
Abstract
The aim of this study was to compare the microbial loads of patients with diabetic foot infections treated with negative pressure wound therapy (NPWT) with and without irrigation with polyhexamethylene biguanide (NPWTi-P). This is a post hoc analysis of combined data of two randomized clinical trials. We evaluated people with diabetes treated with moderate and severe diabetic foot infections that required surgery. Tissue specimens were obtained after the initial surgery and following a second planned return to the operating room after 48–72 h of NPWT or NPWTi-P, prior to the second surgery. We used quantitative polymerase chain reaction (qPCR) to determine the total microbial loads (Log10 16S copies per gram of tissue). There was no difference in mean quantitative bacterial cultures among patients that received NPWT and NPWTi-P (before first surgery Log10: NPWT = 6.4 ± 1.8, NPWTi-P = 7.5 ± 1.7 vs before second surgery Log10: NPWT = 6.7 ± 1.8, NPWTi-P = 7.6 ± 1.9 p = .12). There was no difference in wound healing (59.5% vs 50.0%, p = .51) or time to heal (127 ± 109.3 vs 143 ± 95.9), p = .71). There were fewer re-infections in people that received traditional NPWT (28.6% vs 56.3%, p = .05).
Keywords
Introduction
Foot infections are a major cause of hospitalization in people with diabetes and are associated with increased morbidity, mortality, healthcare expenditures, and reduced quality of life.1–5 Infection severity in acute infections of the skin and soft tissue (SSTIs) are driven by the quantity and virulence of the pathogen as well as the host's immunity.6–8 There are many treatments that have focused on reducing the bioburden of bacterial pathogens to improve wound healing and prevent infection.
Negative pressure wound therapy (NPWT) has dramatically changed the treatments and outcomes of complex diabetic foot wounds. 9 Recent advances in NPWT technology have added technology for the simultaneous irrigation of antiseptics to reduce bioburden.1,10 In a porcine model, Davis and colleagues showed that NPWT with simultaneous irrigation reduced wound bioburden. 11 Subsequently, Kim and colleagues evaluated 181 patients with a variety of wound etiologies in a randomized clinical trial and showed a significant decrease in bioburden with period antiseptic irrigation using polyhexamethylene biguanide solution in combination with NPWT. 12 Patients with diabetes and foot complications are a particularly vulnerable population. Therefore, we sought to develop specific evidence to evaluate this high-risk group. 13 The primary aim of this study was to evaluate changes in quantitative bacterial cultures in patients treated with NPWT and NPWT in combination with irrigation in patients with diabetic foot infections that required staged surgical management. The secondary aims are to evaluate the difference in the incidence of wound closure, time to closure and reinfection rates.
Patients and Methods
This is prospective cohort study that used data that was collected during two randomized clinical trials (RCTs) by our team and this is a post hoc analysis.14,15 The data used for this study is combined data from the two RCT's and has not been published before. Permission from the IRB was obtained. From a dataset of 240 patients, 58 patients were eligible for inclusion into this current study. Patients aged >18 years were eligible for inclusion if they were admitted to the hospital with a moderate to severe diabetic foot infection (DFI) as defined by the International Working Group on the Diabetic Foot infection classification. Patients had to have surgical wound appropriate for NPWT and proven ankle brachial index ≥.5. Exclusion criteria included active Charcot neuropathic osteoarthropathy, active malignancy in the wound bed, active alcohol or substance abuse, and unwillingness to take part in follow up visits.
Standard practice for patients admitted with acute foot infections at our institution included staged surgical intervention which included an initial incision and drainage in the operating room, with application of NPWT with or without irrigation with polyhexamethylene biguanide irrigation (NPWTi-P). Patients then underwent a planned second surgical procedure in the operating room 48–72 h following the first surgery. Intra-operative tissue specimens were collected after the first surgery and directly prior to the second surgery. Quantitative polymerase chain reaction (qPCR) was used to determine the total microbial loads from tissue specimens. All participants at admission received empiric antibiotic therapy. In our institution, patients usually receive with either Vancomycin and Piperacillin-Tazobactam or Vancomycin and Cefepime at the time of hospital admission. Conventional culture sensitivities are then used to target antimicrobial therapy. Pre-operative antibiotics have not been shown to affect bacterial cultures, so antibiotics were not held before tissue culture. 16 Wound closure was determined by the treating physician and based on the absence of soft tissue infection and adequate soft tissue for delayed primary wound closure, local rotational flap, split thickness skin graft, or composite bioengineered tissue coverage (Integra Bilayer Matrix Wound Dressing, Integra Life Sciences, Plainsboro, NJ). The patients were then discharged and followed in the outpatient clinic. If the soft tissue defect could not be closed, we provided NPWT at home, supervised by home health nurses. NPWT with irrigation was not available in the home setting, so both study groups received traditional NPWT when home therapy was needed. Patients were evaluated in clinic every 7–10 days. Wound size was evaluated using a 3D measurement device (inSight, eKare, Fairfax, VA), and wound area and volume reduction were calculated as percent change from baseline. 15
NPWT with and Without Installation
Patients were grouped by treatment; group 1 received NPWT alone and group 2 received NPWT with polyhexamethylene biguanide solution irrigation (Prontosan®, BBraun, Melsungen, Germany). Two NPWT medical devices were used throughout the study, (NPWT PRO Therapy System, Cardinal Health™, Dublin, OH, USA and ACTIV.A.C.™ Therapy System, 3M+Acelity, San Antonio, TX, USA); uniform settings of 125 mm Hg, continuous therapy with foam dressings were used for both devices. One NPWT medical device with irrigation (V.A.C. VERAFLO™, 3M+Acelity, San Antonio, TX, USA) was used with continuous irrigation rate of 30 ml per hour.
Sample Collection and Storage
Intraoperative tissue was obtained from the infected surgical site at the conclusion of the first surgery. NPWT with or without irrigation was applied at the completion of surgery and removed just prior to the second surgical procedure. Prior to the start of the second surgical procedure, tissue specimens were obtained for culture. Tissue specimens were flash frozen in liquid nitrogen and stored at −80 °C until analysis of samples was performed.
DNA Extraction and qPCR
Dry tissue was weighed prior to DNA extraction using the MagAttract Microbial DNA Kit (Qiagen, Hilden, Germany) as described by the manufacturer. Briefly, tissue was disrupted in mannose-binding lectin (MBL) and RNase A (ThermoFisher Scientific, Waltham, MA, USA) solution using the TissueLyser (Qiagen, Hilden, Germany) for 2x cycles of 10 min at 30 Hz. The lysate was then centrifuged, and the supernatant collected as input for step 10 of the MagAttract protocol. qPCR was then performed using the 16S forward (CCATGAAGTCGGAATCGCTAG) and reverse (GCTTGACGGGCGGTGT) primers and 16S probe (TACAAGGCCCGGGAACGTATTCACCG). Standards were prepared using the High Pure PCR Template Preparation kit (Roche, Basel, Switzerland) and were run parallel with DNA isolated from tissue. 2.5 uL of DNA was added to 10 uL of Quanta Perfecta Tough Mix (QuantaBio, Beverly, MA, USA) and the reaction was run on a 480 LightCycler (Roche, Basel, Switzerland) with the following cycling conditions: 1 cycle at 50 °C for 2 min, 1 cycle at 95 °C for 10 min, 35 cycles at 95 °C for 15 s and 60 °C for 1 min, and finally 1 cycle at 40 °C for 30 s with the limit of detection being above 30 cycles. The mean standard cycle threshold (ct) values were then utilized to determine the amount of microbial DNA within the tissue samples, which were then normalized to the original weight of non-disrupted tissue.
Data Analysis
We used a Wilcoxon Ranked Sum test to compare continuous variables. We used Fisher's exact test or chi-squared to compare the distribution of categorical variables. Descriptive data are given as mean and standard deviation (±). qPCR values denoting DNA copy numbers were log transformed to normalize data. Test of normality was done using Shapiro-Wilk test. Corresponding mean Log10 values between groups and timepoints were analysed using Wilcoxon Ranked Sum test two-way. We used Statistical Package for Social Sciences Version 27 (SPSS Inc., Chicago, IL, USA) to analyse the data. For all comparisons and modelling, we used an alpha < .05.
Results
A total of 58 patients with infected DFUs were included in the analysis. Demographic, laboratory, and clinical data are presented in Table 1. There were no significant differences in patient demographics and comorbidities between the two treatment groups. The total microbial load Log10 values were normally distributed. There were no significant differences in mean Log10 values between treatment groups before and after surgical debridement and treatment with NPWT (Time point 1 mean Log10: NPWT = 6.4 ± 1.8, NPWTi-P = 7.5 ± 1.7, vs Time point 2 mean Log10: NPWT = 6.7 ± 1.8, NPWTi-P = 7.6 ± 1.9, p = .12) (Figure 1). There was no difference in the healing rate (NPWT 59.5%, NPWTi-P 50.0%, p = .51)), but there were fewer re-infections among patients that received traditional NPWT compared to NPWT with irrigation (NPWT 28.6%, NPWTi-P 56.3%, p = .05) (Figure 2). There was no difference in the time to heal (NPWT 127.2 ± 109.3, NPWTi-P 143.1 days ± 95.9, p = .71) (Figure 3).
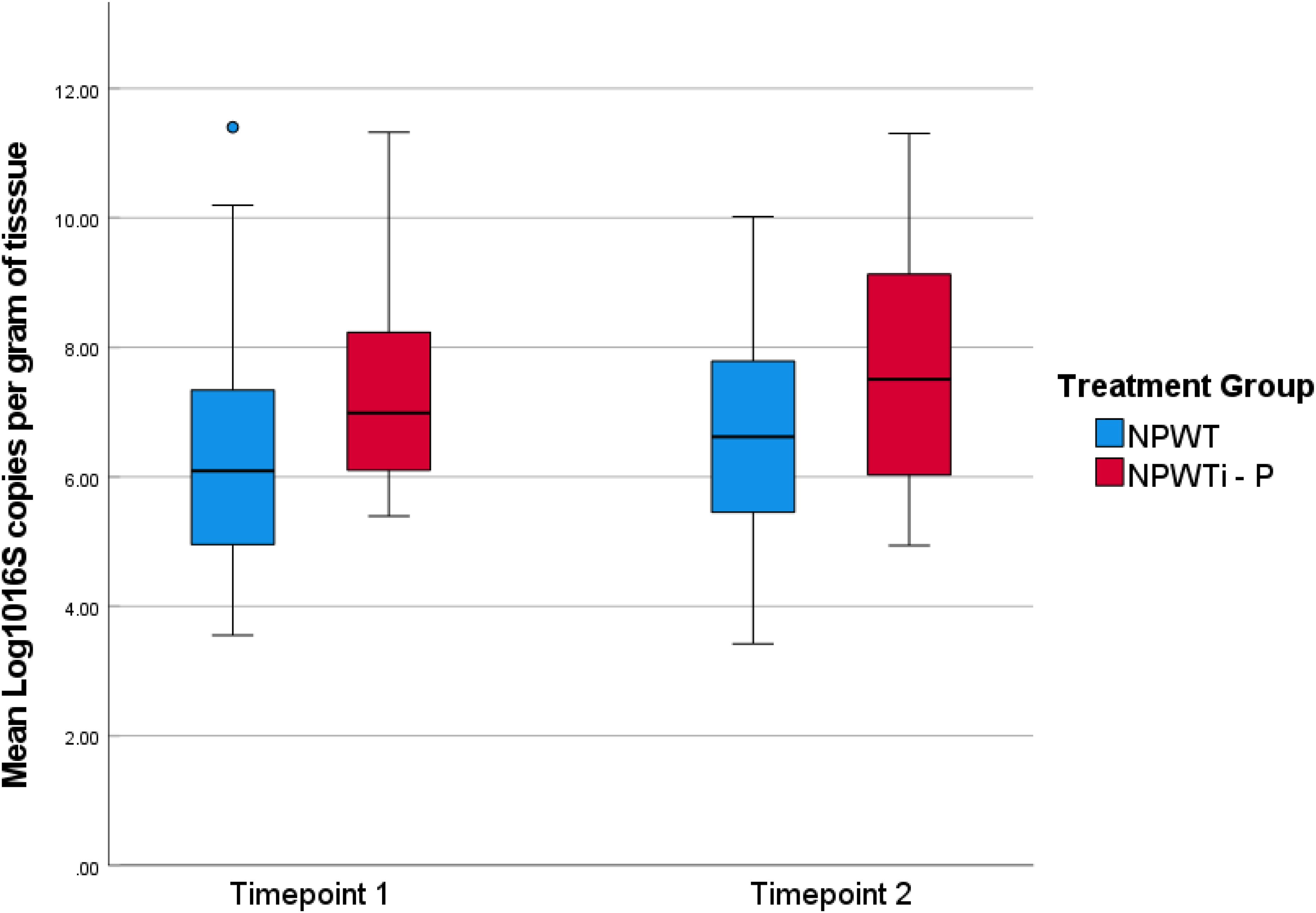
Microbial Loads comparison between Timepoint and Treatment Groups.
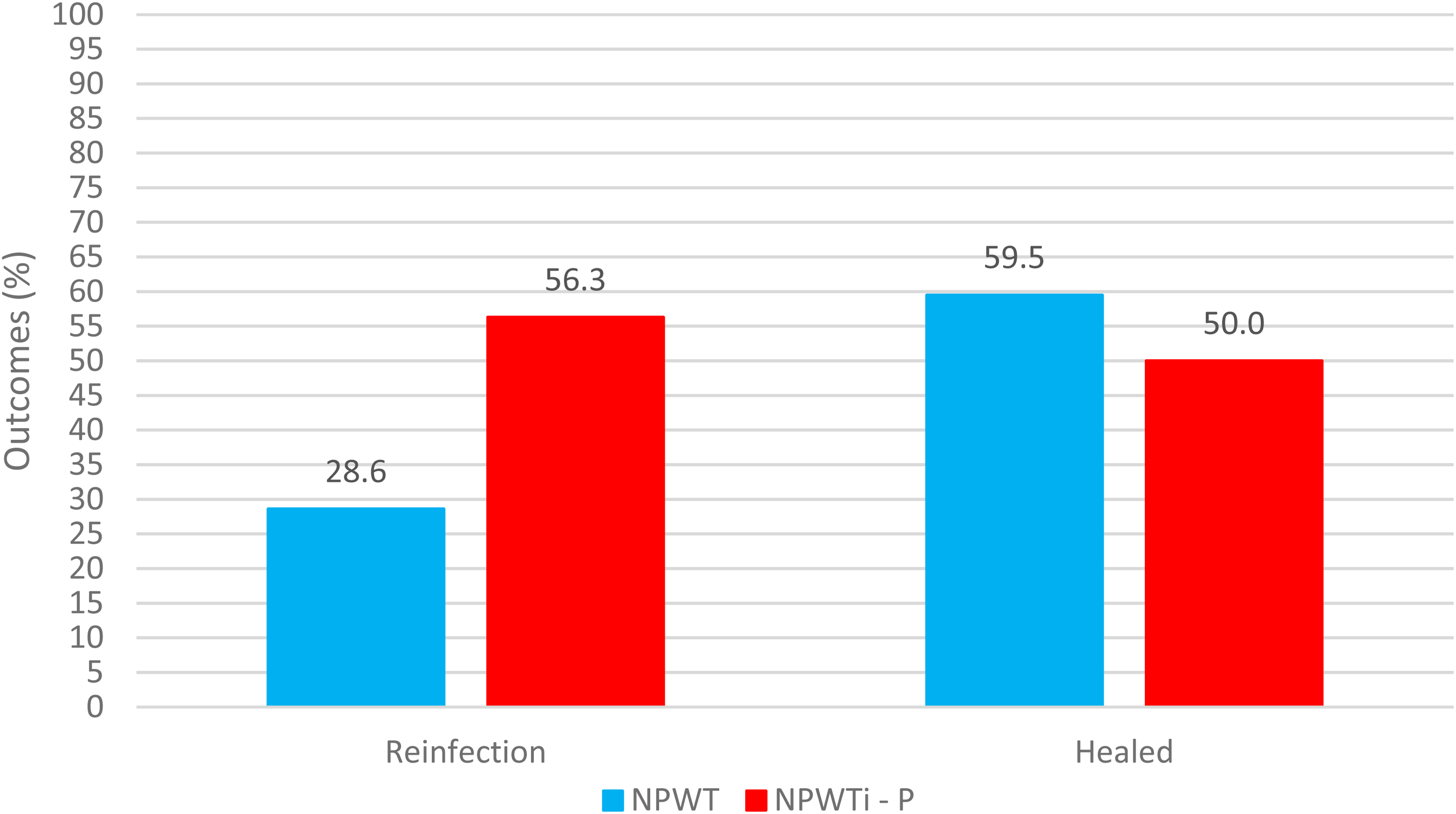
Clinical Outcomes comparison between Treatment Groups.
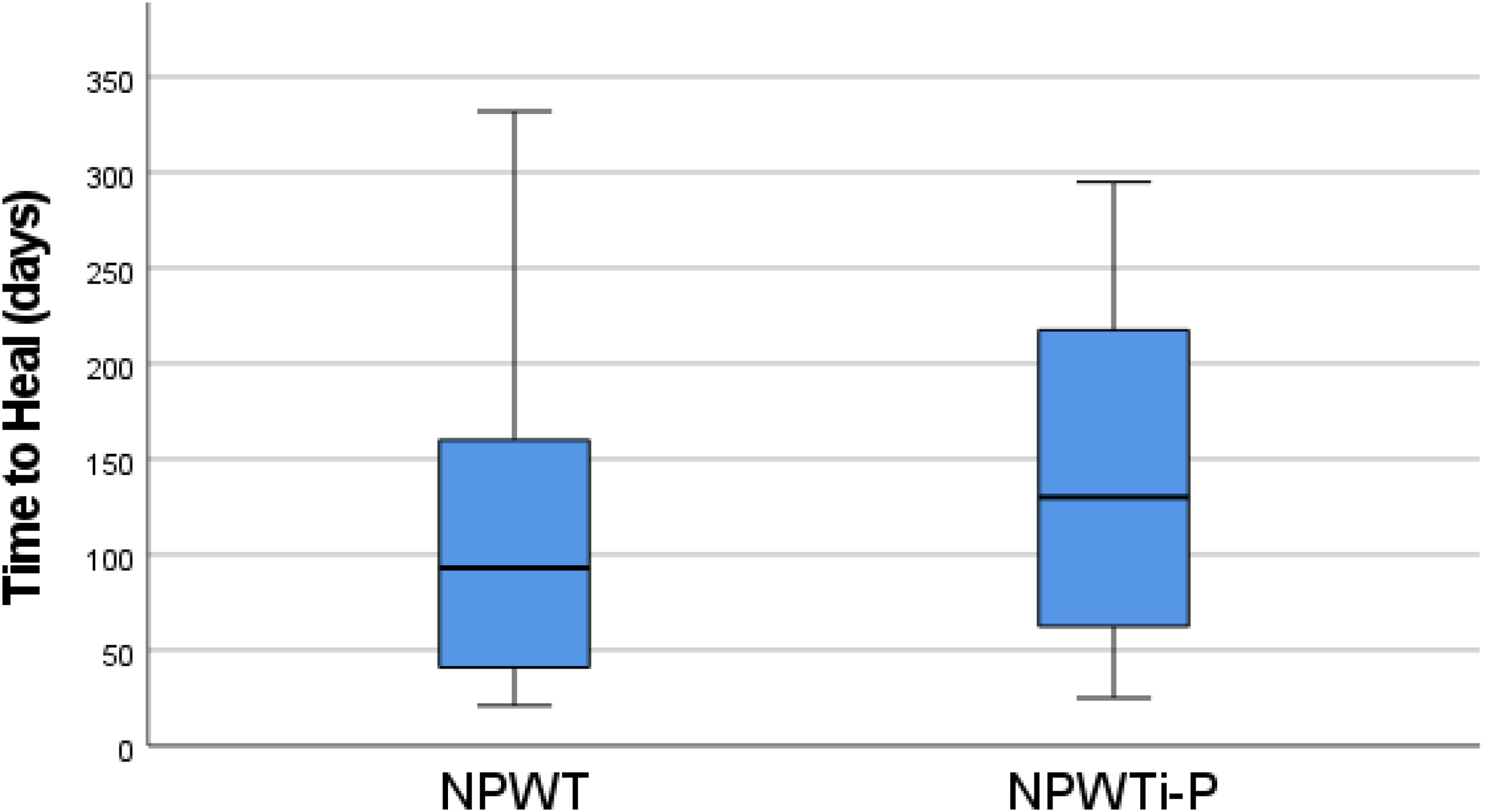
Time to Heal comparison between Treatment Groups.
Clinical metadata of patients presenting with a moderate or severe DFI.
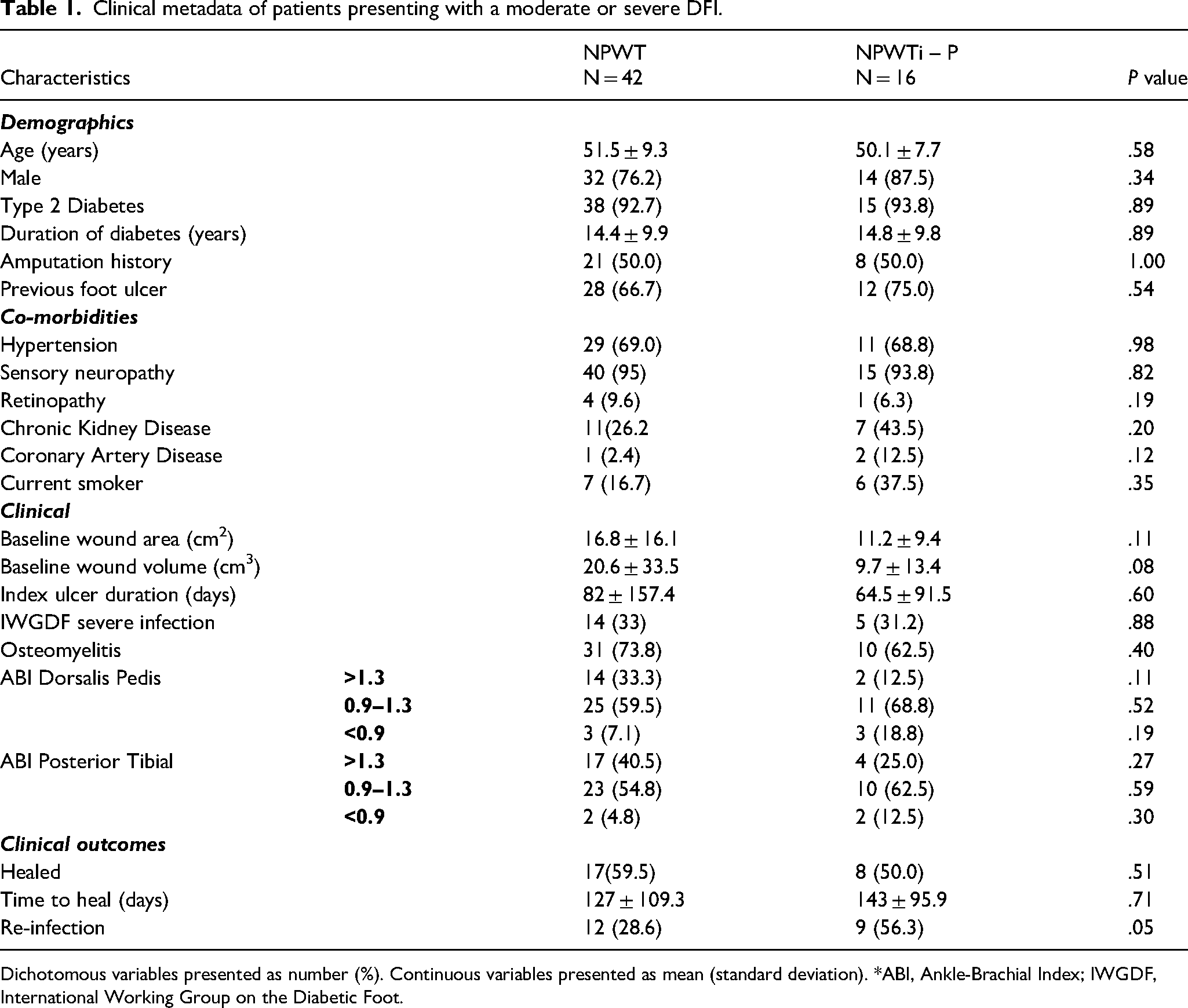
Dichotomous variables presented as number (%). Continuous variables presented as mean (standard deviation). *ABI, Ankle-Brachial Index; IWGDF, International Working Group on the Diabetic Foot.
Discussion
The results of this study show that NPWT with continuous irrigation did not have a significant impact on quantitative bacterial cultures compared to traditional NPWT with no irrigation. There was no added reduction in bioburden, when we combined NPWT with continuous irrigation. There was no difference in bacterial cultures, the incidence of wound closure, or time to closure. There was a significantly higher rate of re-infections in people that received NPWT with continuous irrigation (56.3% vs 28.6%) during a one-year follow-up (Table 1). NPWT without irrigation may be favored in certain situations due to its potential to reduce the risk of maceration and infection compared to NPWT with irrigation, particularly in wounds with fragile granulation tissue or those prone to excessive moisture.
Several animal studies have evaluated antimicrobial solutions in infected wounds. Studies usually show a reduction in bioburden however, the studies that go on to evaluate wound healing do not show any difference in the rate or wound closure. Davis and colleagues evaluate NPWT with high (40 cc/hour) and low rates (15 cc/hour) of continuous irrigation with saline and polyhexamethylene. There was a difference in the reduction in bioburden when NPWT and NPWT with different irrigation were compared. However, there was not a difference in wound healing with NPWT or NPWT with irrigation. 11
Most other animal studies simply evaluate changes in bioburden. Rippon and colleagues found that polyhexamethylene irrigation in a colonized biofilm model resulted in no growth of Staphylococcus aureus at 20 min following exposure. 17 The polyhexamethylene irrigation was also tested on Pseudomonas aeruginosa in the same model, and eradication of the bacteria was seen by 60 min of exposure to the polyhexamethylene. 17 Phillips and colleagues looked at CFU of Pseudomonas aeruginosa after 24 h of NPWT with polyhexamethylene irrigation in a pig model, and found 4-log reduction in bacterial load, compared to saline (p < .001). 18
In human studies, quantitative bacterial cultures were not related to wound healing, time to heal, or re-infection. We have not been able to identify other published work on the effect of NPWT with irrigation on diabetic foot infections. NPWT with irrigation at other wound sites has similar findings.12,19–21 For instance, Kim and colleagues reported the results of an RCT that included subjects with a variety of wound aetiologies. Only 62% of the NPWT group and 63% of the NPWT with irrigation group had infected diabetic foot wounds, so it was not possible to compare our results. 12 In contrast to our study, Kim and colleagues reported a significantly greater mean decrease in total bacterial counts in patients that had NPWT with irrigation. However, like our studies, there was no difference in wound healing. Goss and colleagues reported no difference in bioburden in 13 patients with leg and foot wounds before and after treatment with NPWT with quarter-strength bleach irrigation. Unfortunately, clinical outcomes were not reported. 12
Several other studies report similar results for NPWT without irrigation. A systematic review by Patmo and colleagues evaluated five papers that evaluated the effect of NPWT on microbial load in wounds. 22 Three of the studies were retrospective, and two of the studies were prospective. In a retrospective review, Weed and colleagues found no consistent decrease in semi-quantitative bacterial cultures when comparing pre-NPWT cultures to cultures taken during NPWT treatment. 23 Moues and colleagues evaluated bacterial load from tissue biopsies and found no significant differences between bacterial load in NPWT patients compared to standard of care. 24 However, they found NPWT-treated wounds had a significant increase in Staphylococcus aureus. 25
We expected that NPWT therapy with polyhexamethylene biguanide irrigation would have better performance than NPWT without irrigation based on other published work.1,26 The duration of continuous irrigation was at least 48 h between tissue collection in our study. This would have provided a much longer exposure compared to NPWT technologies that use period irrigation. For instance, in the report by Kim and colleagues, irrigation was provided for only 20 min every 2 h. There was less than a log reduction in bioburden and no difference in clinical outcomes. 12 The exposure of the irrigation solution was much shorter than continuous irrigation.
There is a strong belief that increased bioburden is associated with poor healing and that increased bioburden is linked to an increased risk of clinical infection; however, the evidence does not support these beliefs.12,19 For instance, Kim and colleague showed a significant reduction in CFUs among patients treated with NPWT with periodic irrigation, but there was no difference in wound healing or complications in the treatment arms. 12 In diabetic foot ulceration with no clinical signs of infection, Gardner and colleagues demonstrated that there was not an increased likelihood of wound failure or infection based on quantitative bacterial cultures. The factors related to poor healing were wound size, wound depth and wound duration.27,28
Study Limitations
We have previously acknowledged the limitations of qPCR (based on 16s rRNA gene) and its inability to distinguish viable and non-viable cells. 29 The log reductions noted in this study therefore represent the minimal response and we acknowledge that some of the bacteria detected by qPCR could represent non-viable cells, resulting in a lower calculable efficacy. A limitation of this study is that the location of the wounds was not documented, which could potentially influence wound healing outcomes. Additioally, the absence of a standard dressing control group limits the study's ability to definitively attribute observed improvements solely to the intervention being tested, as some healing might have occurred naturally or with conventional wound care. We utilized additional patient tissue samples that were collected under two previously published RCTs.
Conclusion
This study demonstrated that the use of negative pressure wound therapy (NPWT) with or without irrigation with polyhexamethylene biguanide does not significantly impact the bacterial load in infected wounds undergoing staged surgical intervention. We also found that the addition of continuous irrigation to NPTW resulted in higher re-infection rates at one-year follow-up compared to NPWT alone.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is a sub analysis of combined data from two randomized clinical trials. The randomized clinical trials were separately funded by American Diabetes Association (NCT02308800) and Cardinal Health (NCT02519621). L.A.L is the recipient of both grants.