
Abstract
The triad of ischaemia, neuropathy, and infection are among the principal causes of lower extremity wounds that are commonly prevalent in patients with diabetic foot (DF) a condition in which peripheral arterial disease commonly co-exists. The prevalence of this condition is increasing globally and with it, the mounting costs of its management. One aspect of management is saving limbs and or digits, a crucial part of this process is assessing tissue viability of skin which is a focus of this review: there are other aspects which are well described in the literature. Amputations are offered to limit the damage resulting from acute/chronic ischaemia. Holstein measured skin perfusion pressure using a radioisotope clearance technique to describe critically ischaemic skin; he found 30 mm Hg as the threshold above which healing may reliably be expected. Recent advances in vascular surgery and related technology have informed evidence-based advice to revascularize and save limbs; in practice, this may leave a wound in the distal skin unhealed; managing these raises questions of tissue viability. Much effort has been made to manage, prevent and to better understand these lower extremity wounds using measurements of tissue oxygen, oxygen saturation and skin imaging. The measurement techniques and their relevant merits are examined in this article. Advances in wound management systems and protocols can also facilitate the repair processes, and those which can have a particular impact on restoring or maintaining tissue perfusion are also discussed in the article.
Keywords
Background
Saving limbs to save lives is a continuing clinical challenge in an environment where the incidence and prevalence of both peripheral arterial disease (PAD) and diabetes mellitus (DM) are increasing; this applies to low- to middle-income groups and both genders.1,2 Soyoyo estimated that PAD was 2-7 times more prevalent in subjects with DM than without it.
3
Another article reported that subjects with DM have,
4
a fourfold increase in the incidence of PAD and mortality, with a reduction in quality of life and are at an increased risk for disability. 15%-45% of DM have PAD in 10 years or more. 75% of DM with PAD are symptomatic for claudication or rest pain. subjects with DM and PAD are at increased risk of infrapopliteal disease affecting the tibial vessels with calcification and sparse collaterals. Lower limb pain could be missed during clinical assessment in subjects with DM. Amputation rates are high due to recurrent ulcers, comorbidities and end-organ damage.
5
The amputation coalition estimated that overall amputation rates increased during the recent COVID-19 pandemic due to complications and notwithstanding the increased use of telehealth options for patients foregoing outpatient appointments.
5
The challenge is real, massive and upwardly trending. PAD may lead to acute or chronic limb-threatening ischaemia: in the diabetic foot (DF) condition limb-threatening PAD can and does get compounded by microcirculatory damage leaving foot skin at risk to wounds caused by diabetic neuropathy, neuroischaemic or, in a non-diabetic subject, ischaemic leg ulcers. The purpose of this article is to critique the means of measuring the viability of skin at risk.
Clinical Assessment
When a limb or foot skin is at risk from underlying PAD, DM with or without complications, its presentation is defined by the absence/diminution of pulses, changes in colour, temperature, pain (which is diminished in the presence of sensory neuropathy), also accompanied by gangrene and offensive odour. Increased redness and warmth and pain broadly characterise severely ischaemic tissue. Subjects with neuropathy cannot sense pain, an important consideration to remember while planning treatment or prevention. With regressing ischaemia, tissues turn cold and purple: the presence of gangrene may be evident as dry (in critically ischaemic tissues) or wet skin (when there is an underlying infection, commonly in the DF). 6 Historically, the literature in this area aimed to identify a level of amputation that permitted healing, limb rehabilitation and an acceptable quality of life. In recent decades, revascularisation of limbs gained wider acceptance, aimed to save limbs extending as far as possible to the ankle: this would leave the foot to be perfused by such remaining flow as existed in the dorsal arteries: perfusion pressure at ankle level is reliably expressed by ankle-brachial pressure index (ABI or ABPI).
Skin Perfusion Pressure (SPP)
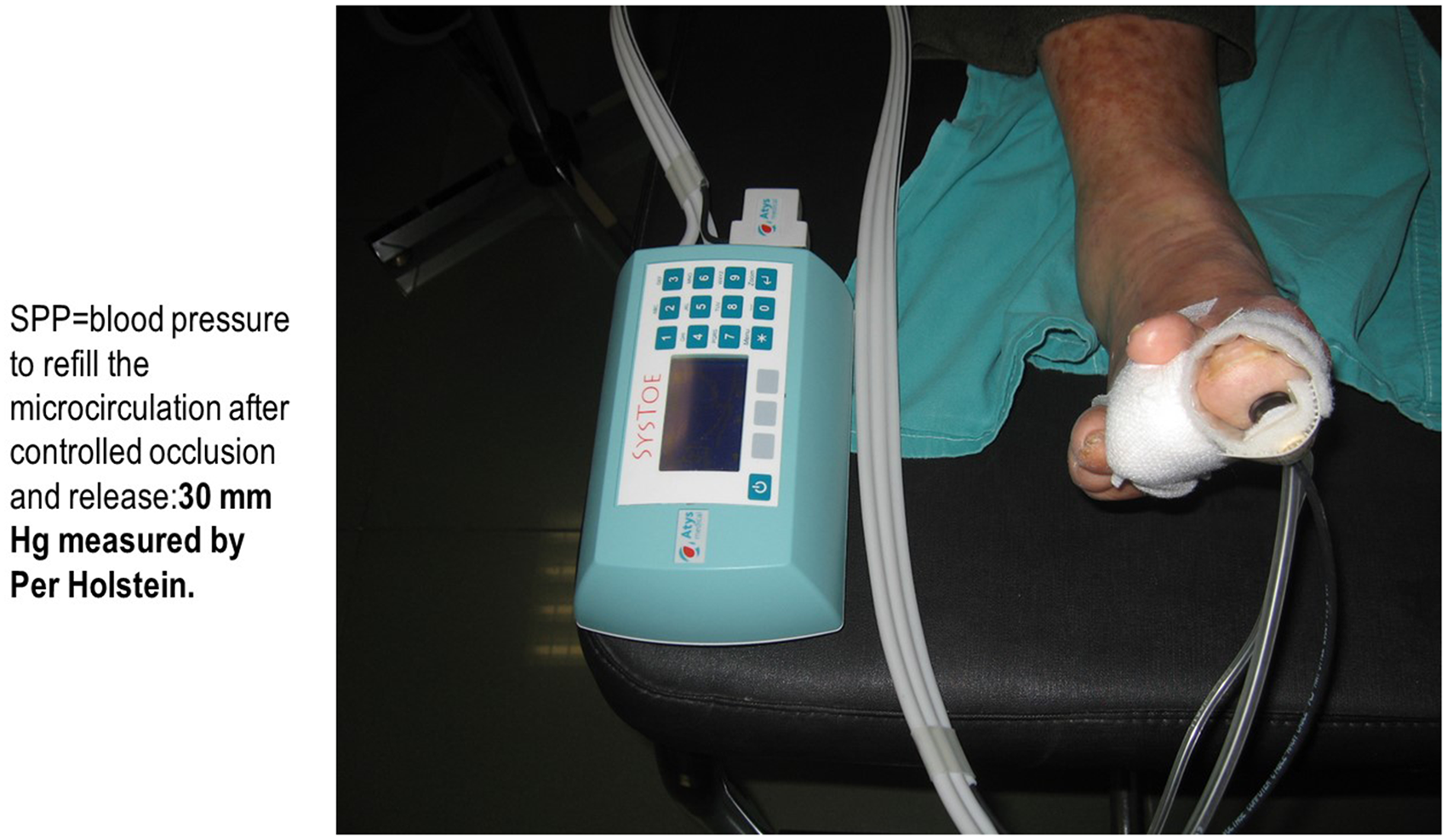
As skin perfusion decreases to zero consequent to advancing significant limb ischaemia, there is net deprivation of skin blood flow and oxygen leading to cell death and ulcers. In this state, skin also loses its ability to autoregulate. Holstein defined SPP as that pressure when radioisotope-tagged blood flow from a sample volume was occluded using a guard ring. He used the radioisotope iodine I131 to tag blood within a defined sample of tissue, and a scintillation counter to detect flow once the counter pressure exerted by the guard ring was released: this was defined as SPP. He reported 30 mm Hg to be SPP on the legs of subjects. 7
In a report to follow, Holstein studied SPP and measured radioisotope clearance in ischaemic limbs that were amputated and reported that limbs with SPP > 30 mm Hg had the best healing: by comparison limbs < 30 mm Hg were associated with failure to heal and SPP was 20-30 mm Hg this associated with variable results. 8 Holstein's report mentioned that some of the included patients were diabetic subjects though details were lacking as to whether these were neuropathic, neuroischaemic or whether they were infected. Notwithstanding this limitation, this definition of SPP opened a door to objective guidance on level of amputation. The clearance of radioisotope technique yields absolute values, it gained recognition as a gold standard. The limitations of the method were, repeat measurements were inherently risky and test facilities with adequate health and safety provisions were only available at the bigger clinical centres with adequate laboratory support. The use of radioisotope 4-iodo antipyrine and a gamma camera to accurately measure tagged skin blood flow at amputation sites improved the Holstein technique: despite its accuracy, this method lacked universal appeal. 9
Other contemporary reports were based on detecting blood vessel pulsatility, blood volume (plethysmography), phase shift of erythrocytes within the capillaries (laser Doppler flowmetry [LDF]/laser Doppler imaging [LDI]), temperature changes (thermography), imaging perfusion using sodium fluorescence infra-red detectors, measuring tissue oxygen partial pressure using electrochemical sensors and measuring tissue oxygen saturation using optical detectors.
Broadly, optical sensors rely on detecting either the reflected or the transmitted fraction of light incident on tissues, this volume fluctuates in synchrony with the subject's heart rate. Such sensors may be flat in profile or shaped as a U clip: these detect either the reflected/transmitted blood volume changes or colour and volume changes depending on the wavelength of light: colour changes in the blood are driven by its oxygen saturation, a relationship defined by Beer Lambert's Laws. The wavelength of light used is critical: in the infrared range light transmittance is independent of colour while at lower wavelengths, it is colour sensitive. The wavelengths that are very important in this context are 633 nm (when transmittance is maximally different) and 805 nm (where transmittance is not affected by colour of blood), this is the principle of pulse oximetry. Optical sensing of blood pulse volume is % volume change, oxygen saturation is expressed as a percentage.
LDF and LDI are optical methods that may be used to detect skin perfusion with the difference that LDF accurately senses blood cell movement; the detected fraction is dependent on the phase shift of erythrocytes in the fractions of blood volume sensed. Hence these devices were called flowmeters: the technique was later used to image tissue and found use in detecting amputation levels on skin and are discussed below.10,11 LDI imaging also offers an accurate means of estimating dermal depth damage in burn wounds compared to both clinical judgement and histology; this is a very valuable application though not discussed in this report. 12
Lee Yong used a LDF and a narrow cuff to measure SPP with an aim to study its association with endovascular therapy to treat PAD. 10 The LDF was positioned on digits, towards the inner or outer aspects of the foot to record flow from the digital, dorsal or pedal arteries, respectively. In this study of patients with chronic PAD Rutherford classification 5 or 6. Lesions were located on the feet or ankles. Patients N = 172 with 236 limbs were supine during the tests, the Wound, Ischaemia, Foot, Infection (WiFi) scoring system was also used. 13 Comparative measures of ankle to brachial measurements and other tests were also done routinely. Wound healing was regularly reviewed and scored by clinicians. Analysis of the data showed that SPP ≥ 50 mm Hg was associated with better outcomes and superior to SPP ≤ 30-40 mm Hg, SPP ≤ 30mm Hg was associated with poor healing. Data analysis showed sensitivity, specificity and overall accuracy of predictive value were superior at SPP ≥ 50 mm Hg. Patient selection in this study was non-randomised in this single-centre study. Overall, the study indicated that the measurement of SPP could guide therapy though study limitations reduced the impact of the findings.
In an earlier report, Grabbe et al reported a study to determine the effect of SPP values on lesion healing on N = 53 patients (62 limbs). 11 Patients had ischaemic foot ulcers treated with conservative therapy based on SPP measured pre- and post-therapy at 4 weeks. SPP > 40 mm Hg was found to be 75% sensitive, 82.6% specific with 80.6% overall accuracy. SPP >40 mm Hg with odds ratio OR 14.2 (95% confidence interval 3.6-55.8) was an independent predictor of healing and had ‘strong correlation’ with toe pressure. Patient selection was not randomised which limited the value of this evidence.
Concurrent with advances in optical measurements, studies emerged of the measurements of tissue oxygen using skin sensors at wound sites to be followed by oxygen saturation optical sensors and fluorescence imaging as discussed in this review. Tissue oxygen measured using skin sensors is a non-invasive, accurate method of measuring the partial pressure of tissue oxygen available: it relies on heating the skin to its maximum vasodilatory capacity. Partial pressure of tissue oxygen (TcPO2) depends directly on oxygen delivered and indirectly so on the resistance to oxygen diffusion from increasing intercapillary distance and oedema. 14
Skin surface oxygen sensors must never be left on site for longer than 2 h. The technique, limitations and applicability to study tissue viability at perilesional skin sites around venous leg ulcers, ischaemic leg ulcers and DF skin have been reported: Arsenault 15 reported after a systematic review and meta-analysis of data from 901 patients (911 lower extremity wounds from 4 studies). Using TcPO2 cut-offs of <20 mm Hg and <30 mm Hg, it was an independent predictor of chronic wound complications with OR 3.2 95% CI (1.07-9.62). Above 30 mm Hg, TcPO2 is associated with reducing probability of amputation and wound healing and is associated with similar values of oxygen saturation derived using optical probes. 16 TcPO2 is recommended in guidelines for wound management. 17
Optical measurement of oxygen saturation (OS) using flat or clip-type sensors is non-invasive, simple to use and no skin heating required: readings are in percent OS. This is widely accepted in clinical practice including Emergency Departments. There is an argument based on theoretical considerations that this technique may underestimate OS on dark skin. These studies suggest that skin perfusion may be accurately measured using LDF while skin surface sensors and optical sensors of oxygen saturation are both accurate and broadly in accord with each other.
When an intravenous injection of indocyanine green is given, the dye tags flow in the vascular system and the resultant autofluorescence is detected using a near Infra-Red (NIFR) sensing, regional tissue viability can be viewed and mapped. It is a minimally invasive technique. Images of areas or regions of viability make this an attractive in-theatre use for many surgical specialties including vascular and plastic surgery. Measurements of these images are based on dye wash-in/dye wash-out times, maximum intensity of dye uptake, time taken to reach 50% of maximum intensity, area under the wash-in and wash-out time curves. 18 The quality of results obtained depends inter-alia on NIFR sensor intensity, camera angle, lighting, camera distance and dose delivered. Goncalves et al reviewed a sizeable body of published data that analysed fluorescence imaging measurements carried out in many surgical specialties including plastic and vascular surgery. These measurements included times for wash-in and/or wash-out of the dye, time taken to reach maximum intensity (perfusion), maximum value of perfusion, area under the curve among others: the wash-in/wash-out curve of the dye is approximately an inverted. V. Goncalves did not recommend any specific analytical method though Brownriggs et al argued in favour of including fluorescein uptake image from the ‘toe slope’ of <18 units: this is discussed in a later section. 19 Since wound healing can and is often delayed in the cohort of patients with PAD and diabetes, valuable measures are described in the following section (Figures 1-3).
An optical sensor used to measure toe blood pressure (cuffs not shown in the figure).

Measuring transcutaneous oxygen tension using skin surface sensors near an ischaemic lesion on a toe.
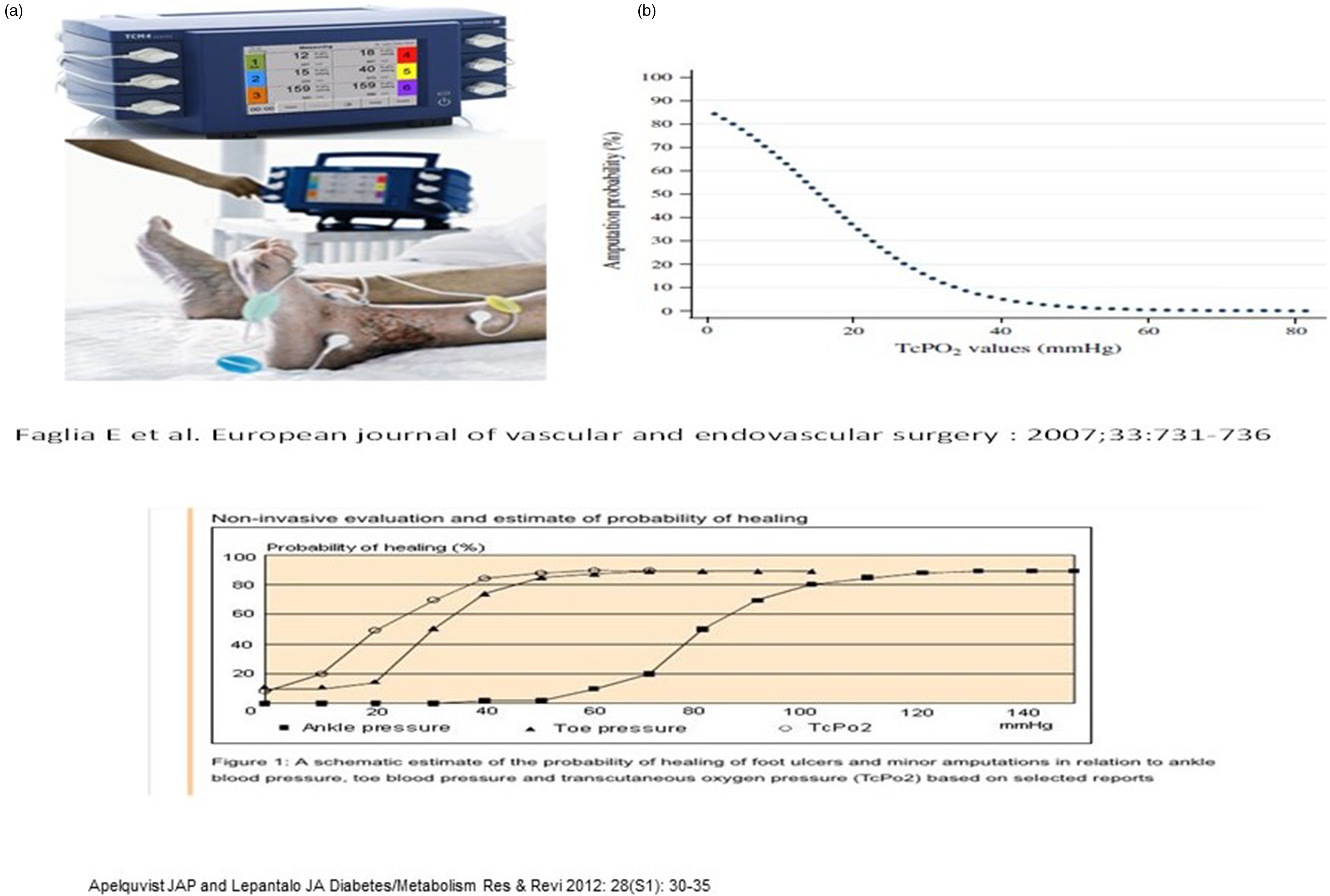
These figures show the relationships between oxygen tension, tissue oxygen saturation and ankle systolic pressure as well as the increasing probability of wound healing without amputation associated with increase tissue oxygen tension levels.
Wound Healing
It has been reported that healing times and one-year recurrence rates above 20% have not significantly advanced in the past 20 years despite the many advances in wound care and revascularization techniques.
20
Therefore, achieving optimal wound healing in the acute wound post revascularisation of the limb/tissue is challenging possibly subject to ischaemia, hypoxia, infection, and diabetes as well as smoking and age all of which impact negatively on healing/healing rates: this is relevant when referring to healing following amputation, or lesion healing post limb saving therapy. Furthermore, subsequent injuries or episodes of cutaneous ulcers de novo will also face similar challenges. Any wound care regime in this situation needs to be attentive to the need of providing the optimal conditions for healing and good wound bed preparation (WBP).
21
Key principles for best practice in WBP for the diabetic patient involve effective debridement, controlling moisture and exudate, and preventing microbial proliferation and subsequent infection. All of these clinical concepts focus on achieving viable granulation tissue formation and epithelial coverage in order to achieve full wound closure as quickly and efficiently as possible.
22
Key considerations for the clinician to consider in order to achieve optimal wound healing in the chronic wound or the acute wound post-revascularisation are :
Assess and maintain adequate perfusion: The primary surgical revascularization procedures aim to restore blood flow to the affected area, ensuring oxygen and nutrient supply to the wound. Wound assessment: Regular assessment is vital to monitor the healing process.
17
The assessment should include measuring the wound size, depth, and appearance, as well as checking for signs of infection. It could also include further assessment of blood flow effectiveness and tissue perfusion using techniques covered earlier. This regular clinical follow-up can also be an opportunity for changes, if needed, in the care plan. Wound management: This should be carried out in line with the principles of WBP. The wound should be kept clean and moist, and dressings should be changed regularly. Nutrition: Good patient nutrition and glucose control is also essential. Patient education: Educating the patient and their carers about proper wound care and how they can perform or support this while providing the necessary support and resources will help ensure optimal healing.
There are a number of advanced therapies available for wound healing post-revascularisation, which can help to promote tissue repair and regeneration if healing is stalled or if the healing trajectory is not as anticipated. It is important these are used in line with an evidence-based practice.
17
Furthermore, access to these therapies and approaches described may be constrained depending on the territory and its local regulatory and reimbursement guidelines and regulations.
23
Negative pressure wound therapy (NPWT) - this has been shown to be effective in establishing a wound environment supportive of healing in a wide variety of wound types by, first preparing it for healing and then actively promoting repairs. 24 It achieves this through suction to remove exudate and oedema hence improving tissue perfusion and stimulating granulation tissue and angiogenesis. It also reduces the bacterial load in the wound. Its effectiveness in wounds of the diabetic has been widely reviewed and considered to be of value. It should however be considered in the case of wounds such as the diabetic limb, where maintaining adequate tissue oxygenation can be difficult, that one needs to take care that the contact pressure applied as part of the NPWT therapy does not deleteriously impact either local tissue or wound blood flow. 25
Hyperbaric oxygen therapy - (HBOT) has been part of the armamentarium for treating wounds in the DF for several decades. HBOT involves the patient sitting inside a hyperbaric chamber breathing 100% oxygen pressurised between 2.0 and 2.5 ATA. 26 Duration of exposure varies from 45 min to 5 h but is typically 1-2 h. Chronic conditions may receive 30 or more treatment sessions with up to 3 sessions per day in single or multi-patient chambers. The reported benefits of tissue repair are linked to the ability of the therapy to increase the partial pressure of oxygen in arterial blood. This higher-than-normal partial pressure then can drive the improved local delivery of oxygen to tissue, enhancing neovascularization, upregulating synthesis of growth factors and other physiological effects. 27
Topical oxygen therapy (TOT) - this is a recent (relative to HBOT) innovation with the ability to deliver (non-hyperbaric) oxygen topically to a wound. In some cases, this can be humidified and/or temperature controlled. While there are several products for delivering TOT all work by generating a continuous application of pure oxygen to the wound dressing. 28 These devices can be systems in which the patient's whole limb is enclosed in a bag or chamber which can then be inflated with oxygen from either a cylinder or generator. Alternatively, they can be small, portable and battery-powered devices capable of generating their own oxygen and able to be used across healthcare settings, and can easily be taken home for use by the patient or carer. Devices can continually supply up to 15 mL/h. This establishes an oxygen gradient between the dressing and the wound bed, thereby enhancing oxygen diffusion into the tissue. Wound dressings are changed as needed weekly, and the devices (or their batteries) are generally replaced after 1-2 weeks of continuous use. These devices offer a very different and more user-friendly approach to oxygen delivery and should not be considered as portable HBOT. Recent evidence reviews suggest that the provision of TOT in diabetic foot ulcers (DFUs) was safe and associated with a higher rate of complete wound healing when added to standard of care.29,30
Topical growth factors - it is well understood that in any wound a variety of growth factors are involved in the coordination and promotion of healing. In a wound that may be in a compromised patient, such as a diabetic, then healing can be impaired. In these situations, it has been postulated that the application of topical growth factors to stimulate wound healing may be of value. 31 This has been studied clinically on multiple occasions and is the subject of a Cochrane review in which it was concluded that growth factors may increase the likelihood that people will have complete healing of foot ulcers in people with diabetes. 32 To date only two growth factors are approved by regulatory agencies globally for clinical use. The first (USA) is becaplermin, a recombinant platelet-derived growth factor (PDGF) therapy. It is approved for the treatment of lower extremity diabetic neuropathic ulcers. PDGF as the name implies is one of a family of molecules released from platelets and helps to promote the healing of wounds and to repair damage to blood vessel walls. 33 PDGF also helps blood vessels grow and initiates the chemotaxis of key cells involved in healing such as neutrophils, macrophages, smooth muscle cells and fibroblasts. It also enhances the mitogenesis of fibroblasts. The second growth factor currently approved is fibroblast growth factor (FGF). Versions of FGF (trafermin) are approved in China and Japan for use on chronic wounds and burns. FGF uses paracrine/endocrine signalling to mediate a range of processes including angiogenesis and wound healing. 34
Tissue equivalents – while patient autografting always remains as a preferred method of choice for obtaining rapid coverage and repair there are situations where this is not a clinical option. In these cases, either advanced therapies such as those described above can be considered or the use of allogeneic grafting materials. A wide range of technologies exist, some with cells and others being acellular. In 2019, it was identified that there were 74 commercially available skin substitutes to treat chronic wounds in the USA. 35 One further intervention worthy of mention is the use of autologous platelet rich plasma which is prepared from the peripheral blood of patients and has a concentration of various growth factors and cytokines. A recent meta-analysis of clinical studies 36 indicates they are safe and can be effective.
Debridement – as described earlier, good wound care depends on effective WBP and an important component of this is debridement. 21 While autolytic debridement (natural lysis, or breakdown, of eschar by the body) and surgical debridement have been traditional approaches to effective debridement other innovative and effective approaches also exist which can be both quicker and more effective. These include water jet debridement, enzymes (such as bacterial collagenase) and maggot debridement therapy (MDT) also referred to as biosurgery. 37 MDT reportedly shows a consistent positive effect in treating chronic wounds. 38
Discussion
The purpose of this article is to critique objective assessments of skin perfusion since timely, adequate levels of blood, oxygen and other essential nutrients are essential to timely healing. PAD and diabetes are increasingly found to co-exist in a cohort of patients as discussed in this group, skin/tissue healing following limb or digit saving surgery, or lesion healing of wounds, healing is unpredictable.
SPP is safely and easily measured using optical sensors. SPP exceeding 40 mm Hg is consistent with good healing: this is to say that in the circumstances obtaining, adequate levels of tissue perfusion and oxygenation are available to promote healing through wound closure as directed by tissue biology. It needs to be reinforced that underlying comorbidities, age and chronicity can and do bear upon healing times: science must model these effects. In considering the healing of lesions (chronic DFUs or ischaemic leg ulcers), non-invasive skin surface measurements of TcPO2 may be made at perilesional skin or wound edges; TcPO2 exceeding 25 mm Hg is a safe threshold: indeed, in the range of 40 mm Hg and beyond TcPO2 has been associated with a decreasing probability of amputation. This is in accord with SO2 measurements and should be used with standardised care protocols. Or it endorses an approach to standardised care. 16
The threshold of 30 mm Hg reflects capillary closing pressure. Sen reported that in the pathway to capillary formation, tissue pressure of 25 mm Hg is essential for collagen bundles to organise to develop as capillaries and may be valuable in future studies of wound healing using direct optical coherence tomography which permits perilesional capillaries to be viewed, and blood vessel density measured.39,40
Diabetes is a vascular disease, both the macro and microvascular beds may be affected. This article has focused on microvascular considerations: discussion of macrovascular imaging/measurements has been well documented.16,19 It is also addressed in another article within this special issue of the journal. Discussion of the application of thermal sensors/thermography, TV video densitometry more suitable for other applications have not adequately been described in this article.
Based on the current state of knowledge, the use of optical sensors with digital readouts would be extremely useful for use at the bedside, in-theatre, outpatient or at home use by patients. In large care settings, things with adequate infrastructure, fluorescein imaging for regional tissue viability and skin sensors for measuring TcPO2 at wound edges would be invaluable aids to clinical management which must include aids to imaging and measuring flow and vessel changes in the microcirculation.41 These and the use of advanced wound technologies should be implemented as part of standardised care of chronic wounds.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.