
Abstract
Critical limb ischemia (CLI) is the advanced stage of peripheral arterial disease, which impairs blood flow to the extremities due to occlusion of arteries, in which patients suffer from ischemic pain at rest and gangrene or ulcers. It is frequently accompanied by major adverse cardiac events, resulting in exceedingly high mortality from a cardiac or cerebrovascular event in this population. Although there have been considerable amounts of novel and costly revascularization and wound dressing technology, mortality is still high. Therefore, the risk factors for such high mortality need to be addressed. This review aimed to summarize the potential risk factors for mortality in patients with CLI of the lower extremities. There are several such risk factors, including modifiable and nonmodifiable risk factors. This review further discusses some highlighted major modified risk factors, including renal failure, cardiovascular, and diabetes. The strategy of regular surveillance and modification of such risk factors in any patients with CLI should be developed.
Introduction
Lower extremity peripheral artery disease (PAD) has been well-recognized as an increasingly global problem. A recent systematic review in 2015 estimated that 238 million people were living with PAD, most of which (172 million) lived in low- and middle-income countries. 1 In addition, the relative increase in PAD burden in developing regions is striking high and exceeds the increases in developed nations. 2 Interestingly, female gender in low- to medium-income countries is at increased risk of PAD. The result also reveals that disability and mortality associated with PAD have continuously increased over the last 20 years, which have been greater among women than those in men. 2
Chronic limb ischemia (CLI) is an advanced stage of PAD. Patients might have rest pain, gangrene, or chronic leg ulcer at this stage. Once the diagnosis is confirmed, treating CLI aims to relieve ischemic pain, heal ischemic ulcers, prevent limb loss, improve patient function and QOL, and prolong survival. Interestingly, the mortality rate in this population group is markedly high due to cardiovascular causes. After the first diagnosis of CLI, the mortality risk is 24% and reaches 60% over 5 years. 3 Based on a study by this author in 2017, 500 patients with PAD in Chiang Mai, Thailand, are followed up in 3 years; 43 patients (8.6%) die of myocardial infarction (MI), stroke, and 22 patients have either stroke or MI. 4
Although less invasive treatment and novel wound care treatment, such as endovascular treatment and hyperbaric oxygen, are the favored approaches to treating CLI, the mortality rate after treatment is still high. 5 In order to reduce mortality in such patients, the risk factors should be illustrated. This may be important in reducing adverse events, including major adverse cardiac events (MACE)/mortality, and improving patients’ quality of life (QoL). Therefore, this review aimed to summarize potential risk factors. We reviewed risk factors in the Medline database during 2010 to 2023. The reference lists in the relevant paper were reviewed. Also, we contacted to expert in this field. Firstly, there were 980 papers during keyword searching (CLI). Only 14 papers were relevant in our study about the mortality risk factors in CLI (Table 1). We discussed further some highlight factors, namely cardiovascular, anemia, diabetes, and renal insufficiency.
Factors Associated With Mortality Rate in Patient With CLI.
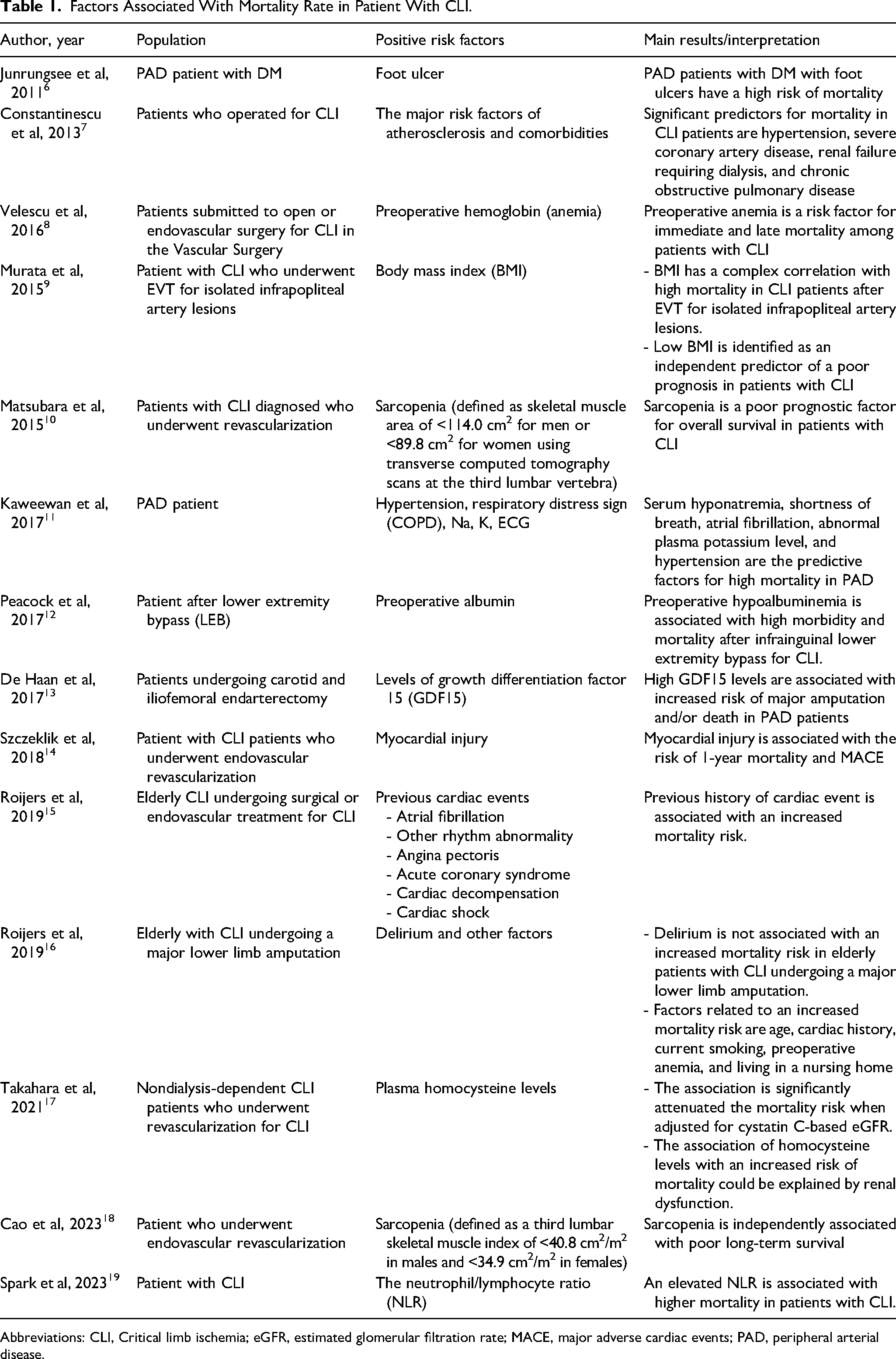
Abbreviations: CLI, Critical limb ischemia; eGFR, estimated glomerular filtration rate; MACE, major adverse cardiac events; PAD, peripheral arterial disease.
History of Cardiac Diseases
Patients with CLI are at increased risk of adverse cardiovascular events and subsequent cardiovascular death. This population also has associated with a history of coronary artery disease. Most CLI patients have advanced coronary atherosclerosis.20,21 The mortality rate within 1 year of CLI patients with a history of cardiac diseases has been reported to be 26%, reaching 75% in 10 years. 22 Adverse cardiovascular events are well known as a significant cause of major morbidity and mortality in the perioperative period in CLI patients with history of cardiac diseases. The adverse cardiac events frequently occurring after surgery are cardiac decompensation and atrial fibrillation. A previous study illustrates the 3.5 times mortality rate in patients with cardiac events occur when compared to patients without an adverse cardiac event. The most frequent adverse cardiac event is cardiac decompensation (45%), followed by atrial fibrillation (22%). Consequently, receiving cardiac evaluation before operation would be beneficial for patients with CLI who undergo endovascular treatment. 15
A retrospective study evaluates the influence of myocardial injury after endovascular treatment in CLI patients on 1-year mortality and MACE. The results illustrate that almost 25% have a myocardial injury after endovascular treatment independently associated with 1-year mortality and MACE. 14 Out of these, only 14.8% of patients show clinical symptoms or have ECG findings indicating a myocardial ischemia. Thus, routine troponin monitoring might be necessary in these patients, as opposed to symptom-initiated troponin surveillance which would result in missing most of the patients who sustain myocardial injury. 14
According to the cardiac event that caused mortality in CLI patients, the guidelines of the European Society of Cardiology/European Society of Anesthesiology recommends that the presence of ischemic heart disease should be evaluated in those patients before surgery. 23 Preoperative cardiac risk evaluation enables periprocedural cardiac measures to be applied and consequently improve cardiac outcomes in CLI patients undergoing vascular surgery.
History of Anemia
According to World Health Organization criteria, anemia is defined as hemoglobin less than 13 g/dL in men and hemoglobin less than 12 g/dL in women. 24 Anemia is a clinically important and frequent finding in surgical patients. 25 Preoperative anemia is common, ranging from 25% to 40% in large observational studies depending on the population and the definition used.26-28 The most common treatable cause of preoperative anemia is iron-deficiency anemia. Vega de Céniga et al reports that among the CLI patients over 30% have iron deficiency, and over 15% have vitamin B12 deficiency. 29 A retrospective cohort study reveals the relationship between preoperative anemia and mortality among patients undergoing surgery for CLI. Preoperative anemia has been shown to increase the risk of cardiac events and risk of both immediate and late mortality in CLI patient. 8 Consistent with previous prospective cohort study, which includes more than 900 patients with PAD undergoing surgery for CLI and claudication, preoperative anemia is found to be an independent predictive factor for postoperative death and major amputation. 29 Despite, a consequence adverse event of a low hemoglobin at preoperation such as immediate mortality and late mortality, multiple studies demonstrate a negative effect of direct perioperative transfusion. There are association between perioperative transfusion and increased postoperative mortality and morbidity, for example, transfusion-associated lung injuries, cardiac events, renal dysfunction, infections, and multiple organ failure.26,30 As mentioned before that iron-deficiency anemia is the most common in preoperation anemia, few randomized studies conduct on the role of oral iron supplementation in preoperative period. The results show an increase in hemoglobin level and a decrease in transfusion rates after the operation. However, the number of studies and the number of patients enrolled are small. 31 Hence, the best management for preoperative anemia in CLI patients still needs to explore further.
History of Diabetes Mellitus
DM is commonly found in PAD and CLI patients. DM is not only associated with a higher prevalence of PAD but also increased risk for adverse outcomes, morbidity, and mortality of PAD. 32 The atherosclerosis of cardiovascular system is the most common cause of death in diabetic patients with PAD through various cardiovascular events, such as MI, stroke, gangrene, and chronic ischemic ulcers of the lower extremities. 33 Our cohort study in 107 diabetic patients (3.5 years follow up) shows that the mortality rate in patients with ischemic ulcer is significantly higher than those without ischemic ulcer (31.9%). 6 In addition, our prospective cohort of study of 500 DM patients with PAD in Thailand, investigating prognostic factors associated with MACE, reveals that chronic kidney disease (CKD), gangrene/chronic ulcer, history of aortic surgery, and history of taking warfarin were associated with MACE in this population, with hazard ratio 2.32, 3.03, 24.07, 2.16, and 3.24, respectively. 4
History of Renal Insufficiency
Acute kidney injury (AKI), defined as an abrupt loss in renal function, is a highly complex syndrome associated with increased mortality and caused long-term renal failure after surgery.
It is well known that angiogram and endovascular treatment for occlusive lesions in CLI patients usually require the use of nephrotoxic iodine contrast. Direct toxic effects of iodine contrast on the tubular epithelium can cause postcontrast AKI (PC-AKI). 34 In addition, the risk of PC-AKI in advanced CKD patients receiving an iodine contrast is more than a 3-fold increase higher than those with normal renal function. 35 Interestingly, AKI in CLI patient appears to be a strong independent risk factor for mortality with a greater odds ratio than that of old age or heart failure.36,37 The possible mechanisms which increased the risk of mortality after AKI are both from direct pathophysiological effects of renal dysfunction and mechanisms of organ cross talk leading to multiple organ failure. The 3 physiological hallmarks of severe AKI consist of hyperkalemia, metabolic acidosis, and fluid overload may explain an increasing mortality rate in AKI. Hyperkalemia and metabolic acidosis are called metabolic abnormalities which increase the risk of arrhythmias and reduce cardiac contractility. A reduction of glomerular filtration rate in severe AKI leads to oliguria or anuria and consequently to fluid overload. 38 Acute kidney injury has been shown to have negative effects on the cardiovascular, respiratory, and neurological systems. The patients who have cardiac disease with AKI show worsen cardiovascular outcomes leading to increased rates of heart failure and MACE.39,40 An animal study demonstrates apoptosis of cardiac myocytes during AKI with simultaneous reduced cardiac output. 41 In addition, altered cytokine profile circulation may directly damage cardiac myocytes.42,43
Acute kidney injury is independently associated with a progressive deterioration of renal function, which can lead to CKD as well as end-stage renal disease (ESRD) and a decreased in the QoL.43,44 A mortality risk in patients with CLI is increased with the severity of CKD (stage of CKD) especially in the ESRD. A recent meta-analysis investigates the impact of renal function on the outcome after surgery. The results reveal that an estimated glomerular filtration rate less than 60 mL·min·1.73 m−2 was associated with a 3-fold increased risk of death and AKI within 30 days of surgery. 45 Moreover, several studies also report a mortality of about 10% in CLI patients with ESRD after revascularization.46,47
Management of Risk Factors Modification in CLI
According to the absence of identification and treatment in the risk factors of comorbid conditions, the prognosis of CLI patients is poor as indicated by a high mortality rate range from 20% to 26% within 1 year after diagnosis.48,49 Recently, the goal treatment of CLI condition is revascularization to salvage a functional limb. However, there has been a high rate of MACE and mortality rate after revascularization. Previous evidence also reports that the risk factors, including nonmodified factors (age and sex) and modified factors (hyperlipidemia, hypertension, diabetes, and smoking), are related to the development of MACE and the reduction of survival rate. Therefore, the prevention/modification of these aggressive risk factors is of paramount importance.
Currently, a global vascular guideline on the management of CLI in 2019 suggests the application of metabolic-lowering agents such as antithrombotic, lipid-lowering, antihypertensive, or glycemic control agents in CLI patients to decrease rates of major amputation and increase patency after revascularization. 50 Following aggressive risk factor controls in aspirin used, statin medications, ACE inhibitors, and smoking abstention, data reveal significantly a 36% reduction in MACE, a 45% reduction in major adverse limb events, as well as a 44% reduction in mortality rate within 3 years among CLI patients. 51 A growing body of literature indicates alternative drugs to aspirin, such as ticlopidine, dipyridamole, and clopidogrel, may be more effective.52-54 The Clopidogrel versus Aspirin in Patients at Risk for Ischaemic Events (CAPRIE) trial reveals an 8.7% decrease in MACE in patients with PAD receiving clopidogrel compared with aspirin. 54
Conclusion
Critical limb ischemia patients are at risk of high mortality, even though there has been a considerable amount of high technology in revascularization techniques and novel wound care. Various risk factors are associated with high mortality in patients with CLI in the literature. Although some factors are nonmodifiable, physicians need to focus on any modifiable risk factors intensively according to the guidelines to reduce mortality. Some factors like CLI with a history of cardiac disease or anemia or renal insufficiency or diabetes are becoming a deadly combination. The strategy of regular surveillance and modification of such risk factors in any patients with CLI should be developed.
Footnotes
Acknowledgments
This project was partially supported by Chiang Mai University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.