-one patients showed a reaction in the standard series, 30 patients did react on at least one item in the leg ulcer series, and 11 patients had a positive reaction in both the standard and leg ulcer series. Two patients had a positive reaction on one of the local used materials. Table 2 shows the number of contact allergies of patients in both series.
Number of Patients with Reactions in Standard, Leg Ulcer or Both Series.

Figure 1a shows the number of allergies in the European standard series. Sensitization for Perubalsem is most frequent (N = 6 patients), followed by Fragrance Mix II (N = 4), and Fragrance Mix, Methylchloroisothiazoline, Dibromodicyanobutane (all N = 3). All patients with a sensitization for Fragrance Mix II had no reaction on Fragrance Mix in these series.
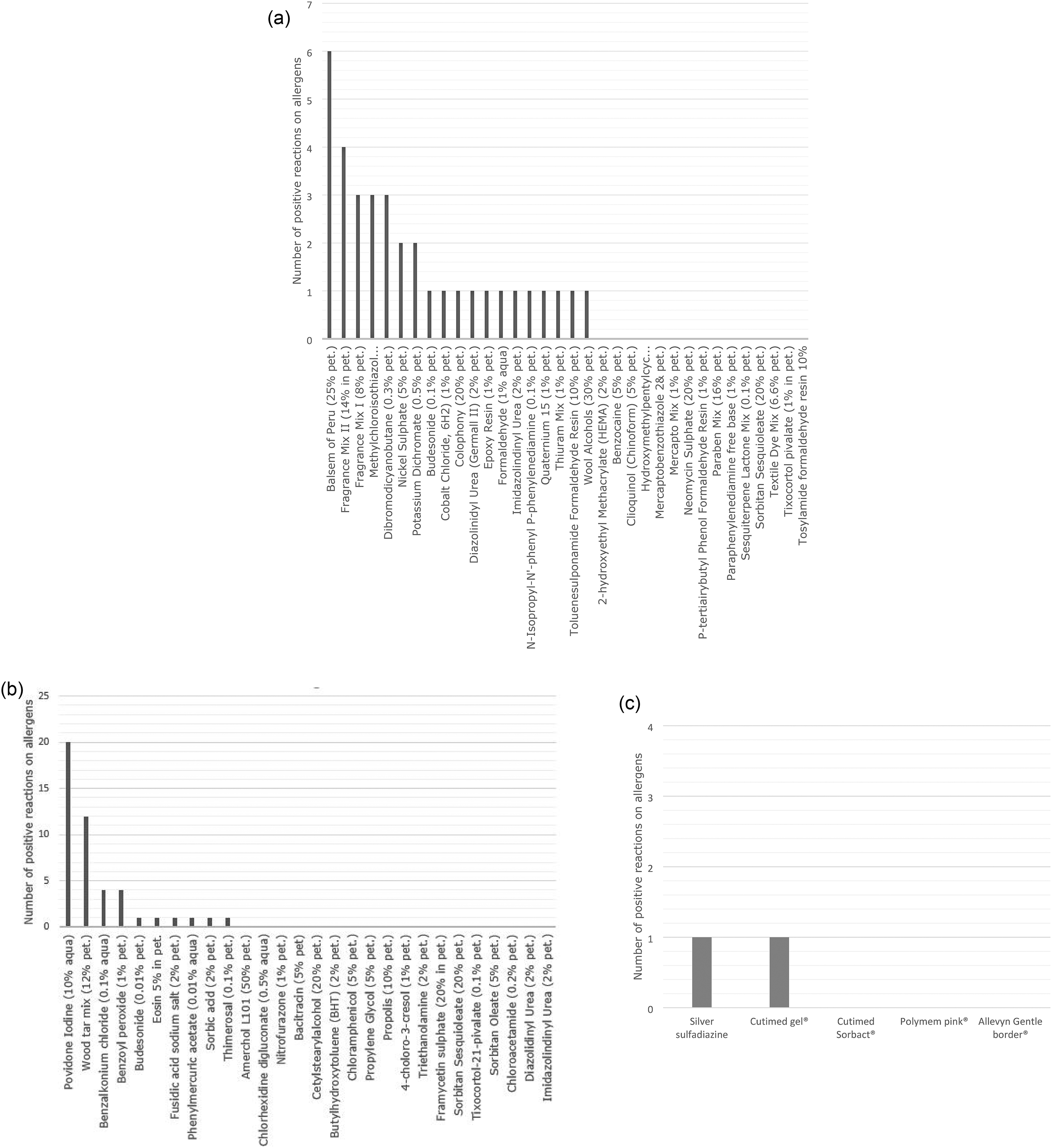
(a) Number of allergies in European Standard series. (b) Number of sensitizations in leg ulcer series. (c) Number of sensitizations in local used materials.
In Figure 1b the number of sensitizations in the leg ulcer series are depicted. Most frequent is sensitization for Povidone Iodine (N = 20), followed by Wood Tar Mix (N = 12). A contact allergy for Povidone Iodine was seen in 20 out of 30 patients with a sensitization in the leg ulcer series. Most frequent contact allergies in patients with a contact allergy for Povidone Iodine were for Wood Tar Mix (N = 6), and Benzalkonium Chloride (N = 3), respectively. Sensitization to lanoline/wool alcohol was low (N = 1) and sensitization to corticosteroid Budesonide was seen (N = 1).
A sensitization for the local used materials are depicted in Figure 1c, with one patiënt having a sensitization for silver sulfadiazine and another patient for Cutimed gel.
No correlation was found for sensitization and patients with eczema on baseline, TEXAS classification (both stages and grades), duration of diabetes, history of ulcers or the duration of the foot ulcer. Duration of the ulcer was higher in the group patients with sensitization than without sensitization but not significant (5,7 vs 4,4 months, P = .523).
Discussion
To the best of our knowledge, this is the first prospective study in which sensitization is tested specifically in patients with DFU. The prevalence of sensitization was lower than the known prevalence of the chronic leg ulcers, 37% compared to approximately 50%. The relevance of this contact sensitization, especially delayed wound healing is still underestimated by clinicians. In general population the prevalence of sensitization is 4.2% to 27%.15,16 In patients with chronic leg ulcers this prevalence of sensitization is clearly higher: 46% to 76%.7,17 Although the opposite is often suggested, modern wound dressings do not eliminate the risk of sensitization. Several studies showed sensitization of modern wound dressings. Due to the use of different ingredients of preservations, fragrance and adhesive in all these products, it is hard to compare these products with each other.
In this current study the prevalence of sensitization to one or more allergens in patients with DFU was 37%. This percentage is higher than in general population, but lower in patients with chronic leg ulcers where the prevalence of sensitization is approximately fifty percent or more.5,7–9 The majority of the tested patients in these studies are patients with venous, or arterio-venous pathology. Most reported sensitizations are for Perubalsem, Lanoline and Fragrance, often 15% to 20%.5,7 For Perubalsem even percentages of 40% are mentioned.5,9 There is no clear explanation why the prevalence of sensitization is lower in DFU compared to chronic leg ulcers. One theory is the immunologic system theory, the immunologic system is too occupied to be involved with sensitization.
In contrary to other studies, this study showed a highest percentage of sensitization to Povidone Iodine (17,6%). This was higher than in other studies, 10-12.7%.9,17 In one study sensitization to specific Betadine crème® was reported in 7,5% in 2002 and 13,9% in 1988 (total of 35 patients). 8 Povidone Iodine is often used because of its antiseptic effect. 18 It had a very low cytotoxicity and inhibits the release of bacterial endotoxine's, such a α-hemolysine. 18
An explanation for this high prevalence might be that Povidine Iodine is commonly used in especially patients with DM with a small skin ulcer, not only on the feet or lower leg, but on ulcers located all over the body. Betadine gaze contains Povidine Iodine. Cross sensitization might also be an explanation. Cross sensitization is seen with desinfectans as thymol-iodide and iodoform. And also in certain cough syrups, iodine is used.
Sensitization to Perubalsem in our study is only seen in 6 patients (5,6%). Sensitization to Fragrance (both Mix added) and Lanoline was seen in 6.5% and 0,9% respectively. This is very low compared to other studies. A lower sensitization might be explained by a lower production of Adenosine Triphosphate, leading to a lower activity of ion canals. This results in a lower immunological activity. Since sensitization in patients with DFU is lower than in regular chronic leg ulcers, an increased sensitization of Povidine Iodine is extra remarkable and relatively very high.
It might be considered to use another local antiseptic, but also these products will increase in sensitization during the years. Favorite products in the past, such as local neomycine, became higher on the list of sensitization, when they were used more often. This incidence has decreased or is even absent since the use is abandoned.
The damaged skin barrier in ulcers of the skin increases the risk of sensitization of used allergens in wound dressings. Allergens cause a T-cell mediated inflammatory reaction leading to delayed woundhealing. Important in making the proper choice for wound dressings is knowledge about the components of this products. Especially Lanoline is used in different products, and certainly in most paraffine gauze and different creams. In daily clinical practice, practitioners will need to be more aware of possible allergic reactions and the use of modern dressing materials. It is often not clear to practitioners which ingredients are used in these dressing materials, partly due to inadequate information provided by manufacturers of dressing materials.
The type IV reactions, tested in this study do not have a significant relation with the type I reaction seen in patients with contrast fluid.
The high number of patients which were tested, strength the importance of testing patients since results seem applicable for all patients with DFU. This study is important because it shows a high prevalence of sensitization and this might not be forgotten by all doctors and health care professionals treating patients with DFU.
This study has several limitations. First, the European leg ulcer series were used to identify allergies. This list is limited, but also outdated for the products used in the Netherlands. Second, the local used materials tested might not be used everywhere. On the other side, it is necessary to show the importance not only using standard series but also local materials to prove sensitization.
In patients with DFU a relevant sensitization to wound dressing of skin product should be considered and tested more often, also in the absence of eczema. This study was performed to determine the prevalence of contact allergies in patients with DFU, but it must be taken in mind that sensitization (allergies) can cause delay in wound healing, as also our data suggest. The role of the dermatologist in the diabetic foot team seems essential to prevent unnecessary delayed wound healing. The importance of avoiding an infection is very important, but if that risk is minimized, other aspects that prevent healing should be considered, such as avoiding allergy for wound dressings.
More research is needed to demonstrate the relationship between allergic reactions and delayed wound healing. In addition to a role for clinics, manufacturers of modern wound dressings have an important role to play in raising awareness of the risks of allergies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.