
Abstract
Chronic limb-threatening ischemia (CLTI) represents one of the most severe forms of peripheral arterial disease implying impaired wound healing and tissue loss at the same time posing a significant impact on the quality of life of patients and a serious economic burden on healthcare systems around the world. A major challenge in the management of patients with CLTI is the validity and role of non-invasive hemodynamic parameters in assessing their clinical status before and after revascularization. Traditionally, the diagnosis of CLTI is routinely based on clinical symptoms and confirmed by measurements of non-invasive limb hemodynamics including ankle-brachial pressure index (ABPI) and toe-brachial pressure index (TBPI). However, whether these indices alone can provide definitive treatment or be used as adjunctive tool along with the implementation of novel techniques to help guide revascularization for CLI patients still remains unclear.
Keywords
Peripheral arterial disease (PAD) is characterized by arterial obstruction and impaired blood flow, mostly in the lower limbs, caused mainly by atherosclerosis. Although PAD involves a broad spectrum of vascular territories such as mesenteric as well as head, upper extremity and neck vessels, the evaluation and post-treatment of atherosclerotic vascular disease in the lower extremity (ilio-femoral, femoro-popliteal and femoro-distal arterial axes) are reviewed in the present study. The disease shows a high prevalence in the elderly, reaching up to 25% in this population and it is well-documented in the literature as a strong predictor of cardiovascular (CV) morbidity and mortality, leading to serious and potentially catastrophic sequelae, especially if left untreated or remains underdiagnosed.1,2 Chronic limb-threatening ischemia (CLTI) represents one of the most severe forms of PAD implying impaired wound healing and tissue loss at the same time posing a significant impact on the quality of life of patients and a serious economic burden on healthcare systems around the world. 3 A major challenge in the management of patients with CLTI is the validity and role of non-invasive hemodynamic parameters in assessing their clinical status before and after revascularization.
Traditionally, the diagnosis of CLTI is routinely based on clinical symptoms and confirmed by measurements of non-invasive limb hemodynamics including ankle-brachial pressure index (ABPI) and toe-brachial pressure index (TBPI). 4 These measures are also used to confirm eligibility and quantify response to therapy in PAD patients participating in clinical trials where ABPI or TBPI increases >0.15 are taken as evidence of hemodynamic success. 5 The term ABPI was recommended by the recent American Heart Association Proceeding on Atherosclerotic Peripheral Vascular Disease on the basis of its current widespread use in contemporary literature and accordingly in epidemiological studies, an ABPI lower than 0.9 is often used to define PAD. 6 The National Institute for Health and Care Excellence (NICE) guidelines and European Society for Cardiology (ESC) guidelines recommend that PAD presence and severity are assessed by measuring ABPI.7,8 However, in other National and Societal guidelines, the association between changes in these hemodynamic parameters and clinical outcomes following revascularization still remains unclear. 9 Summarizing data are presented in Table 1.
Data of national and societal guidelines on ABPI on diagnosis, interpretation and follow up treatment of PAD patients.
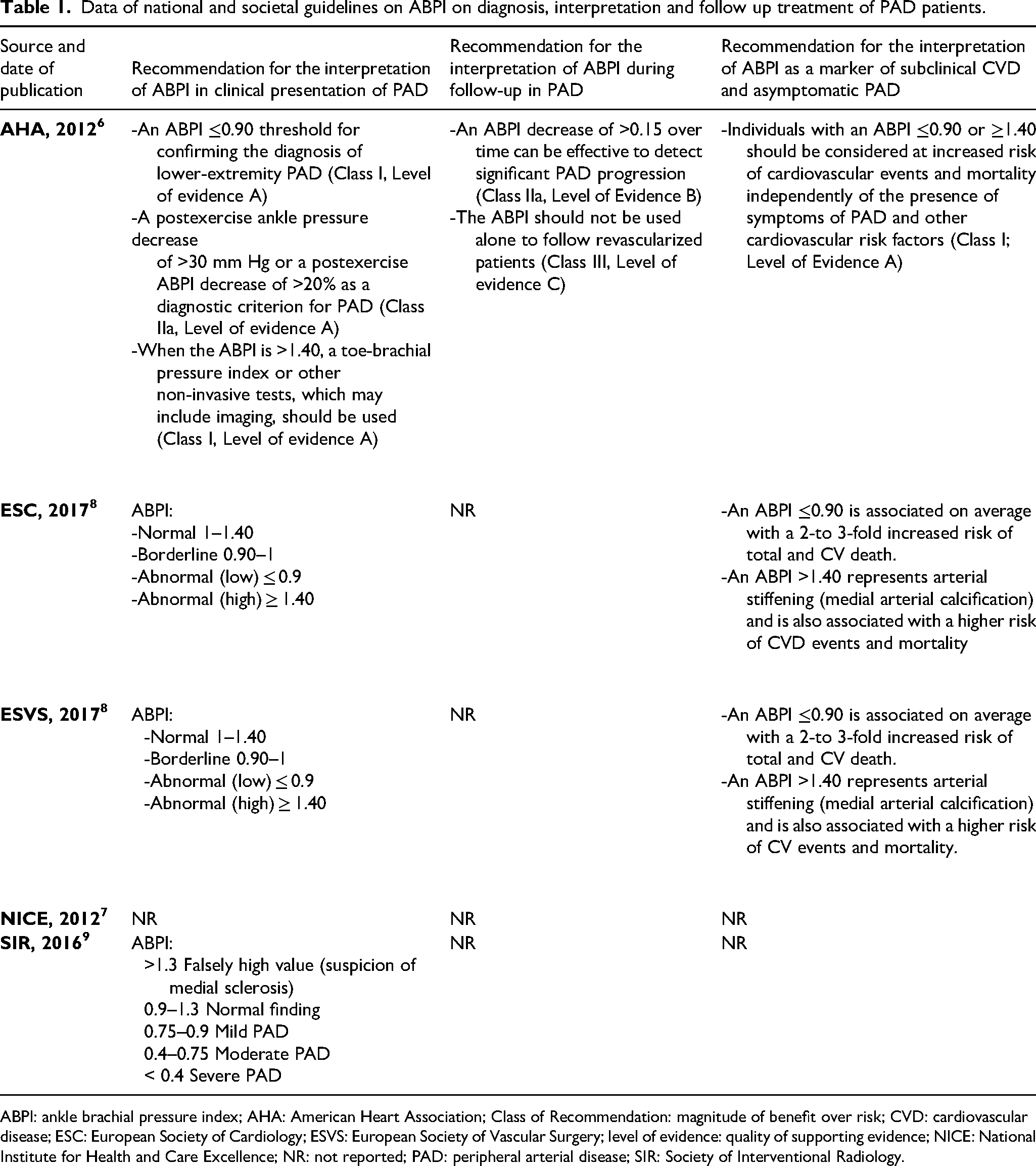
ABPI: ankle brachial pressure index; AHA: American Heart Association; Class of Recommendation: magnitude of benefit over risk; CVD: cardiovascular disease; ESC: European Society of Cardiology; ESVS: European Society of Vascular Surgery; level of evidence: quality of supporting evidence; NICE: National Institute for Health and Care Excellence; NR: not reported; PAD: peripheral arterial disease; SIR: Society of Interventional Radiology.
One of the challenges in treating patients with ischemic tissue loss is objectively determining what constitutes sufficient revascularization, that is, providing perfusion above the threshold that will allow wound healing. In a single-centre study which enrolled 100 patients from the PRIME (Peripheral Registry of Endovascular Clinical OutoMEs) registry and underwent infrapopliteal endovascular revascularization, there was no statistically significant change between the pre-treatment and the post-treatment limb hemodynamic values of ABPI and TBPI after successful infrapopliteal endovascular therapy. 10 The authors concluded that re-evaluation of these parameters for assessing response to therapy in interventional CLTI patients is mandated. 10 Bunte et al evaluated the relationship between ABPI and TBPI in 66 patients with CLTI and concluded that nearly one third of patients with minor or major tissue loss had normal or mildly reduced ABPI. Furthermore, among patients with borderline to normal ABPI results, concurrent TBPI was abnormal in all (39 patients). However, a significant limitation of the study was the lack of comparative indices in pre- and post-operative status of the patients regarding wound healing process.8,11
The traditional target for treating CLTI with tissue loss is re-establishment of in-line flow to the foot of the affected limb either surgically or by endovascular techniques. 12 The angiosome concept, providing direct in-line flow to the specific vascular bed directly perfusing the ischemic zone, has been also advocated as a guide for PAD revascularization. 13 In this respect, the role of a non-invasive hemodynamic parameter such as ABPI and TBPI may be more appropriate for use in screening programmes rather than help guide the extent of sufficient revascularization or wound healing. Watson et al in their recent systematic review evaluated six ABPI and TBPI measurement portable devices and they concluded that all included devices had moderate levels of sensitivity and high levels of specificity ranging from 20% to 70% and 86% to 96% respectively and that their sole use in screening programmes could be a useful tool for evaluation of patients with CLTI. 14
Whereas ABPI and TBPI are the most frequently used parameters to assess PAD severity, these non-invasive hemodynamic parameters have important limitations, especially in patients with calcified arteries, in elderly patients and in those with diabetic and renal disease, resulting in a falsely increased values which can lead to misdiagnosis or ineffective treatment after revascularization.11,15 Medial arterial calcification (MAC) seems to be an explanation for such lack of sensitivity. In MAC, calcium deposits in the muscular middle layer of the arteries, thus turning the vessels rigid and poorly compressible, which results in an overestimation of ankle pressures by ABPI. Subsequently, it may result in falsely elevated or falsely normal ABPI values, making this measure unreliable to guide diagnosis, clinical practice and further management. 16
Another important limitation of these non-invasive indices in monitoring PAD patients after revascularization exists, where ABPI change correlates poorly with improvement in symptoms or functional performance. According to Decrinis et al, after angioplasty, an ABPI increase of 0.10 and 0.15 in the revascularized limb predicted no residual stenosis >50% with pre-op and post-operative sensitivities of 79% and 67% and specificities of 92% and 100%, respectively. 17 The ABPI may continue to improve from that measured in the immediate postoperative period for several weeks or months after revascularization. 18 However, the ABPI is a global estimator of whole-limb perfusion and cannot distinguish between graft failure and progression of PAD in native arteries. 19 The ABPI is not site specific and may reflect changes elsewhere in the arterial tree and considering its low sensitivity for predicting graft failure, the measurement of the ABI alone is not a reliable method of surveillance after revascularization.20,21
However, use of traditional techniques has not become obsolete and could be used as an adjunct in CLTI diagnosis and follow up. The pole test is an alternative approach first introduced by Smith et al 22 Using this test, the systolic ankle pressure can be measured by slowly elevating the patient's leg to a level where the Doppler signal vanishes during insonation of the posterior tibial or dorsalis pedis artery, and then lowered until an audible signal reappears; the height at which the signal reappears is the “pole” pressure. The height in centimetres could be converted to millimetres of mercury. When used in the toe, the test can assess pressures less than 70 mm Hg, whereas only pressures less than 45 mm Hg can be assessed at the ankle level as the height that the foot is elevated could not exceed 60 cm. This is a simple low tech method that could be used on the ward, especially on patients who are unable to tolerate the pressure of the cuff or those with MAC and false elevated ABPI.23,24 Last but not least, tests that mimic the walking stress could be used to uncover mild disease. Some patients with PAD present with normal systolic pressures at rest. A normal response is a slight increase (<10%) or no change in ABPI, but if it decreases immediately after treadmill exercise, the test is considered positive. 23
Novel techniques measuring the incremental change, rather than an absolute value, to predict wound healing may help guide revascularization and provide better outcomes for CLTI patients have already been described in this study. 25 Furthermore, a non-invasive hemodynamic parameter to help guide the extent of anatomic revascularization in patients with CLTI, while balancing the risks of longer or technically challenging procedures, would be extremely helpful. In this respect, Reed et al attempt to define threshold hemodynamic parameters to predict wound healing in patients with CLTI after an endovascular revascularization using the change in ABPI and TBPI. Endovascular treatment was performed in 218 CLTI patients for minor and major tissue loss. An increase in ABPI ≥0.23 was associated with a greater probability of wound healing, less repeat revascularization, and no change in major adverse limb events (MALE). An increase in TBI ≥0.21 was associated with a greater probability of wound healing, fewer MALE, but no reduction in repeated revascularization attempts. 25
Whereas in the literature there are plenty of articles separately examining the accuracy of ABPI and TBPI, only one study exists that jointly combines and compares these two indices as to their efficacy in diagnosing or assessing PAD. In this meta-analysis, comprising 35 studies for ABPI and 9 studies for TBPI, TBPI showed far better sensitivity than ABPI (81% vs 61%), although specificity was worse (77% vs 92%) and showed moderate heterogeneity (I2 = 49.4%). 26 This fact may position TBPI as a better test to work as a screening test while ABPI could work better as a diagnostic test. Another rationale for the above-mentioned lack of sensitivity in ABPI could be MAC, which turns vessels rigid and poorly compressible. Since the collateral vessels of the toe are relatively unaffected by MAC, TBPI has emerged as a promising diagnostic test to diagnose PAD, especially for those patients’ suffering MAC. 26
Multiple methodologies have been tested to improve our ability to predict wound healing. These include transcutaneous oxygen tension, 27 photographic thermography 28 and laser Doppler skin perfusion pressure changes. 29 Research is ongoing in the field of computed tomography perfusion scanning to evaluate the ischemic limb and adequacy of perfusion for wound healing. 30 Magnetic resonance imaging techniques are in development to assess limb perfusion, including arterial spin labelling to assess oxygen concentration of tissue. 31 However, more research is needed to determine the efficacy of advanced imaging techniques for predicting the adequacy of revascularization in CLTI patients.
The goal of revascularization in CLI patients is to promote wound healing, prevent amputation, preserve limb function and decrease mortality. Traditional non-invasive measurement tools such as ABPI and TBPI have inherent drawbacks that limit their use as a single guide to therapy and clinical follow-up. However, these indices could be used as adjunctive tool along with the implementation of novel techniques and methodologies to help guide revascularization and provide better outcomes for CLTI patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.